
Abstract
Abstract
Background:
Renovating or building a new intensive care unit (ICU) can be a challenging project. Planning the renovation or rebuild as a quality improvement project will help break down the process into manageable pieces with clear goals.
Methods:
Literature was reviewed with regards to ICU design and renovation, with specific attention to patient quality improvement, process and structural change, healthcare systems engineering, emerging technology, and infection control.
Results:
In any quality improvement initiative, a first step is to create a multidisciplinary change team charged with leading the rebuild process. This team should include frontline providers, administration, architects, infection prevention specialists, and healthcare system engineers. Healthcare system engineers (HSEs) are specialized system and human factors engineers who can assist with data analysis, create mathematical models to anticipate areas of difficulty, and perform simulations to assist with the actual structural changes as well as the process changes aimed at eliminating nosocomial infections. Every aspect of creating a new ICU space should begin with infection control standards of practice ranging from selection of furniture and computer keyboards, to identifying the best location of the soiled utility rooms. There are many infection control products that may be considered during the building process such as tele-tracking hand hygiene stations and heavy-metal–coated surfaces aimed at decreasing surface colonization and subsequent infections.
Conclusions:
This article offers suggestions on renovating or rebuilding an ICU aimed at eliminating the preventable harm associated with hospital acquired infections.
C
Methods
The published literature was reviewed with regards to ICU design and renovation, with specific attention to patient quality improvement, process and structural change, healthcare systems engineering, emerging technology, and infection control.
Results
Avedis Donabedian, a forefather of healthcare quality improvement, created a model more than 50 years ago to evaluate the quality of healthcare that focused on the triad of structure, process, and outcomes [1]. Structure includes all factors that affect how care is delivered including the physical facility, equipment, and human resources. Process is defined as all the individual actions that are performed to deliver care. Outcomes are the results of the care rendered to the patient. Most quality improvement initiatives focus on modifying processes to affect outcomes because structure is often fixed and difficult to change. Building or renovating a new ICU creates the perfect environment to change the structure and process of care to yield optimal improvements.
Involvement of healthcare systems engineers can assist with the new ICU build or renovation. Healthcare systems engineers (HSEs) are industrial and human factor engineers with additional healthcare training. This additional training includes healthcare financing, patient flow dynamics, medical informatics, logistics, supply chain structure and function, healthcare improvement science, and infection control [2]. They are specialists in data management and analytics. They can perform intelligent data analysis, create mathematical models (e.g., logistic regression, decisions trees, and neural networks), and complete simulations to assess how structure affects work and patient flow, and how these in turn affect hospital-acquired infections. These professionals, with the assistance of content experts such as critical care nurses, physicians, and infection control specialists, can help evaluate and influence current processes for the new ICU as well as help solve questions such as where the best place is to locate dirty utility rooms based on employee and patient flow. Healthcare systems engineers understand that “form follows function” and are critical team members for quality improvement [3].
The first step to any ICU redesign or renovation, similar to any quality improvement project, is to form a multidisciplinary change team. This change team should include clinical members and nonclinical members. The clinical members should be diverse and include frontline staff employees. Deference to expertise, one of the five pillars of high-reliability organizations, is vital for redesigning units and workflows [4]. This includes soliciting input from the frontline caregivers about opportunities for improvement in their current workflows and how structure changes may improve existing workarounds. The frontline staff often know the answers for improvement and can provide useful insight when asked. An infection control specialist must be part of the clinical team because every design aspect should have infection control rooted in the foundation of the new plan. The nonclinical team members should include the architects, administration, and HSEs. In large projects such as an ICU redesign there will be competing interests among the team members. The team must utilize good negotiation skills to effectively balance the varying team member goals. Work must focus on collaboration in which all parties work together to find a mutually agreeable solution to maintain the ongoing relationship rather than settling for a compromise in which both parties lose something important [5]. Once the change team and its leader are identified, the group can embark on the evidence-based ICU design undertaking.
In 2012, the American College of Critical Care Medicine published a guideline for designing intensive care units. This guideline serves as an excellent process manual for the change team [3]. The guideline breaks down the ICU into four critical zones: the patient care zone, clinical support zone, unit support zone, and the family support zone (Fig. 1). Each of these zones has its own requirements and daily workflow that must be reviewed and optimized. They also each have their own infection control issues, therefore, an infection control risk assessment must be performed in each zone. Infection control must be kept at the forefront during the entire design process. Designing for ICU infection control can lower nosocomial infections and decrease overall patient morbidity, mortality, and resource utilization [6].
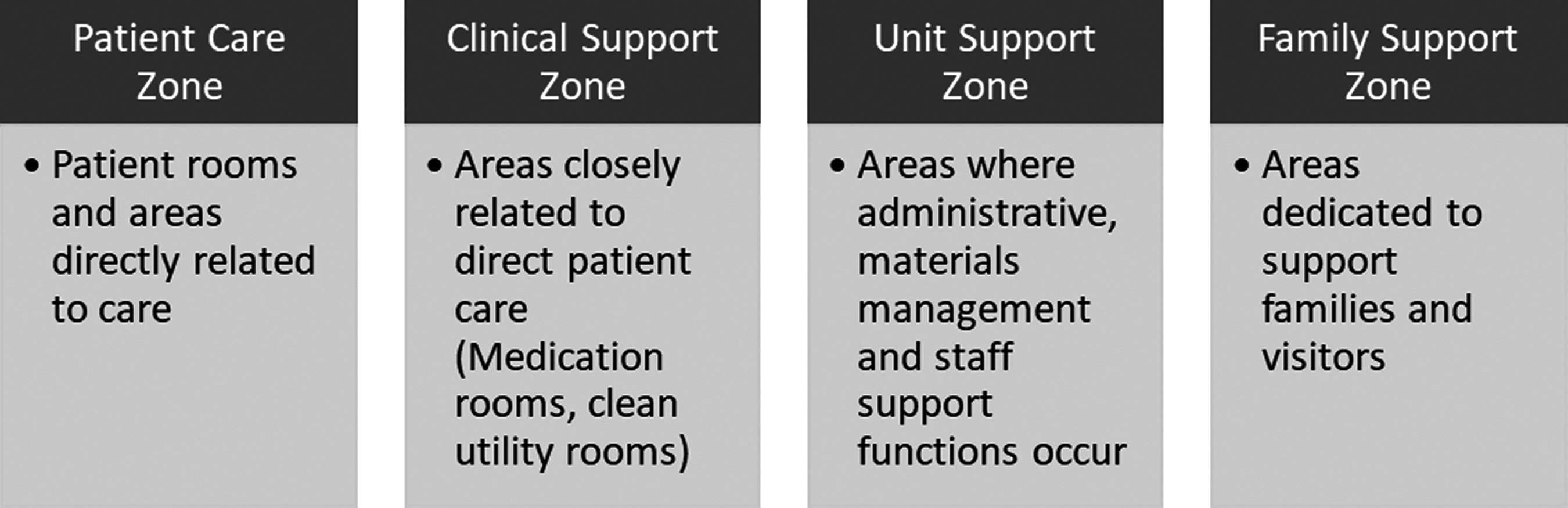
Four intensive care unit zones should be evaluated separately when building or renovating a new intensive care unit (ICU).
Intensive care infection control is everywhere. Infection control strategies are influenced by the type of floors, the head and boon wall configuration, type of furniture, window treatments, and computer keyboards. Thoughtful placement of trash cans, sharps disposal and biohazards, as well as hand washing sinks are essential to decreasing nosocomial infections. Even the building process has inherent infection control risks. In 2003, the U.S. Centers for Disease Control (CDC) in conjunction with the Healthcare Infection Control Practices Advisory Committee (HICPAC), published guidelines regarding environmental infection control in healthcare facilities [7]. They recommend that infection control specialists be involved in all facets of any hospital construction, remodeling, and demolition. There should be mandatory adherence agreements for infection control built into any construction or demolition contract. Infection specialists must utilize active surveillance to monitor for airborne infections in immunocompromised patients during any construction as well as implement dust-control measures. Fungal spores are often released within dust created during construction projects and must be controlled and contained to prevent outbreaks in other areas of the hospital away from the construction site itself.
In general, it is recommended that ICU rooms should be single occupancy to improve patient safety, decrease infections, decrease antibiotic use and increase sleep quality [8–10]. Because of infection risks, carpet should be avoided. There should be plenty of windows for natural light, but window treatments must be selected to allow easy cleaning according to infection control practices. Patient room furnishings must also be selected with ease of cleaning forefront in the selection process.
There are several special infection risks that must be considered during ICU design. Although many ICU patients do not often use them, toilet facilities can be a vector for infection. Shared patient toilets should be avoided. Swing-out or fold-down commodes are not recommended because of cleaning difficulty. Additionally, these specialty toilets may not be suited for bariatric patients [3]. A bedpan washing device and a fluid removal system should be available in each patient room as part of the toilet or as a standalone device. This will avoid transporting waste outside of each patient room. Sharps containers must be located within each patient room and be in a visible location. Utilization of dialysis equipment within patient rooms requires appropriate water and drain facilities. These water and drain facilities must be separate from handwashing sinks and should follow all local code requirements [3,7].
Hand hygiene practices are critical to combat nosocomial infections and must become a cultural practice within the unit and institution. Recommendations are for both soap and water as well as gel systems be available within the patient care zone. The gel dispenser systems should also be placed within the clinical support, unit support, and family support zone. Consistent and reliable processes must be created to ensure soap and gel systems remain full, paper towels are replaced, and garbage cans are emptied on a scheduled and as-needed basis. Overflowing ICU garbage cans with used personal protective equipment, paper towels, and other items may increase nosocomial infections.
Location of sinks, paper towel dispensers, and gel systems are important for hand hygiene compliance. Healthcare systems engineers can help find proper locations for these items based on workflow analysis. They must be located conveniently near the entrance and exit of the room. Data demonstrates that there may be as many as 279 hand hygiene opportunities per patient day in hospital wards [11]. Compliance with hand-washing regulations is dependent on sensible placement of gel systems and handwashing sinks. Ensuring compliance with these hand-washing opportunities can be challenging and should be integrated into the design process of an ICU. The gold standard for compliance measurement has rested on direct observation, which is time consuming and can induce the Hawthorne effect. There are many new compliance systems on the market including videotaping and tele-tracking. Tele-tracking systems can place a tag within the hand hygiene stations and another on the identification badge of the hospital workers. Every time the employee enters or exits the patient room is recorded (denominator) as well as if the hand hygiene dispenser was utilized (numerator). This allows electronic calculation of hand hygiene rates at a provider, room, and unit level. These systems have been shown to increase hand hygiene compliance, but ongoing analysis needs to be completed to show if they impact nosocomial infection rates [12].
Another infection prevention strategy that may be considered in an ICU renovation or rebuild is utilizing heavy metal (copper or silver) coated surfaces on high touch areas. Copper has the most published data supporting its use and is the only heavy metal evaluated in clinical trials [13]. An intention-to-treat randomized control trial between July 12, 2010 and June 14, 2011 in the ICUs of three hospitals was completed by Salgado et al. [14]. Patients were randomly assigned to copper-coated surface ICU rooms or standard ICU rooms. Hospital-acquired infections and room colonization with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE) was compared between room types. Patient hospital-acquired infection rates, as well as room colonization of MRSA and VRE were statistically decreased in the copper-coated rooms [14]. Copper-coated items included the high-touch areas such as bedrails, intravenous poles, overbed tables, arms chairs, nurses call button, computer mouse, bezel of the telemetry monitors, and the palm rest of in-room computers. Although this copper-coated strategy has some scientific merit, its implementation may come down to a cost-benefit analysis within the renovation or rebuild budget. Healthcare systems engineers can perform this type of evaluation factoring in the cost of hospital-acquired infections within the institution compared with copper-coating costs.
Other technologies that may be of interest to the change team are ultraviolet lights and peroxide cleaning systems. These systems can decontaminate hospital surfaces and are residual free. Disadvantages, however, are that they are only useful for terminal cleaning after a thorough decontamination with approved cleaners. These products do have installable systems that can be utilized in empty, clean rooms. They must be considered early in the project to ensure appropriate wiring is created. Again, HSEs can help locate the optimal in-room location of these devices to get the best capture of the infection control technology.
Conclusions
Renovating or rebuilding an ICU is an enormous undertaking that should be structured similar to any other quality improvement initiative to optimize its success. A multidisciplinary change team should be created with both clinical and non-clinical staff. Frontline staff should be key members on this change team. Healthcare systems engineers are also vital team members and can perform many mathematical analyses, create models, and execute simulations to help with decision making. They can be utilized throughout the rebuild/renovation. Form follows function, and all processes within the four care zones should be evaluated, modified, and improved within the new space. A rebuild project serves as a perfect opportunity to make changes to those processes that are frustrating, inefficient, or require workarounds for their routine use. Infection control is weaved throughout the project and an infection control specialist is a vital team member. Consider utilizing new technology such as hand hygiene compliance systems, heavy-metal–coated surfaces, and permanently mounted ultraviolet lights. Following the evidence-based guidelines provided by Thompson et al. [2] will keep the project focused, thorough, and improve patient care by eliminating surgical and nosocomial infections. An open-minded, purpose-driven change team that incorporates the tenets of quality improvement with an interwoven focus on infection control is inherent to the project success and improved patient outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.