
Abstract
Abstract
Background:
The objective of the study was to investigate the effects of intra-abdominal infection after curative gastrectomy on the prognosis of patients.
Patients and Methods:
Data were collected for enrolled patients who underwent curative gastrectomy in two centers; the relationship between intra-abdominal infection and prognosis was analyzed.
Results:
Of the 5,721 patients in the entire group, intra-abdominal infection occurred in 202 (3.5%) patients. Co-morbidities and duration of surgical procedures ≥240 minutes represented the independent risk factors for intra-abdominal infection. The overall five-year survival of patients with and without intra-abdominal infection was 60.2% and 64.3%, respectively (p = 0.041). After propensity score matching, the five-year overall survival between the two groups was not significantly different (p = 0.909). T staging, N staging, American Society of Anesthesiologists score, and age were independent prognostic factors for the overall survival of patients who underwent curative gastrectomy. The meta-analysis of the random effects model showed that there were no significant differences in the five-year overall survival between patients with and without intra-abdominal infection.
Conclusions:
The development of intra-abdominal infection after curative gastrectomy is associated closely with co-morbidities and longer operation time, whereas intra-abdominal infection does not lead to reduced long-term survival of patients.
Intra-abdominal infection represents one of the serious complications after gastrectomy, and its incidence in gastric cancer after operation, according to the literature, is 3.4%-14.3% [1–4]. Such conditions as pseudoaneurysms, sepsis, and septic shock caused by intra-abdominal infection not only increase patients' suffering, prolong their hospital stays, and increase their costs of hospitalization but also reduce their quality of life, leading even to death [5,6]. In recent years, scholars have attached great importance to surgical safety and management of post-operative complications, and studies are yielding increasingly deep insights into the factors associated with intra-abdominal infection diagnosis and treatment, etc., with some progress made so far.
Recent studies have shown that post-operative intra-abdominal infection may lead to reduced long-term survival of cancer patients [1–4]. Tokunaga et al. [1] reported that intra-abdominal infection was an independent risk factor for long-term survival after curative gastrectomy, and the study by Hayashi et al. [4] showed that post-operative infectious complications contributed to an increased risk of recurrence of gastric cancer.
Most of these studies, however, were based on single-center case data, and the sample size in the subgroup stratified analysis of tumor staging was small, which might lead to a biased result. Therefore, we aimed to explore the effects of intra-abdominal infection after operation on long-term survival through the analysis of clinical and pathologic data from patients who underwent curative gastrectomy, based on a large multi-center sample.
Patients and Methods
The clinical pathologic data of patients with a diagnosis of primary gastric cancer who underwent curative gastrectomy from January 1996 to December 2014 in Fujian Medical University Union Hospital (FMUUH) and patients who underwent curative gastrectomy in the International study group on Minimally Invasive surgery for GASTRIc Cancer (IMIGASTRIC) study (NCT02325453) [7] between January 2000 and December, 2014 were collected prospectively and analyzed retrospectively; tumor staging was performed in accordance with tumor, node, metastases (TNM) staging, based on the Union for International Cancer Control staging standards (7th edition, 2010) [8].
Patients were included if (1) they were pathologically confirmed to have primary gastric adenocarcinoma before operation; (2) examinations such as chest radiography, abdominal ultrasound, and abdominal computed tomography showed no direct invasion of the adjacent organs, such as the pancreas, spleen and liver; no distal metastasis to the liver, lungs, and abdomen; and no significantly enlarged lymph nodes around the abdominal aorta; and (3) patients had undergone D1+ or D2 lymph node dissection, and there was a pathologic diagnosis of R0 resection.
Patients were excluded if (1) tumor seeding in the abdominal cavity or distal metastasis was seen during operation; (2) patients had undergone palliative surgery; (3) patients' pathologic diagnostic data and follow-up data were incomplete; or (4) patients were treated with neoadjuvant chemotherapy or neoadjuvant radiotherapy.
Variables and definitions
Intra-abdominal infection, also known as organ/space surgical site infection (SSI) was defined according to the surgical patient component of the 1999 Centers for Disease Control and Prevention National Nosocomial Infection Surveillance System manual [9]. The definition refers to any one of the following signs of infection within any organ/space except the abdominal wall within 30 days after operation: Purulent drainage, positive culture of micro-organisms, re-operation, and support of histopathology or imaging evidence. Anastomotic leakage, pancreatic leakage, duodenal stump leakage, jejunal leakage, and abdominal abscess of unknown origins are included in the definition of intra-abdominal infection.
We also collected data regarding potential related factors of intra-abdominal infection, including sex, age, American Society of Anesthesiologists (ASA) score [10], body mass index (BMI), tumor site, TNM stage [8], operation type, duration of surgical procedure, blood loss, number of dissected lymph nodes, etc.
Follow-up
The follow-up–related data of the FMUUH patients were collected by two well-trained research assistants when patients were discharged; data were updated after each follow-up and reviewed by an attending physician before data analysis. The follow-up, with an interval of three to six months, lasted until the patients died or June 2017 (median, 44 months). The final follow-up for IMIGASTRIC was conducted in November 2016, and the median duration was 38 months; the overall survival was defined as the interval from the diagnosis of gastric cancer to death from any cause.
Statistical processing
The Mann-Whitney U test was performed on the continuous variables, and the chi-square test or the Fisher exact test was performed on the categoric variables. Survival was calculated using the Kaplan-Meier method, and the survival curve was plotted also using the Kaplan-Meier method; survivals were compared using the log-rank test. In this study, a ratio of 1:2 was adopted to reduce bias as follows: Center, age, sex, ASA, T staging, N staging, and post-operative chemotherapy were used as the variables, and the propensity score of each case was calculated using the logistic regression model. Subsequently, the cases of with and without intra-abdominal infection with similar scores were paired in a ratio of 1:2 according to the principle of proximity [11]. A p value <0.05 indicated statistical significance. The data were subjected to statistical processing using the SPSS version 18.0 (SPSS, Chicago, IL). The potential publication bias was analyzed using the Egger test, and data were analyzed by means of Stata 13.0 (STATA Corporation, College Station, TX).
Results
Incidence of intra-abdominal infection
The cohort data of two centers were included in this study, and 5,721 patients who underwent curative gastrectomy were enrolled eventually (FUHH, 5,228; IMIGASTRIC, 493). The general clinical pathologic data of patients with intra-abdominal infection are shown in Tables 1 and 2. Among the entire group of patients, intra-abdominal infection occurred in 202 (3.5%) patients, and 12 (5.9%) patients died of failed treatment of intra-abdominal infection. Age, co-morbidities, ASA score, tumor size, T staging, duration of operation, intra-operative blood loss, and post-operative adjuvant chemotherapy between patients with and without intra-abdominal infection were significantly different.
Characteristics of Patients with or without Intra-Abdominal Infection after Curative Gastrectomy
FMUUH = Fujian Medical University Union Hospital; IMIGASTRIC = International study group on Minimally Invasive surgery for GASTRIc Cancer; SD = standard deviation; ASA = American Society of Anesthesiologists; LN = lymph node.
Details of Intra-Abdominal Infection
Intra-abdominal infection-related factors
The potential risk factors for abdominal infection in the entire group were subjected to uni-variable and multi-variable analyses. A total of seven factors were associated closely with the occurrence of intra-abdominal infection, including co-morbidity (p < 0.001), ASA score (p < 0.001), pT4a (p = 0.044), pT4b (p = 0.001), pN3 (p = 0.021), duration of operation (p < 0.001) and intra-operative blood loss (p = 0.005); further multi-variable analysis showed that co-morbidities (odds ratio [OR] = 1.884, p < 0.001) and duration of operation ≥240 minutes were independent risk factors for intra-abdominal infection (Table 3).
Uni-Variable and Multi-Variable Analyses for Intra-Abdominal Infection in Patients after Curative Resection of Gastric Cancer
FMUUH = Fujian Medical University Union Hospital; IMIGASTRIC = International study group on Minimally Invasive surgery for GASTRIc Cancer; SD = standard deviation; ASA = American Society of Anesthesiologists; LN = lymph node.
Survival of patients with gastric cancer
In the entire group of patients, the five-year overall survival was 60.2% in the group of patients with intra-abdominal infection, which was significantly different from that in the group of patients without intra-abdominal infection (64.3%, p = 0.041, Fig. 1). The differences in such factors as demographic and clinical characteristic, pathologic data, and therapeutic factors between the two groups of patients might lead to biases. We performed a 1:2 matching analysis between the with and without intra-abdominal infection groups using estimated propensity scores for each patient. After propensity score matching, there were 202 patients in the intra-abdominal infection group and 404 in the without intra-abdominal infection group. The five-year overall survival between the two groups was 60.2% and 58.1% (p = 0.909), respectively, indicating no statistically significant differences (Fig. 1).
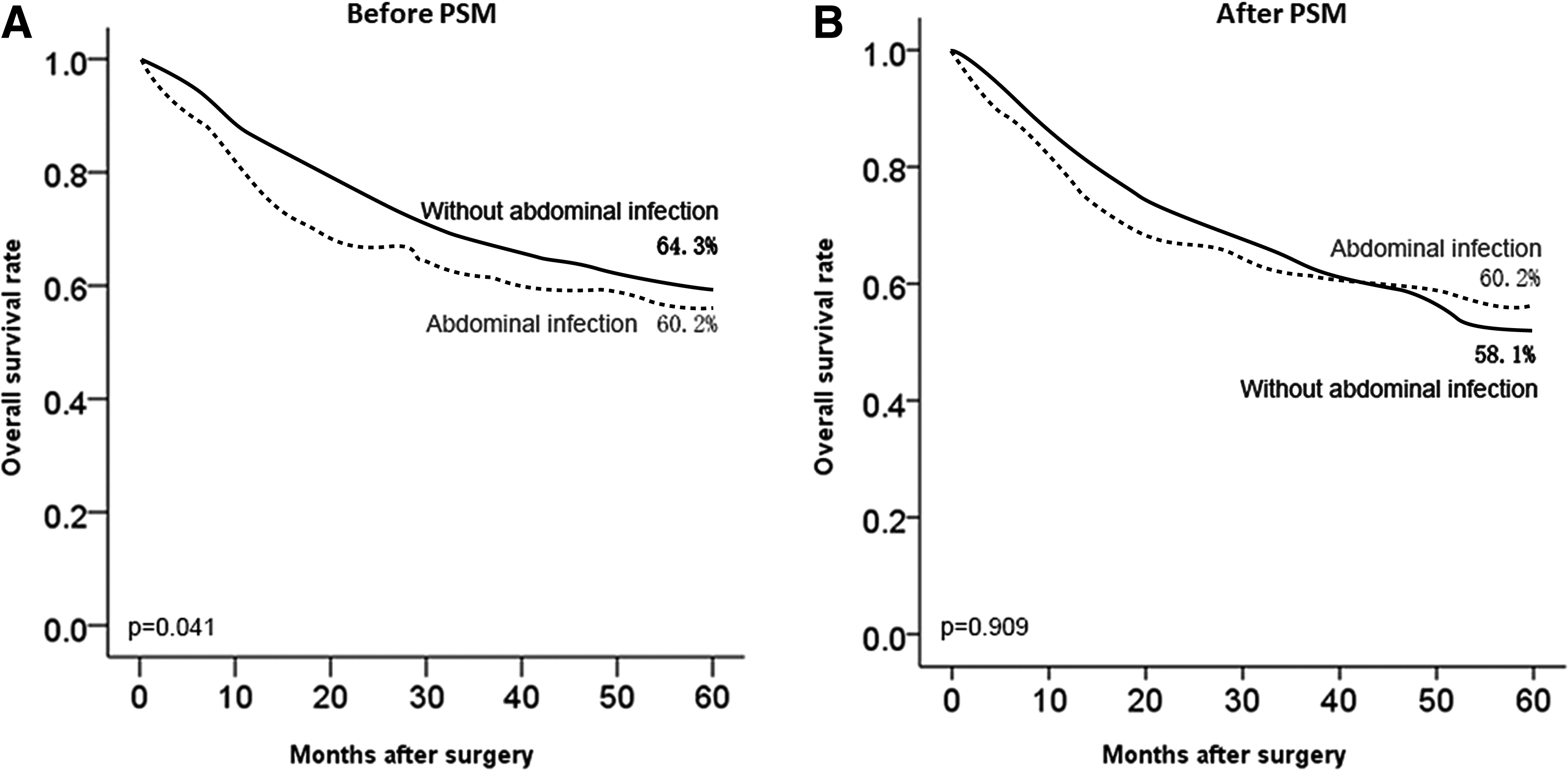
Overall survival curves after curative gastrectomy before and after propensity score matching (PSM) in patients with and without post-operative intra-abdominal infection. (
Prognostic factors in the entire group of patients
Supplementary Table S1 presents the analysis of the risk factors for the overall survival of patients after curative gastrectomy before propensity score matching. The results showed that T staging, N staging, age, and ASA score represent the independent risk factors for the overall survival of patients after curative gastrectomy; that post-operative chemotherapy is a protective factor for patients; and that intra-abdominal infection did not function as an independent risk factor for the overall survival of patients with gastric cancer (p > 0.05). Table 4 presents the analysis of the risk factors for the overall survival of patients after propensity score matching, and the results also showed that intra-abdominal infection is not an independent risk factor for the overall survival of patients who underwent curative gastrectomy (p > 0.05).
Uni-Variable and Multi-Variable Analyses for Overall Survival in Patients after Curative Resection of Gastric Cancer (after Propensity Score Matching)
FMUUH = Fujian Medical University Union Hospital; IMIGASTRIC = International study group on Minimally Invasive surgery for GASTRIc Cancer; SD = standard deviation; ASA = American Society of Anesthesiologists; LN = lymph node.
Comparison of relative literature on intra-abdominal infection
We searched the Medline, Cochrane, OVID, Embase, and Web of Science databases for relevant studies through April 2018. All the studies were single-center and retrospective, with the number of study cases being 265-1,951 (Supplementary Table S2) [1–4]. The incidence of intra-abdominal infection in our study was similar to that in the studies found (3.5% vs. 3.4%-14.3%). The meta-analysis of the random effects model showed that the five-year overall survival of patients with and without intra-abdominal infection was close (OR = 0.69, 95% confidence interval [CI] [0.48, 1.00], p = 0.050) (Supplementary Fig. S1). The subgroup analysis of patients with stage II/III gastric cancer revealed that the five-year overall survival of patients with and without intra-abdominal infection was not significantly different (OR = 0.75, 95% CI [0.46, 1.22], p = 0.25) (Supplementary Fig. S2).
Discussion
Intra-abdominal infection not only threatens the life safety of patients after operation, prolongs hospital stays, and increases hospitalization costs, but its treatment also consumes much of the energy of the surgical team, making it one of the most common and serious complications after gastric cancer surgical procedures [12–15]. The incidence of intra-abdominal infections after gastric cancer surgery is 3.4%-14.3%, as reported in the literature. This study showed that among the 5,721 patients in the entire group, the incidence of intra-abdominal infection was 3.5% (n = 202), which was similar to reports in the literature.
The risk factors for intra-abdominal infection in patients who undergo curative gastrectomy as reported in previous literature included age, high BMI, diabetes mellitus, peri-operative blood transfusion, long duration of operation, large amount of blood loss during operation, total gastrectomy, and combined organ resection [16–19]. In this study, we found that long duration of operation was associated closely with intra-abdominal infection after operation and that it was an independent risk factor for the incidence of intra-abdominal infection after operation.
Prolonged duration of operation led to increased exposure time to bacteria and tissue trauma and decreased concentration of antibiotic agents in the tissues, thereby increasing the susceptibility to infection [20]. In addition, prolonged duration of operation is associated closely with the poor technical skills of inexperienced surgeons or accidents during surgical procedures (such as accidental organ damage and involvement of surrounding organs or tumors). Therefore, duration of operation should be shortened as much as possible on the basis of ensuring curative gastrectomy, which may reduce the occurrence of intra-abdominal infection.
There are few relevant studies and no conclusions currently as to whether intra-abdominal infection affects the prognosis of patients with gastric cancer [1–4]. Some scholars argue that the complex recovery process after operation may inhibit the responses of the immune system to the proliferation of tumor cells, leading to reduced tumor-specific survival and that the systemic inflammatory responses may exacerbate immunosuppression in patients with intra-abdominal infections, thereby affecting their prognosis [21,22]. In other study, researchers believe that intra-abdominal infection leads to the cultivation of tumor cells in the abdominal cavity of the patient, which will increase the risk of local recurrence.4
Some deficiencies exist in these studies [1–4], however: first, most of them are single-center retrospective studies based on small sample sizes; therefore, they unavoidably have selection biases. Second, some articles in the literature have not defined intra-abdominal infection clearly and even enrolled patients subjected to empirical use of antibiotics agents in studies on intra-abdominal infection; this results in a higher incidence of intra-abdominal infection, poor specificity of study subjects, and failure to win wide acceptance of the conclusions. Third, the differences between some research groups concerning infected and non-infected patients are very large concerning matters such as TNM staging; these confounding factors may contribute to poor prognosis of patients with intra-abdominal infection.
In this study, however, data were collected from a large sample size of international multiple centers, intra-abdominal infection was defined strictly, and the propensity score matching ratio was employed to balance the differences between the groups. With this, we found that there were no significant differences in prognosis among patients with and without intra-abdominal infection.
In addition, we performed a meta-analysis of the random effects model for intra-abdominal infection-related studies, and the results showed that there was no significant difference in the five-year overall survival between patients with and without intra-abdominal infection. Use of available data, however, for the exploration of the relationship between intra-abdominal infection and the prognosis of patients who undergo curative gastrectomy, especially using well-balanced data based on a large multi-center sample, is particularly important and can be used as the basis for prospective studies.
Conclusions
The development of intra-abdominal infection after curative gastrectomy is associated closely with co-morbidities and longer operation time, whereas intra-abdominal infection does not lead to reduced long-term survival of patients.
Footnotes
Acknowledgment
The study was sponsored by the scientific and technological innovation joint capital projects of Fujian Province (2016Y9031);Construction Project of Fujian Province Minimally Invasive Medical Center (No. [2017]171);The second batch of special support funds for Fujian Province innovation and entrepreneurship talents (2016B013); CARIT Foundation (Fondazione Cassa di Risparmio di Terni e Nami), No.0024137.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.