
Abstract
Abstract
Background:
The groin surgical site is frequently infected in vascular surgical procedures. Our aim was to evaluate the relation of skin closure methods and groin incision infection after vascular operations involving femoral artery exposure.
Methods:
In this retrospective patient record study, patient files of all consecutive patients admitted for a vascular procedure to the Turku University Hospital Department of Vascular Surgery during 2015–2016 were evaluated. Patients with an isolated groin surgical site because of femoral artery exposure (256) were included in the study. Patient demographics, details of the operations, and follow-up data were collected from the electronic patient data record. Statistical analyses were performed using a multi-variable model.
Results:
Altogether, 330 groin incisions were performed for 256 patients. Of all incisions, 262 (79.4%) were closed using intra-dermal absorbable suture; trans-dermal sutures were used in 68 (20.6%) incisions. Groin infections occurred in 24 (9.2%) patients after skin closure with intra-dermal absorbable suture and in 17 (25.0%) cases after trans-dermal sutures. Incisions that were closed using trans-dermal sutures were 3.5 times as likely to have an infection as those closed using intra-dermal sutures (odds ratio 3.5, confidence interval 95% 1.6 to 7.6, p = 0.002).
Conclusion:
Present data suggest that groin incision closure with intra-dermal absorbable suture is associated with groin incision infections compared with those incisions closed with trans-dermal sutures.
T
The surgical sites, including femoral artery exposure in vascular operations, are closed traditionally using trans-dermal closure techniques—i.e., metal staples or traditional non-absorbable sutures. A Cochrane review on skin closure techniques concluded that wound dehiscence may be reduced by using sub-cutaneous absorbable sutures [12]. This sub-cutaneous closure method is adopted widely in plastic surgical procedures.
Because the possible association between the vascular groin incision closure method and groin surgical site infection has not been reported earlier, the aims of the present retrospective study were to evaluate the possible relation of skin closure method and groin surgical site infection.
Methods
All consecutive vascular surgical patients operated on in the University Hospital of Turku in the two-year period between January 1, 2015 and December 31, 2016 were screened. Patients with solely a groin incision for femoral artery exposure—e.g., femoral endarterectomy, embolectomy, femoral access for endovascular aortic repair (EVAR), etc.—were included in the study. Also, patients who had undergone femoro-femoral bypass procedures were included as well as femoro-popliteal bypass procedures where a prosthetic graft was used. The exclusion criteria were that the groin incision was not a part of a vein harvesting surgical site (i.e., bypass procedures with harvested saphenous vein). In addition, operations because of puncture site hematomas were excluded from the present study.
The pre-operative skin wash was performed according to the hospital's guidelines using denatured ethanol. Antibiotic agents were administered 30–60 minutes before incision, and an extra dose was administered after three hours. Cefuroxime was the first choice of prophylactic antibiotic agent.
Data were collected from the operation monitoring system Opera™ (GE Medical) and the patient record system Uranus (CGI). A part of the patient information was collected for quality control purposes prospectively. Additional data were recorded to this data file retrospectively between January and March 2017.
The following patient related data were recorded: age, gender, diagnosis, and body mass index (BMI) of the patient, peripheral artery disease (PAD), presence of critical limb ischemia (CLI), hypertension, diabetes mellitus, rheumatoid arthritis, and smoking.
Operation related data included indication and urgency of the operation. The incision closure method was entered in the file. The incision closure method for each operation was not pre-determined; the wounds were closed according to each surgeon's preferences.
Infection was detected after operation, and it was recorded during the first 30 days after operation according to the Szilagyi classification of vascular surgical site infections. The follow-up data were collected from the outpatient control visits and emergency care unit electric data files covering all hospitals in the South-West region of Finland.
For the statistical analyses of infections, each surgical site was considered separately. The four-category variable “wound closure method” was classified further to a binominal variable. Metal staples, continuous trans-dermal suture, and interrupted trans-dermal suture using polyamide suture material (Ethicon, Ethilon II™) were combined as trans-dermal wound closure. Intra-dermal absorbable suture using poliglecaprone 25 suture (Ethicon, Monocryl™) was classified as intra-dermal wound closure.
Continuous variables were characterized using means and standard deviations for normally distributed variables and in case of categoric variables, frequencies and percentages were used. Normality of distribution for continuous variables was tested with the Shapiro-Wilk test. Variables were compared with independent sample t test as variables at each group were distributed normally.
A multi-variable logistic regression model, where subject was taken into account (GEE-model) was used to analyze the data. The final model included the following variables: Skin closure technique, diabetes mellitus, critical limb ischemia, gender, age, and BMI. Two-sided tests were used and p values <0.05 were considered statistically significant. Statistical analyses were performed using the SAS System for Windows, Version 9.4 (SAS Institute Inc., Cary, NC) and IBM SPSS Statistics program (version 23).
Results
Characteristics
A total of 256 patients were operated on and 330 groin incisions were performed. For 74 patients, the groin incision was bilateral. Characteristics of the patients and procedures are presented in Table 1.
Characteristics of the Patients and Performed Operations Divided into Two Groups According to the Incision Closure Technique
SD = standard deviation; BMI = body mass index; PAD = peripheral artery disease; CLI = critical limb ischemia.
Continuous variables were characterized using means and standard deviations for normally distributed variables, and in case of categorical variables, frequencies and percentages were used.
P-Value calculated with Pearson chi-square test for non-continuous variables and with the Mann-Whitney U test for continuous variables.
The most common indication for operation (152 wounds, 46.1%) was arterial aneurysms; these included elective abdominal aortic aneurysms and iliac artery aneurysms as well as ruptured aneurysms. In most of these cases, the incisions were bilateral; 144 incisions (43.6%) occurred because of PAD. The rest of the patients (34 wounds, 10.3%) were operated on because of arterial embolus (Fig. 1.). Altogether 76 incisions were performed in urgent operation settings, of these, 46 (60.5%) were closed with trans-dermal sutures (Table 1).
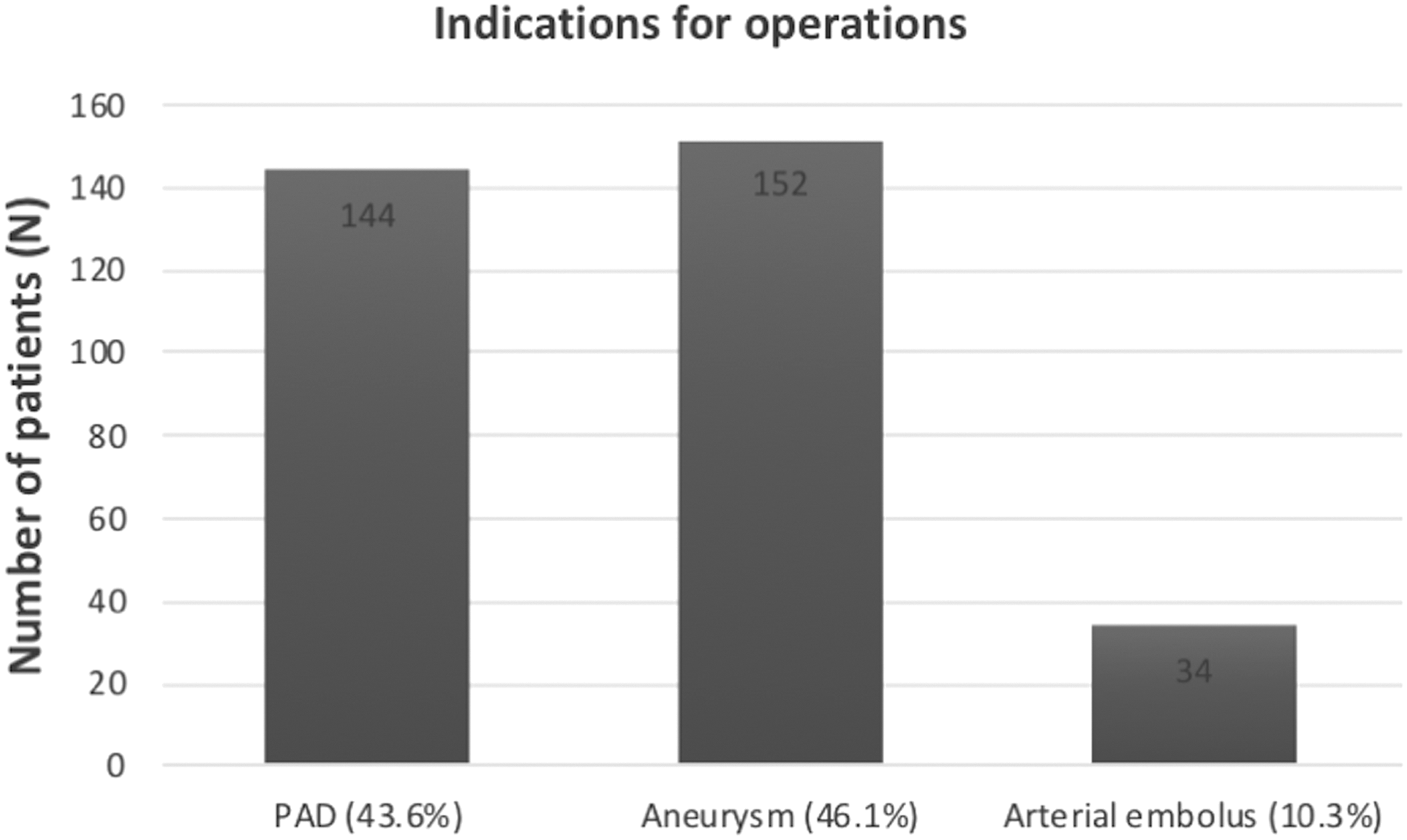
Indications for operations. Total number of patients was 256; 330 incisions were performed. PAD = peripheral artery disease.
The majority (262, 79.6%) of groin incisions were closed using intra-dermal absorbable sutures, and 68 (20.4%) were closed using skin trans-dermal closure methods. Of these, metal staples were used most frequently; other closure methods were interrupted polyamide suture and running polyamide sutures. In hybrid and EVAR procedures, 90.5 % of the incisions were closed using intra-dermal absorbable sutures, while in 59.6% of other operations with femoral artery exposure, intra-dermal absorbable suture was utilized. Closure methods are presented in Figure 2.
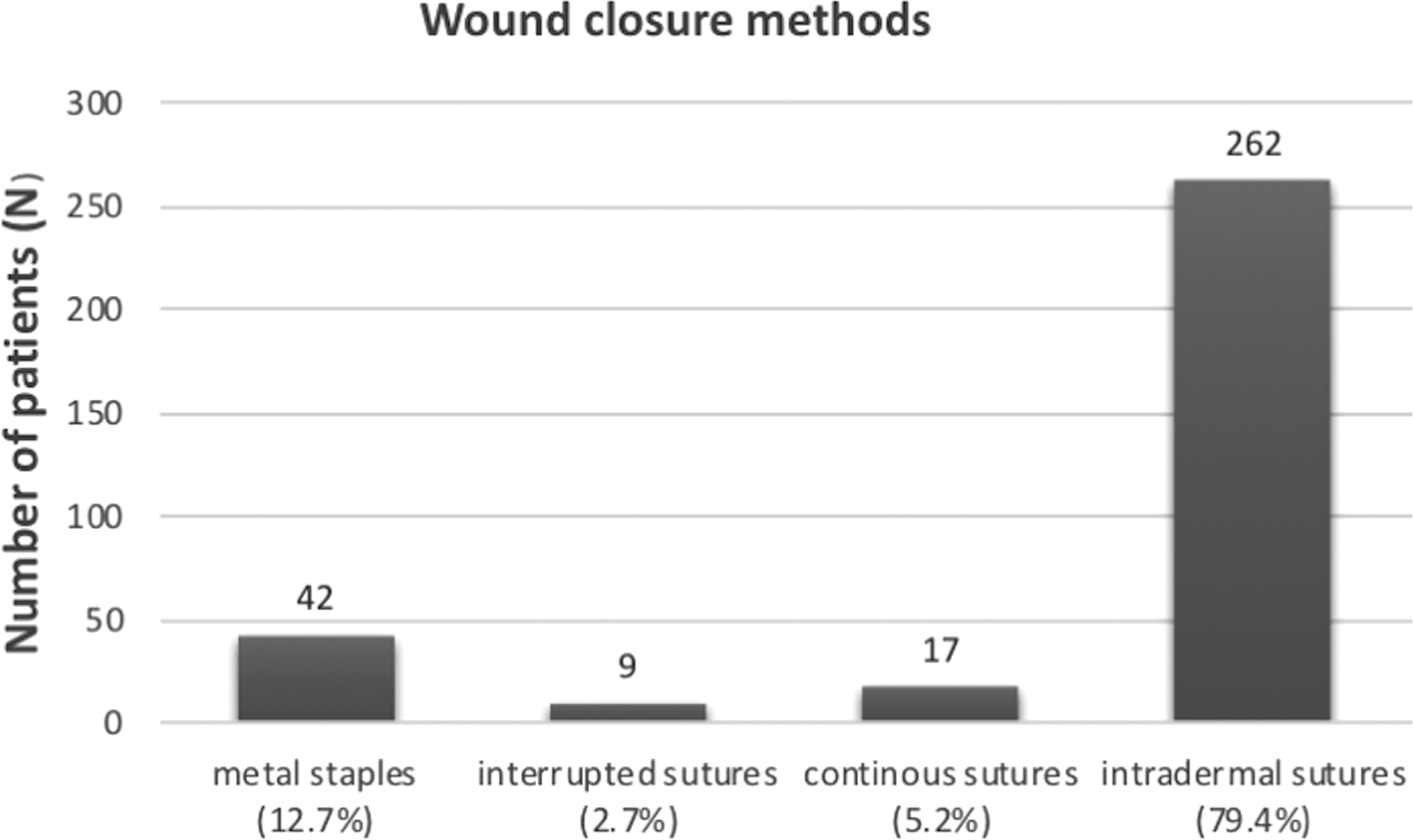
Incision closure methods. Total number of patients was 256; 330 incisions were performed.
The peri-operative death rate (<30 days from operation) was 3.9%. All causes of death were of cardiovascular etiology. The mean operative time for the non-infected surgical sites was 140 minutes (95% confidence interval [CI] 132–148) and 131 minutes (95% CI 114–148) for the infected sites. These differences in operative times were not found to be statistically significant.
Infections
Altogether, 41 (12.4%) surgical site infections were observed. In the intra-dermal closure group, the number of infections was 24 (9.2%) while in the trans-dermal group, this number was 17 (25.0%) (Table 2). After trans-dermal closure, site infection occurred 3.5 times as likely as after intra-dermal closure (odds ratio [OR] 3.2 CI 95% 1.6–7.6, p = 0.002). The results of the statistical analysis are presented in Table 3. Altogether, 10 (3.0%) deep infections (Szilagyi grade II and III) were recorded. According to micropathology, the following pathogens were present in these sites: Staphylococcus aureus (four), Escherichia coli (two), Pseudomonas aeruginosa (one), and Streptococcus agalactie (one). The rest were mixed infection with S. aureus, E. coli, and Enterococcus fecalis.
Numbers and Percentages of Surgical Site Infections According to Studied Risk Factors
N = number of wounds; CLI = critical limb ischemia.
Patient-Related Risk Factors and Incision Closure Method in Relation to Incision Infections
OR = odds ratio; CI = 95% confidence interval; BMI = body mass index; CLI = critical limb ischemia.
A multi-variable (GEE) model was used to analyze the data.
Total number of groin incisions was 330.
Discussion
The present study showed a lower number of groin incision infections after femoral artery exposure when the skin was closed using intra-dermal absorbable sutures compared with trans-dermal sutures. This result supports our hypothesis that the risk for infections can be reduced with intra-dermal closure of the groin incision.
The observed rate of groin surgical site infections was 12.4%. This figure is in line with earlier reported rates from 5% up to 27% [3–7]. The high incidence of infection after peripheral vascular operation compared with other clean surgical procedures is both procedure and patient related. Procedure-related risks include long operative time related to hypothermia, inadequate antibiotic prophylaxis, and breaks in sterility [13]. Patients undergoing a surgical procedure for PAD are often frail and typically have multiple co-morbidities. Co-morbidities predispose vascular surgical patients for development of post-operative complications including surgical site infections. The post-operative risk is generally associated with cardiovascular risk factors, degree of ischemia in the operated limb, and operative method [14–16]. In the present study, diabetes mellitus, critical limb ischemia, and high BMI were not significantly over-represented in the infection group (Tables 2, 3).
The infection occurs primarily as a result of contamination by skin organisms during or right after operation [1,2]. The most frequent pathogenic bacteria encountered in surgical incision infection are gram-positive cocci (e.g., S. aureus and streptococci) [17]. Both of these bacteria colonize normal skin, but when they penetrate into the tissues, they can cause infections. Our hypothesis is that if the skin is closed using intra-dermal sutures, a tighter barrier is created and bacterial infiltration deeper into the tissues can be reduced. The Cochrane review concluded that wound dehiscence may be reduced by using continuous sub-cutaneous sutures [12]. Our result with a reduced number of infections supports this. Although the intra-dermal technique could be considered more laborious to perform, it may promote better healing of the site.
This was a retrospective, single center study with a relatively small cohort. The incisions were closed according to the operator preferences, and no randomization was performed. It was notable that non-absorbable sutures were more often used in urgent operations, while in elective operations and hybrid operations, the skin was more often closed using absorbable sutures. Patient selection in each group, however, was evenly divided considering common risk factors for surgical incision infection (Table 1.).
Conclusion
Present observations suggest that groin incision closure with intra-dermal absorbable suture is associated with fewer infections of the groin in vascular surgical patients. Further randomized trials are needed to confirm this finding.
Footnotes
Author Disclosure Statement
No competing financial interests exist.