
Abstract
Abstract
Background:
Group A streptococcal infections are a major cause of benign and deadly human infections with their most destructive manifestation taking the form of necrotizing soft tissue infections (NSTIs) and toxic shock syndrome.
Discussion:
The mainstays of treatment have not changed since antibiotic agents were added to the standard of early diagnosis and aggressive surgical debridement, and the mortality rate continues to be staggering. In the age of targeted medicine, there is undoubtedly a need for a more precise approach to treating this spectrum of aggressive diseases.
Conclusion:
This review covers the basic biology and clinical presentation of NSTIs and group A streptococcal sepsis with particular attention to novel treatments that may transform care and outcomes.
G
This review highlights the epidemiology, clinical manifestation, and microbiology of NSTIs caused by group A streptococcus. We also outline the current approach to treatment and examine how novel adjuncts, such as immune-modulating proteins and intravenous immunoglobulin (IVIG), are being explored for the treatment of invasive group A streptococcal (iGAS) infections.
Epidemiology
Although iGAS infections are relatively common in the hospital and outpatient settings, NSTIs are rarely encountered. There are estimated to be 1,000–1,500 cases of diagnosed NSTIs in the United States annually at a rate of 0.04 cases per 1000 person years, but this number appears to be increasing [6,7]. This trend is partially because of increased incidence reporting, but there has also been a three-decade–long increase in the global burden of iGAS infections, which may also contribute to the higher incidence of NSTIs [1]. Patterns of NSTI incidence among populations in the United States have largely revealed no noteworthy trends, but there do appear to be higher rates in patients with diabetes mellitus, obesity, and peripheral vascular disease as well as clustering of affected populations and bacterial causes by geographic location [8]. Although most clinicians will see few cases of NSTI throughout their entire career, tertiary referral centers where NSTI care is becoming centralized are now testing grounds for advancements in therapy.
Clinical Presentation
As evidenced by the diversity of names used to describe NSTIs in the days of early medicine, its clinical presentation varies widely. The most common site for GAS NSTI is the extremities, but NSTIs can occur in any body area. They are difficult to identify because they can initially involve deep tissues while maintaining normal-appearing overlying skin. Necrotizing soft tissue infections often emanate from a site of skin trauma such as a diabetic ulcer, animal bite, intravenous drug use site, or surgical site and progress rapidly from a localized skin infection to sepsis and toxic shock. Because the initial presentation can be obscure and the progression rapid, early diagnosis is challenging and the consequences of every hour delay result in increased tissue loss, limb loss, and mortality [9,10]. Often the earliest clinical features are pain out of proportion to examination, pain upon active and passive range of motion, and epidermolysis. Diagnosis is then based on a combination of clinical presentations including rapid chronology of symptoms, laboratory markers summarized in a Laboratory Risk Indicator for Necrotizing Fasciitis (LRINREC) [11] score, and ultimately operative exploration.
Microbiology
The causative agents of NSTIs are various combinations of gram-positive and gram-negative bacteria. The most popular classification proposed by Giuliano et al. [12] in 1977 describes type I NSTIs as polymicrobial; these account for approximately 60% of NSTI cases and tend to involve the perineum and trunk of older comorbid patients. Type II NSTIs are monomicrobial, usually because of GAS and less frequently staphylococcus. They often occur in younger, healthier patients and spread aggressively and systemically, probably as a result of expressed exotoxins. Type III NSTIs are caused by marine organisms, most commonly Vibrio vulnificus and are rare. Importantly, there has been no demonstrated difference in clinical course and mortality have among these subtypes [12,13].
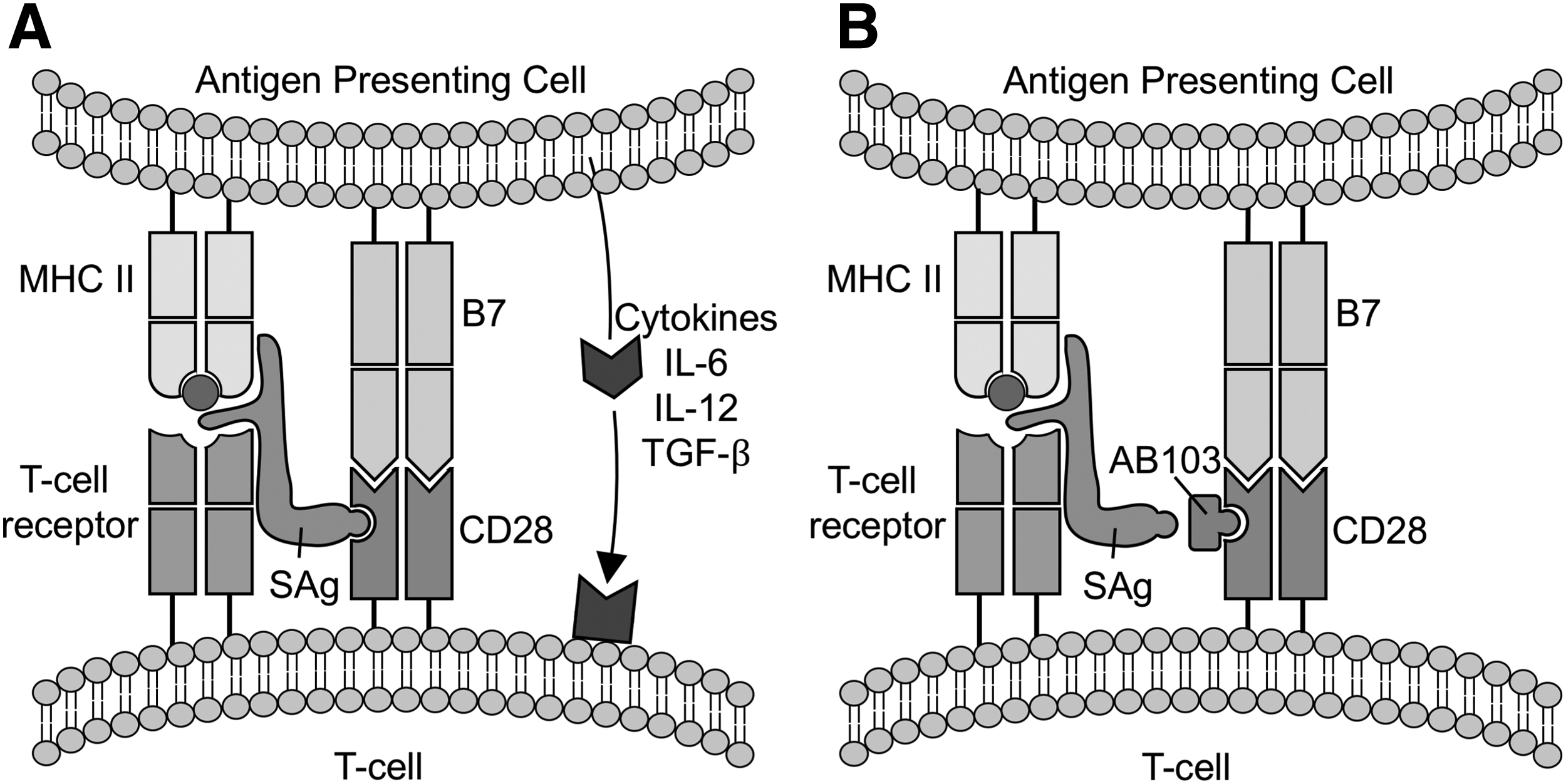
One of the most important features of NSTIs is the rapid progression to systemic toxicity. In the case of tissue invasive strains of Streptococcus and Staphylococcus, the mechanism responsible for this is toxic shock syndrome resulting from expression of superantigen (SAg) exotoxins [14,15]. Superantigens hyperstimulate the immune response by hijacking the normal major histocompatibility complex II (MHC-II) and T-cell receptor communication axis (Fig. 1). Superantigen binds the outer face of MHC-II and T-cell receptor at sites not ordinarily involved in antigen presentation, thereby bypassing the normal internal processing by antigen-presenting cells. In addition to interaction of MHC-II with the T-cell receptor, the adaptive immune response requires co-stimulation by CD28 on T-cells with B7 on antigen-presenting cells (Fig. 1). Superantigen has a peptide sequence that is well conserved across all staphylococcus and streptococcus species and binds CD28. By coordinating the interaction of MHC-II with the T-cell receptor and activating the CD28 molecule, superantigens hyperstimulate the T-cell–mediated immune response [16].
(
Standard of Care
The standard of care in NSTIs is based on source control through operative debridement and broad antimicrobial coverage for invasive and disseminated infection. In sepsis, antimicrobial coverage without source control is ineffective [17]. In order for antimicrobial agents in conjunction with the host immune system to be successful in fighting an infection, the inoculum size must be reduced quickly. The best way to achieve this in an NSTI is through early, wide surgical debridement. Antimicrobial coverage should initially be directed broadly to include gram-positive, gram-negative, and anaerobic organisms with particular emphasis on Staphylococcus, Streptococcus, and Clostridium species. Therefore, acceptable regimens should be multi-drug and may include a penicillin for gram-positive organisms including invasive species of GAS, vancomycin, linezolid, or daptomycin until methicillin-resistant Staphylococcus aureus (MRSA) can be excluded; clindamycin for inhibition of toxin production; and a broad-spectrum agent such as piperacillin-tazobactam or a fourth-generation cephalosporin for drug-resistant gram-negative organisms. Numerous alternative regimens exist, but these major classes of microbial coverage should guide antibiotic choice. The duration of antimicrobial treatment may be reduced with culture results, resolution of sepsis physiology, and most importantly adequate source control with no further need for operative debridement. These pillars of NSTI treatment have existed for more than half a century, yet we have only made small improvements in survival. As result, adjuncts to the antimicrobial and operative foundations of NSTI management are an area that require further exploration.
Novel Therapies
As discussed previously, the cornerstones of NSTI treatment are wide operative debridement concurrent with broad antimicrobial coverage. However, this strategy has resulted in only modest improvements in survival since the time of Dr. Joseph Jones during the Civil War. Because mortality in iGAS is driven by end-organ failure and multi-system collapse, there have been a handful of studies directed at curbing the systemic toxicity of local tissue infection.
Immune-modulating peptides
Rational design of molecules to antagonize immune cell communication is a relatively new strategy. In toxic shock caused by secreted SAgs of Staphylococcus and Streptococcus species, the SAg binds both the MHC-II molecule on antigen-presenting cells and the β chain of the T-cell receptor at regions not normally involved in antigen recognition [15,18]. In contrast to normal antigen presentation that requires internal antigen processing and stimulates approximately 0.2% of T cells, SAgs bypass processing by antigen-presenting cells and stimulate approximately 30% of T cells, causing massive upregulation of inflammatory T-helper cells and of interleukin-2 and tumor necrosis factor-α cytokine production. Treatments aimed at inhibiting the downstream cytokine production that results from SAg stimulation have failed in prior STSS studies [19].
AB103, also known as Reltecimod, is an experimental drug that was developed as an alternative approach, namely, targeting the interaction of SAg with cell receptors at the onset of the inflammatory cascade. AB103 works by mimicking the SAg peptide sequence that binds the costimulatory molecule CD28 (Fig. 1). Both Staphylococcus and Streptococcus SAgs have a highly conserved distal sequence that binds and stabilizes the CD28 costimulatory molecule required for all T-cell activation. When this SAg-CD28 interaction is disrupted, mice are protected from the lethal effects of SAg [20]. Moreover, when AB103 was studied in a murine model of NSTI caused by GAS, there was dose-dependent improved survival and reductions in muscle inflammation and cytokine levels [16]. This paved the way for studies in human beings, which are ongoing.
The phase 2 study of AB103 was the first prospective study of an investigational drug for the treatment of NSTI. With 43 patients enrolled, it demonstrated safety and dramatic dose-dependent improvements in organ dysfunction based on Sequential Organ Failure Assessment (SOFA) scores at 14 days [21]. The subsequent phase 3 trial, ACCUTE (AB103 Clinical Composite Endpoint Study in NSTI) is currently underway with a planned enrollment of 290 patients to assess efficacy.
Intravenous immunoglobulin
In contrast to new efforts to deliberately design modulators of cell-mediated immunity, the theory of harnessing non-specific passive immunity has been proposed for iGAS infections for more than 20 years. The principle has been that infusion of polyspecific immunoglobulin G (IVIG) acts at multiple levels in the innate and adaptive immune system (Fig. 2) and in particular inhibits the activity of streptococcal and staphylococcal virulence factors [22]. Whereas surgical debridement and antimicrobial coverage have remained the backbone of treatment, some centers have reported adjuvant use of IVIG [23]. Nevertheless, strong clinical evidence to justify its use in iGAS, STSS, and NSTI has not been shown. The first and only placebo-controlled, double-blinded randomized trial for IVIG in STSS was conducted by Darenberg et al. [24] in 2003 and was prematurely terminated after enrolling 21 patients because of low patient recruitment (Table 1). The outcomes of the study showed statistically insignificant difference in survival between the groups but trended toward improved SOFA score and reduced mortality. Therefore, the justification for clinical benefit in humans is limited to case reports and several prospective observational studies comparing matched patients who received IVIG and those who did not (Table 1). These demonstrated variable 28- or 30-day survival in patients receiving anywhere from 0.5–2.0 g/kg pooled IVIG. Taken together, these studies were relatively small, involved heterogeneous case types, and showed no conclusive mortality benefit to IVIG. The largest and most definitive study for the use of IVIG in the NSTI population was a retrospective cohort study in vasopressor-dependent and surgically debrided NSTI patients conducted by investigators of the National Institutes of Health and several high-volume critical care centers [25]. Of approximately 12,000 patients with diagnosis of NSTI, 161 IVIG patients across 61 centers were propensity matched to 161 non-IVIG patients and their outcomes compared. No impact on mortality or hospital length of stay (LOS) was found between the groups. More detailed analysis revealed that even when IVIG was administered early (within the first two days of diagnosis), there was no mortality or LOS benefit.

Actions of intravenous immunoglobulin during streptococcal infection. IVIG is a therapy of pooled, polyspecific, and polyclonal human IgG that works at many levels in the immune system. It activates components of innate immunity by coating and targeting bacteria for phagocytosis as well as recruiting complement, which forms pores in the cell wall resulting in bacterial lysis. IgG can also directly bind and neutralize cytokines and toxins. Finally IgG binding to B and T-cells modulates the adaptive immune response. Sag = superantigen; IgG = immunoglobulin G.
Trials of Intravenous Immunoglobulin G in Streptococcal Toxic Shock Syndrome and Necrotizing Soft Tissue Infection
IVIG = intravenous immunoglobulin G; STSS = streptococcal toxic shock syndrome; IgG = immunoglobulin G; iGAS = invasive group A streptococcal infections; RCT = randomized controlled trial.
Challenges and Conclusions
The ongoing challenge of improving our treatment of NSTI and sepsis caused by iGAS is underscored by the substantial morbidity and mortality. Thoughtful and aggressive surgical management of the disease has only taken us so far in minimizing the systemic toxicity caused by secreted bacterial proteins, which are ultimately responsible for organ failure and death in these patients. Efforts to study this disease will continue to be challenging because of the broad spectrum of clinical presentation, difficulty enrolling patients, and a lack of powerful pre-clinical models with which to test therapies. In retrospect, the successes of IVIG as a substitutive therapy in primary and secondary immunodeficiencies [26] compared with its relative failure in patients with NSTI and iGAS with intact immune systems is perhaps not unexpected. However, we should be encouraged and excited by the frontier of precision therapy to identify specific targets to mitigate the impact of these organisms and their toxins on the immune response.
Footnotes
Author Disclosure Statement
D.M. has no relations to disclose. E.B. was a former consultant for AtoxBio LTD, which manufactures AB103 and is currently the lead investigator of the phase 3 study of AB103 for which her institution receives grant support.