
Abstract
Abstract
Background:
Glove perforation is common during surgery. Surgical gloves are used as personal protective equipment to reduce infection risks from bloodborne pathogens for both the surgical team and patients. This research was conducted to determine the perforation rates of gloves worn in open abdominal surgery performed in a general surgery department and the risk factors affecting perforation.
Methods:
This research was designed as an observational prospective cohort study including 70 open abdominal operations. There were four members of the surgical team (surgeon, first assistant, second assistant, and scrub nurse). A total of 280 (70 × 4) pairs of gloves in 70 consecutive open abdominal procedures were included in this study. A total of 140 unused gloves were tested as control group to assess perforations and pre-existing leaks. After the operation, all gloves were checked for water impermeability using the EN455-1 method and the presence or absence of a puncture hole was recorded.
Results:
Glove perforation was detected in 54.3% of operations. The rate of perforation in all gloves was 10.7%, of which 78% unnoticed by the surgical team during surgical procedure. It was determined that the puncture in the gloves was mostly on the non-dominant hand (left). For the left-hand glove, the highest number of holes was observed on the index finger (21.1%) and palm/dorsum of the hand (21.1%). The risk of glove perforation was 5.8 times greater for surgeons compared with the other team members, and operation time of 61 minutes or longer increased the risk of perforation by 12.77 times.
Conclusions:
Glove perforation rates are high in open abdominal surgery. The highest number of perforations occurred in the non-dominant hand (left) has a high rate of perforation in surgeons and long operations. It may be beneficial for surgical team members to change gloves at certain intervals during surgery or use indicator glove systems.
Surgical gloves were first used toward the end of the nineteenth century by William S. Halsted's nurse to protect from dermatitis [1]. At that time, gloves were only used to protect the surgical team from infections, but today personal protective equipment is also used for the safety of the patient [2]. The punctures and tears caused by sharp instruments such as surgical needles, scalpels, and scissors in gloves used during surgery negatively affect the aseptic environment [3]. As a result of glove perforation, both the patient and the surgical team members face the risk of contamination, and micro-organisms can pass from the team to the patient and vice versa. Exposure of infected patients to blood or body fluids increases the potential for transmission of infections, such as hepatitis B, hepatitis C, and human immunodeficiency virus [4]. In addition, surgical site infections were found to be more frequent during surgery in which glove perforation occurred [3,5]. Surgical gloves were shown to prevent transmission of micro-organisms from the patient or the hands of the surgical team [3,4,6].
It has been reported that glove perforation rates varied depending on the type of operation, the experience of the surgeon, and operation time. It has also been demonstrated that during surgery, exchange of surgical equipment between the team members, frequent use of sharp instruments, and use of scalpel and needles increase glove perforation rates [3,7].
In studies investigating glove perforation, the rate of perforation also varies depending on the type of surgery, e.g., 4.7% in total knee and hip arthroscopy [8], 21.4% in major plastic surgery [9], 93% in oncologic gynecologic surgery [10], 15% in orthopedic surgery [11], and 4% in ophthalmic surgery [12]. Furthermore, for colorectal surgery, the glove perforation rate was 27.3% and 15.37% in operations longer and shorter than 60 minutes, respectively [13]. Although there are numerous studies in the literature on the perforation of sterile gloves, only a limited amount of research has been undertaken to investigate the perforation of gloves used in open abdominal operations in Turkey. This research was undertaken to determine the perforation rates of gloves used in open abdominal operations performed by the general surgery department and the risk factors affecting perforation. The results are expected to contribute new data to the literature by the determination of glove perforation rates.
Methods
Research design
This was an observational prospective cohort study.
Setting and samples
This study was conducted between March and October 2016 in a university hospital operating room in the west of Turkey. The sample size was calculated using minimum (4.2%) and maximum (23.5%) perforation rate of gloves reported in Çalışkan et al. [13] as a reference. The minimum sample size was determined as 60 operations with a power of 80%, α = 0.05 error, and 95% confidence interval. A total of 280 pairs of surgical gloves (560 single gloves) used in 70 adult open abdominal operations were searched for hidden perforations and related issues in this study. None of the surgical team members wore double gloves. A total of seven surgeons, seven first assistants, 50 second assistants, and 10 scrub nurses participated in this study. If any glove was found to be visibly punctured, it was immediately replaced with a similar glove. Seventy unused pairs of gloves were tested as the control group. The right hand was the dominant hand for all team members. The type and size of the gloves were selected according to the personal preference of the surgical team members.
The operations were evaluated in two groups of 60 minutes or less and more than 60 minutes. In addition, gloves used in surgery were divided into 60 minutes or less and more than 60 minutes according to the usage time. The research included Beybi® (Beybi Plastik, Istanbul/Turkey), single-coat, barrier, sterile surgical gloves. Gloves perforated while being worn were not included in the study. Surgical gloves that were perforated during wearing after scrubbing were not included in the study. Gloves worn after being changed for any reason were also excluded from the study.
A plastic box was placed in the operating theater for the participating surgical team to place their used gloves. In order to obtain sufficient correct data, the gloves were collected in plastic bags labeled with identification information. The gloves were individually labeled and placed in marked numbered plastic bags. At the end of each day, the researcher collected all the study gloves from the plastic box. Only one pair of gloves used by each surgical team member for each procedure was included in this study. Gloves of each member of the team were placed in separate boxes.
The glove perforations were evaluated against the following parameters: (1) whether the gloves worn by the surgeon, assistants, or scrub nurse had a perforation, (2) duration of surgery, and (3) site of perforation. Furthermore, after each operation, the gloves were tested by the approved standardized water leak test method EN455-1 (European Committee for Standardization).
According to the EN455-1 method, the gloves were filled with 1,000 ± 50 mL of water at a temperature of 15°–35°C. The water-filled gloves were observed for two minutes, and the location of the leak was marked on the prepared form. The left-hand little finger, a; the right-hand little finger, j; left hand back, k; right hand back, l; left palm, m; right palm, n; and the holes were recorded in this order. The same researcher undertook all the procedures.
Statistical analysis
SPSS 15.0 (SPSS Inc., Chicago, IL) was used for the evaluation of the data in the study. The descriptive statistics included mean and standard deviation, median (interquartile range [IQR]), and minimum and maximum values for continuous variables, and number and percentages for categorical data. The univariate analyses of the data were undertaken using the Mann-Whitney U and χ2 tests. For multivariable analysis, a logistic regression model was constructed for the presence of perforation in gloves. The values that were found to affect glove perforation in univariable analyses were included in this model and tested. The findings were expressed as Exp (B) (95% confidence interval [CI] values and odds ratio (OR) (95% CI). The significance level was accepted as 0.05.
Ethical consideration
The study was approved by the Scientific Ethics Committee of Medical School (reference number 09.03.2016/20478486- 81). All surgical team members gave their written and verbal informed consent.
Results
The characteristics of the surgical team members are given in Table 1. Of the surgical team members who participated in the study, 55.4% were female, 9.46% were surgeons, 9.46% were first assistants, 67.57% were second assistants, and 13.51% were scrub nurses. The mean duration of surgical experience in years was 10.7 years ±9.7 for the surgeons, 5.3 years ±3.7 for the nurses, 4.9 years ±7.13 for the first assistants, and 0.6 ± 1.38 years for the second assistants (Table 1).
Characteristics of the Surgical Team Members
One participant was involved in more than one surgery.
SD = standard deviation; Min = minimum value; Max = maximum value.
In this study, the number of surgical operations (70 cases) in which at least one glove hole was identified was 38 (54.3%), and 18.4% of these operations were for inguinal hernia repair. The perforation rates for the non-dominant (left) gloves of the surgical team members were 30% for surgeons, 8.6% for scrub nurses, 12.9% for first assistants, and 1.4% for second assistants. For the whole surgical team, the glove perforation rate was 13.2% on the left hand, 8.2% on the right hand, and 10.7% on both hands. The puncture rate of the gloves used by the whole team was 13.2% on the left hand, 8.2% on the right hand and 10.7% on the right hand plus left hand gloves. The surgical team did not notice 78.3% of the holes in the gloves used during surgery. No glove perforation was detected in 45.7% of the operations, and the control group gloves did not have any holes (Table 2).
Distribution of Glove Perforation
In all operations.
Calculated without considering the number of puncture holes.
Calculated based on 70 gloves.
Calculated based on 140 gloves.
Calculated based on 280 gloves.
Calculated based on 560 gloves.
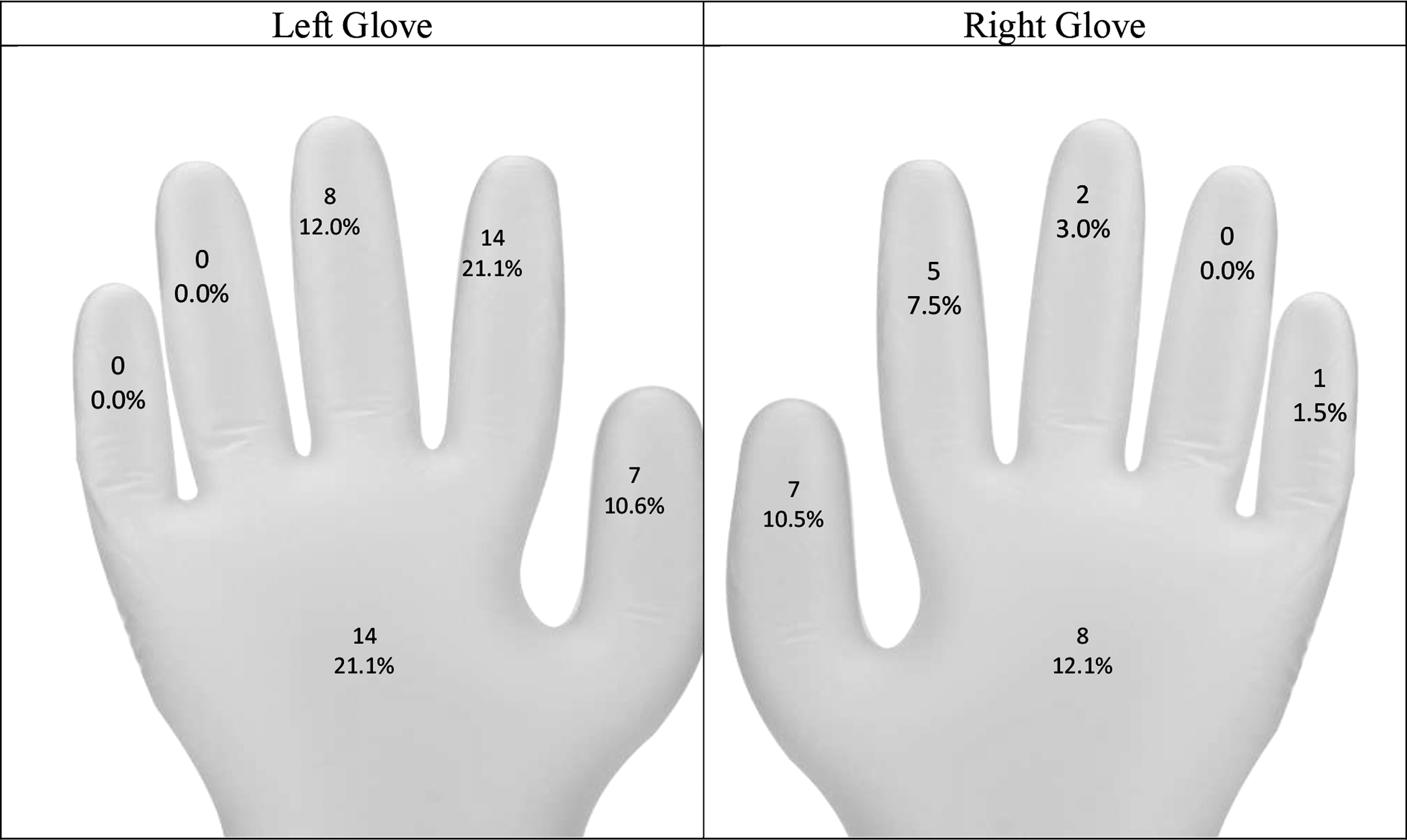
A total of 66 holes were found in 560 gloves used in surgical operations. The majority of these holes were on the non-dominant hand (left), observed on the thumb (10.6%), index finger (21.1%), middle finger (12%), and palm/dorsum of the hand (21.1%) (Fig. 1).
Number of holes in the gloves examined.
Table 3 shows the results of multivariable regression analysis of the variables affecting perforation in the right or left gloves used in surgery. According to this, surgeons had a 5.8 times greater risk of glove perforation (95% CI: 2.31–14.56), and the operation time being 61 minutes or longer increased this risk by 12.77 times (95% CI: 4.24–38.45) in the right or left gloves (Table 3).
Results of the Multivariable Logistic Regression Analysis Explaining the Factors Affecting Glove Perforation
p < 0.05. Significant p values (< 0.05) are shown in bold.
OR = odds ratio; 95% confidence interval (CI).
Discussion
In this study, the rate of surgical operations with at least one glove hole was 54.3%. Laine et al. [14] investigated the frequency of glove perforation in surgical procedures, comparing single and double gloves, and identified glove puncture in 18.3% of all operations. Shek and Chau [12] reported glove perforation in 8% of the surgical operations they investigated. In another study examining glove perforation in open and closed thoracic surgery, the authors identified glove holes in 70% of the former and 25% of the latter [15]. The results from the literature and our findings clearly show that the rate of perforation is higher in open abdominal and thoracic surgery.
In the current study, the greatest number of glove perforation was identified in an inguinal hernia repair (18.4%) and least seen in gastroenterostomy (7.9%). All of the operations were elective in this study. In a study investigating glove perforation in elective orthopedic surgery, Maffuli et al. [16] reported the rate of perforation to be 73% in joint replacement surgery, 17% in bone surgery, and 10% in soft tissue surgery. In the study by Çalışkan et al. [13], the puncture rate in the gloves used in pelvic surgery (27.09%) was found to be higher than those in non-pelvic surgery (17.06%). Soldá et al. [17] reported that glove perforation was most frequently seen in trauma surgery at a rate of 33%. In another study in which abdominal surgery was examined, it was determined that the rate of perforation in gloves was 9.6% and 3.3% in open closed procedures, respectively [14]. Similarly, in the present research, glove punctures mostly occurred in surgical operations involving dissection, e.g., hernia repair.
We identified a hole in 10.7% of all gloves. In the literature, glove perforation was reported as 3.58% in total knee replacement surgery [18], 8% in oral surgery [19] and open and laparoscopic cholecystectomy [20], 9.2% in thyroid surgery [21], and 24% in elective surgery [22]. The relatively higher rate of perforation found in the current study can be explained by the differences in the surgical procedures examined. Abdominal surgery often involves procedures such as abdominal wall closure, anastomosis, dissection, and tissue binding, which increase the possibility of glove puncture. To minimize injury, it is recommended that blunt suture needles are used for fascia and muscle closure [7].
According to the results, the rate of glove perforation used in surgery was the highest for surgeons (25%), followed by first assistants (9.30%), scrub nurses (6.45%), and second assistants (2.15%). The literature also reveals higher rates of glove puncture in surgeons compared to other team members [16,17,23,24]. Similar to the current study, some researchers found that glove punctures were most commonly observed in the gloves worn by surgeons and first assistants [11,13,25]. However, in other studies, it was stated that nurses were the second most frequent team member experiencing glove punctures after surgeons [22,26]. In contrast to these results, Kumar et al. [27] reported the highest rate of glove perforation in the first assistants in knee and hip surgery, whereas Lancaster et al. [28] detected glove punctures mostly in nurses in obstetric and gynecologic surgery compared with the other surgical team members. Despite varying according to the type of operation, glove perforation is generally considered to occur in surgeons at a higher rate because of their greater use of sharp instruments during operation. According to the Association of periOperative Registered Nurses (AORN) guidelines, to prevent sharps injury during surgery, surgeons should use suture packets, not their hands, when placing stitches into the needle holder, and they should utilize blunt instruments, such as forceps for the replacement, guidance, and removal of suture needles [7].
In the current study, a total of 66 holes were found in the gloves used in surgery, with most being located on the index finger (28.8%). In addition, 21.1% of the holes were on the index finger and 10.6% were on the thumb of the non-dominant (left) hand. Similarly, Walczak et al. [20] examined the gloves used in open and closed cholecystectomy and determined that the most frequent localization of perforation was the index finger of the non-dominant hand. Kumar et al. [27] found that 63% of the holes in the gloves were on the index finger and 20% were on the thumb of the non-dominant hand. In another study, it was reported that the most frequently punctured area of the glove was the index finger of the left hand [14]. Surgical team members often hold surgical tools (needle holders, clamps, scissors, etc.) that require finer motor coordination in their dominant hands, whereas they generally use their non-dominant hands to handle tissues and surgical needles. In addition, it is considered that perforation mostly occurs in the left glove because the left hand is used to support the tissue during tissue dissection.
We did not detect any holes in the control group gloves similar to the majority of studies in the literature [13,25,29]. However, in their randomized controlled study examining glove perforation in surgery, Makama et al. [30] reported that 0.8% of the gloves in the control group had holes [30]. They were not truly perforated but defective out of the package. The absence of perforation in the control group gloves indicate that surgical gloves are checked accurately and thoroughly during the manufacturing stage. This also confirms that the gloves were punctured during surgery.
Surgical team members removed the glove when they noticed glove puncture during surgery. However, because most of the perforations (78.3%) were not noticed, these gloves were used until the end of the operation. As shown in Table 3, there was no difference in terms of perforations in the gloves used in the operations at the end of the day or at the beginning of the day. Other researchers reported unnoticed glove perforation at a rate of 66.9% in knee and hip replacement surgery [8], 72.7% in minor and major orthopedic surgery [23], and more than 85% in laparoscopic and open cholecystectomy [19,21]. Beldame et al. [18] found that none of the glove holes were detected during total hip replacement operations. The findings of the current study are consistent with the literature. Surgical team members and patients may be at risk of infectious diseases due to unnoticed glove puncture. It is recommended by AORN that surgical team members use indicator gloves (under-gloves and over-gloves of different colors) for easier detection of glove perforation during surgery and allowing practitioners to immediately change their gloves and restore an intact barrier [7].
The rate of glove perforation was higher for surgical procedures longer than 60 minutes. Similarly, in the literature, more glove punctures were identified in hand surgery and abdominal surgery that lasted longer than 60 minutes [13,16]. Cole and Gault reported [31] that glove punctures increased during plastic surgery operations that lasted two hours [31]. Otis and Cottone [32] suggested that latex gloves should be replaced at intervals of less than 120 minutes. In a review of 19 studies published from 2003 to 2016, the maximum time before changing gloves was indicated as 120 minutes for gastrointestinal, thoracic, and gynecologic surgery; 90 minutes for oral and maxillofacial surgery; and 60 minutes for ophthalmic surgery [33]. Because a high percentage of glove holes go unnoticed, we consider that team members should change gloves at certain intervals during surgery. As the operation time increases, the duration of exposure to surgical instruments also increases. The increase in the length of operation causes a higher risk of perforation to the gloves worn by surgical team members. This study was in agreement with the literature in terms of revealing a linear relation between operation time and glove perforation rate.
It was determined that the number of perforated gloves increased as the surgical experience period increased. As team members' surgical experiences increase, they work faster, move faster, and intervene more in the surgical field. Because of increases the exposure to surgical materials, the rate of perforated gloves also increased.
In this study, being a surgeon and performing an operation for longer than 60 minutes were found to be factors affecting glove perforation. During surgical operations, surgeons perform suture removal procedures and use surgical tools, such as scissors, clamps, and advanced technological materials, which is considered to result in more punctures of surgeons' gloves. As the length of the operation increases, surgeons' use of and exposure to sharp instruments also increases. We believe that this increased exposure is one of the reasons for the greater rate of glove puncture experienced by surgeons. Similarly, other researchers reported that the glove perforation rate was higher in surgeons and long operations [13,16,21,34]. It was found that workflow did not affect the perforation rate. There was no difference in glove perforation at the beginning or end of the day. According to research, glove perforation was not affected by using the scrubbing nurse glove, type of surgery, operation time interval (day, night, etc.), use of advanced technological material, and size of glove. Glove performation was impacted by surgeon's glove and the duration of surgery. Also, fatigue has not been examined.
Study limitations
In this study, only gloves used in open abdominal surgery performed in the general surgery operating room in one hospital were examined. Therefore, the results of the research can only be generalized to the gloves carrying the characteristics of this sample group.
In the questionnaire used for data collection, the question about changing gloves during surgery was answered by each surgical team member who wore gloves during surgery, and therefore the reliability of the data depends on the accuracy of the participants' responses.
Another limitation of the study is the exclusion of gloves worn by surgical team members after being changed for any reason. We also did not examine the gloves of surgical team members who replaced other team members during an operation.
Finally, the EN455-1 method was performed by the same researcher for glove collection and detection of perforation. The absence of a second observer may be considered as a limitation.
Conclusion
This study was performed to determine the perforation rates of gloves used in open abdominal surgery. The results revealed that glove perforation occurred in 54.3% of surgical operations, most worn by surgeons (25%), and the holes were generally not noticed by surgical team members (78.3%). The punctures in the gloves were most frequently seen in the non-dominant hand and on the index finger. As the operation time increased, the rate of glove perforation also increased.
According to the results of the study, we recommend that gloves should be changed at intervals of less than 60 minutes in open abdominal procedures performed in general surgery; all surgical team members but especially surgeons should change gloves at certain intervals; in operations involving dissection, especially the glove on the non-dominant hand should be changed more frequently; the use of indicator gloves should be commonly adopted and surgical team members should be provided with necessary training about the use of these gloves; and when handling sharps instruments, the hands-free technique and safe tools (e.g., blunt suture needles and sheathed scalpels) should be used.
Footnotes
Acknowledgments
This study was accepted for the 2017 Master's Program of Manisa Celal Bayar University, Institute of Health Science.
Author Disclosure Statement
There is no conflict among authors.