
Abstract
Abstract
Background:
Surgical site infection is associated with a substantial healthcare burden and remains one of the most challenging complications to treat. Airborne particles carrying contaminating micro-organisms are responsible for the majority of these infections.
Methods:
Various operating theater ventilatory systems have been developed to prevent direct airborne bacterial inoculation of the surgical wound. Laminar air flow uses positive pressure air currents through filtration units to direct air streams away from the operative field in order to create an ultraclean zone around the operative site.
Discussion:
Early studies reported lower infection rates with laminar air flow and therefore it became the accepted standard for implant-related surgery. However, more recent evidence has questioned its clinical importance. The purpose of this article is to review contemporary laminar air flow handling systems and the current evidence behind their use.
The prevention of surgical site infection (SSI) is a fundamental aspect of surgical practice and is integral to all subspecialties. Post-operative infection is associated with substantial healthcare costs and carries a substantial health risk in terms of prolonged hospitalization and increased mortality [1]. In the United States, SSIs are the most common type of hospital-acquired infection and occur in up to 5% of patients undergoing elective inpatient surgery [2]. The estimated incidence ranges from 160,000 to 300,000 per year and the estimated annual cost ranges from $3.5 billion to $10 billion [2]. Surveillance programs in National Health Service hospitals in England estimate that SSIs account for 16% of all health-care–associated infections ranging from less than 1% in hip and knee joint replacement surgery to 9% in large bowel surgery [3].
The operating room environment plays a key role in SSI prevention and requires detailed consideration. Airborne particles carrying contaminating micro-organisms are responsible for 98% of SSIs and arise from multiple sources such as skin surfaces, surgical instruments, clothing, dust, and condensation droplets produced from talking, sneezing, and coughing [4]. Human skin is a rich milieu for commensal micro-organisms of which the most common culprit for SSI is Staphylococcus. An individual sheds 107 skin cells per day and many of these become airborne particles within the surgical environment [5]. Small particles (<5 μm) become suspended in the air while larger particles either settle on nearby surfaces or move between sites within air flow currents [6]. Bacteria adhere to larger particles and form aggregates known as colony-forming units (CFUs) that can inoculate wounds [7]. Ventilatory systems are designed to provide air quality control to reduce the harmful effects of airborne contamination. The aim of this article is to review contemporary laminar air flow handling systems and the current evidence behind their use.
Ventilatory Systems
Ventilatory systems use positive pressure air flow to transfer contaminated air streams away from the surgical field preventing direct bacterial inoculation of the wound. The systems draw in air from the roof-level through a series of fans and create a dynamic barrier around the operative site. Conventional plenum systems rely on an air pressure gradient between the operating theater and its outside corridors. Air is at higher pressure inside the operating theater and is fed through vents at floor-level, moving clean air from inside to outside. Theoretically, contaminated air from outside the theater should not be drawn in but this system is made inefficient by door openings and movement of personnel within the theater. The benchmark for efficacy in plenum systems with 20 air changes per minute is to achieve less than 35 CFU/m3 [8]. Laminar air flow (LAF) systems are used more commonly in implant-related surgery because they carry a higher risk of infection resulting from the production of antibiotic-resistant biofilm. Normally quiescent low-volume CFUs can flourish in these conditions causing tissue destruction unless the implant is removed [9].
Laminar air flow systems were originally designed by the National Aeronautics and Space Administration (NASA) to create an ultraclean environment for the assembly of missile parts [10]. They provide a unidirectional flow of air that moves at a uniform velocity and pressure (>15 Pa). In the operating theater, this occurs within a central enclosed space formed by vertical panels extending from the ceiling. Air is drawn through a series of filters including a high-efficiency particulate air (HEPA) filter that, by definition, should have the capability to filter out at least 99.97% of airborne particles measuring 0.3 μm diameter [11]. Each HEPA filter has a regulatory manometer that measures the resistance to filtration as a result of becoming blocked. Filters should be positioned as close to the air supply outlet as possible to ensure that particles are filtered out well before entering the operating theater. Air flow can be directed either horizontally through wall-mounted fans or, more commonly, vertically through ceiling-mounted systems (Fig. 1). Ultraclean air is produced by LAF systems and is defined as containing <10 CFU/m3 but in order to eliminate all risk of airborne contamination it should be <1 CFU/m3 [7]. In contrast to plenum systems, LAF more efficiently reduces contaminated air from peripheral areas entering the ultraclean area and also from around the wound as positive pressure air currents are targeted directly over the operative site. Also, air changes can occur more than 300 times per hour compared with standard plenum rates of 20 air changes per hour. However, the main problem with LAF is turbulence that is caused by physical barriers and heat sources obstructing and diverting contaminated air flow currents toward the incision. This may be caused by personnel or equipment such as ceiling lamps, image intensifiers (Fig. 2), and warming devices. A specific issue with vertical LAF is that of peripheral entrainment (Fig. 3) that is caused by personnel standing at the periphery of the enclosure. The exponential-flow modification utilizes a higher velocity of central air flow creating a down and outward trumpet-shaped flow of air that has been associated with lower rates of SSI [12]. Air temperature and humidity are controlled independently and are a separate function of the air conditioning system. Both have the ability to affect air flow through convection current gradients.

Vertical laminar air flow (black line = air flow currents). HEPA = high-efficiency particulate air filter.
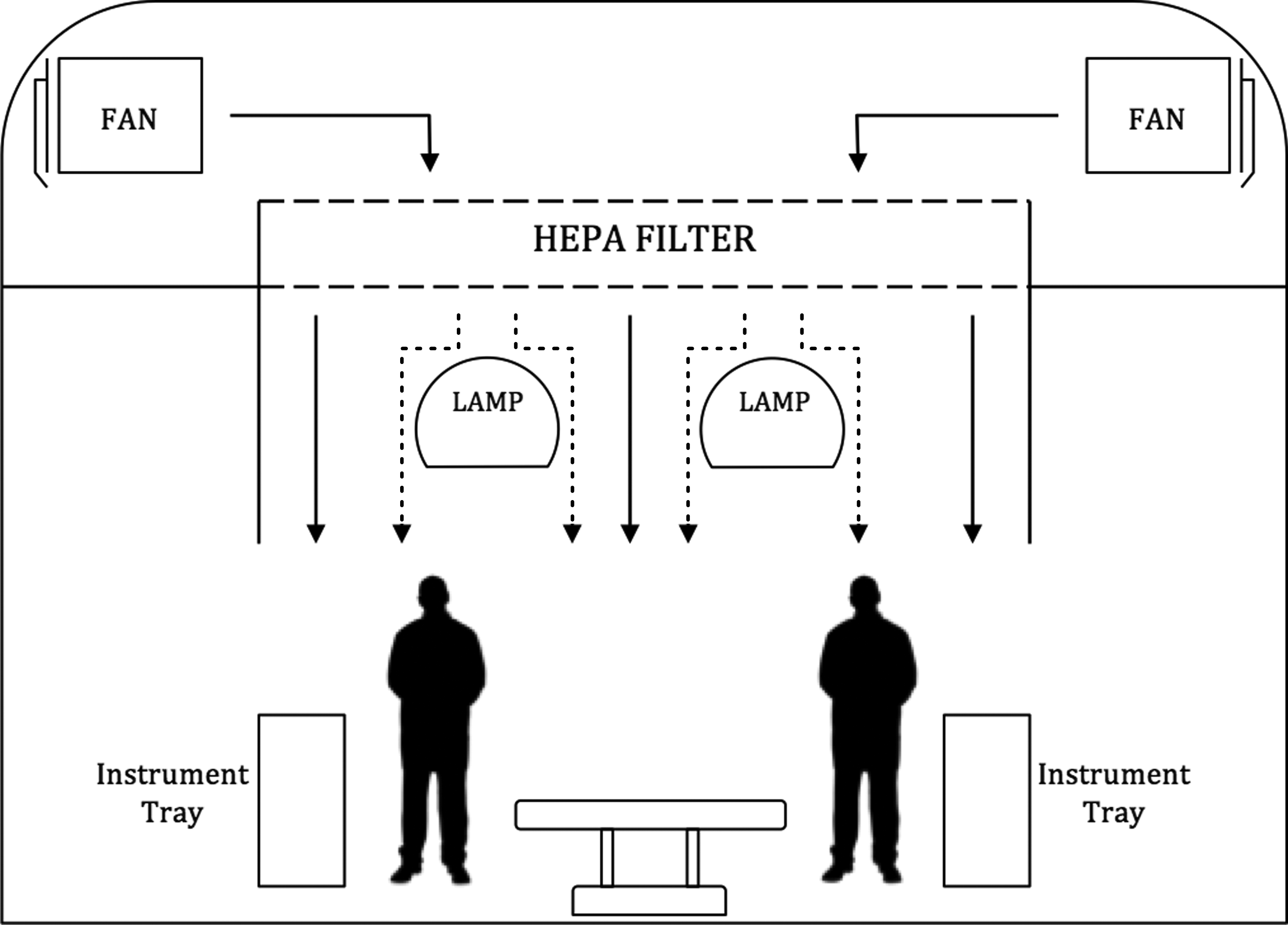
Effect of ceiling light on laminar air flow (dotted lines = turbulent and contaminated air flow currents). HEPA = high-efficiency particulate air filter.
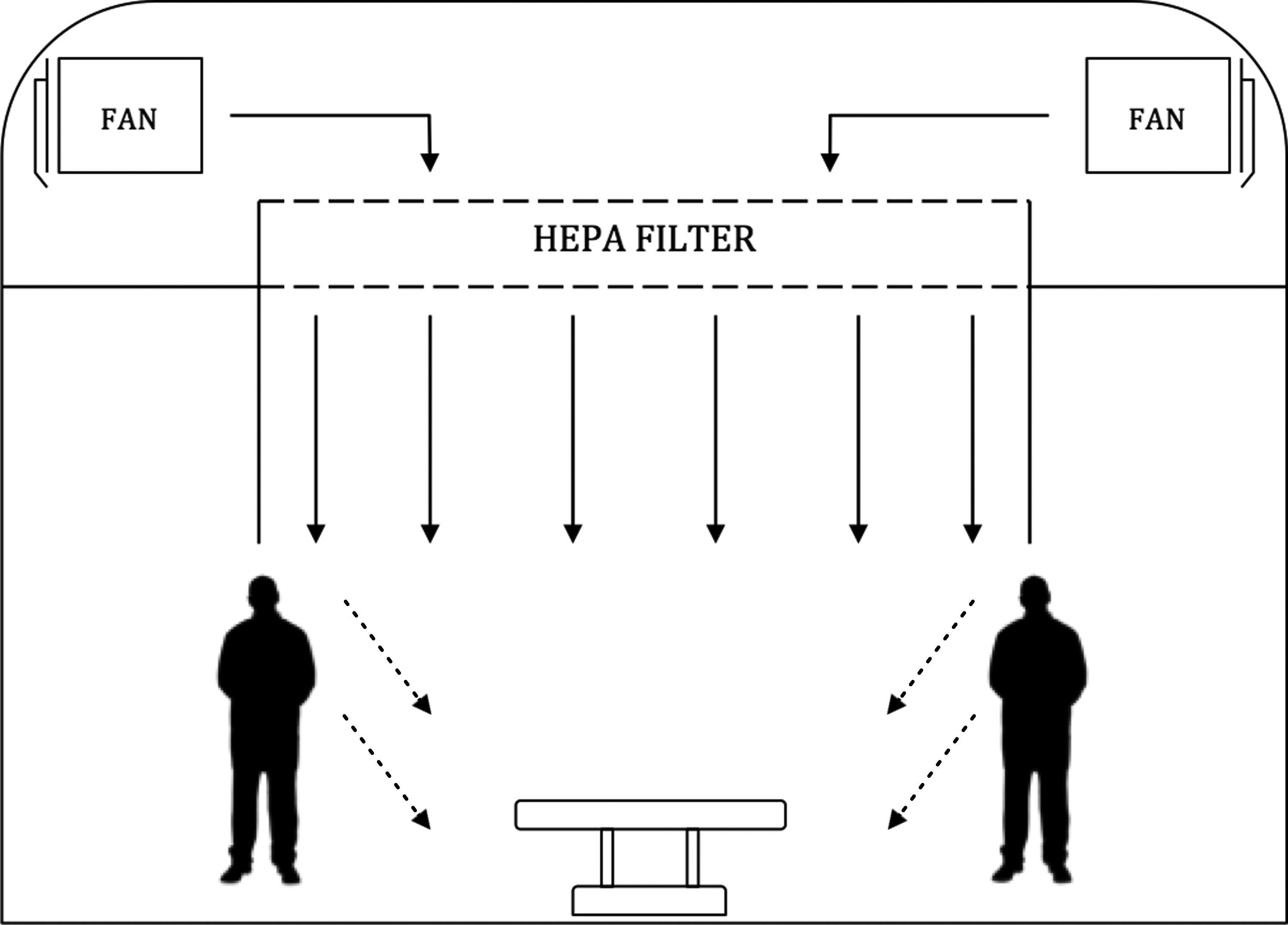
Peripheral entrainment (dotted lines = contaminated air flow currents). HEPA = high-efficiency particulate air filter.
Evidence in Lower Limb Arthroplasty Surgery
Deep periprosthetic joint infection (PJI) is a major cause of implant failure and is associated with substantial morbidity and economic burden [13]. Although its incidence is declining, it remains one of the most challenging complications to treat. Sir John Charnley was a pioneer of total hip arthroplasty (THA) and contributed substantially to the widespread introduction of LAF in joint replacement surgery. In 1969, he reported a PJI rate of 9.5% in a large series of THAs and began to focus on preventing infection through air quality control [14]. Along with air conditioning engineer, Hugh Howorth, he designed a purpose-built ultraclean LAF enclosure that functioned as a separate “room within a room.” In combination with occlusive operating exhaust gowns, he reduced his PJI rate to 0.5% [15]. As LAF gradually became a culturally accepted standard, a landmark study by Lidwell et al. [16] was published in 1982 that provided further evidence supporting its use. This multi-center randomized controlled trial involved 8,055 hip and knee replacements and compared LAF systems to conventional theaters and body exhaust suits to conventional clothing. Vertical LAF and body exhaust suits were associated with the lowest rate of PJI (0.1%) and the lowest bacterial air count (0.4 bacteria carrying particles per cubic meter). When prophylactic antibiotic agents were used with LAF, the rate of PJI reduced substantially from 3.4% to 0.3%. Limitations of the study were non-standardized randomization protocols, different LAF systems, differences in operating room practice, and a subjective definition of PJI. Despite these methodological flaws, this study provided strong evidence supporting LAF systems. In a series of 3,175 arthroplasties, Salvati et al. [17] reported a reduced PJI rate after THA (2.0% to 1.2%) but an increased PJI rate after total knee arthroplasty (TKA; 1.9% to 3.9%) with horizontal LAF. A sub-analysis of confounding factors such as age, diagnosis, comorbidity, surgeon experience, and duration of surgery could not explain this difference but the authors highlighted concerns over the disruptive effect of operating room personnel on clean horizontal airstreams. In a randomized study of 90 patients, Ahl et al. [18] found that the combination of horizontal LAF and occlusive theater clothing resulted in substantially lower air contamination than conventional air flow and cotton garments in TKA, but this effect was less marked during THA. Furthermore, in a series of 435 uncemented hip hemiarthroplasties, Kakwani et al. [19] found a substantially higher re-operation rate for PJI when patients underwent surgery in a conventional theater compared with an LAF theater (4% versus 0%).
More recently, there has been an increasing body of registry-based evidence that disputes the clinical efficacy of LAF. An analysis of 41,212 THAs and 20,554 TKAs from the German nosocomial infection surveillance system determined that hospitals with LAF systems had similar PJI rates to hospitals with conventional ventilation [20]. An interrogation of 51,485 THAs and 36,826 TKAs from the New Zealand Joint Registry found a substantially higher rate of early revision for PJI when procedures were performed with LAF compared with a conventional theater (0.148% vs. 0.061%) [21]. A higher rate of early revision for PJI was also observed when space suits were used compared with conventional clothing (0.186% vs. 0.064%) [21]. A more recent analysis of 91,585 THAs from the same registry observed nearly a two-fold risk of revision for PJI within six months with LAF compared with conventional ventilation [22]. Data from the UK National Joint Registry has also been used to analyze the effect of LAF. In comparative series of 4,915 THAs and 5,928 TKAs, there was no substantial difference between LAF and conventional ventilation in the rate of SSI (0.92% vs. 1.14%, respectively) or revision for infection (0.53% vs. 0.45%, respectively) [23]. A meta-analysis of 196,819 hip or knee replacements performed by Gastmeier et al. [24] revealed a higher risk of SSI with LAF (relative risks of 1.71 and 1.36 for THA and TKA, respectively) compared with conventional ventilation. Bischoff et al. [25] performed a more recent meta-analysis of 12 studies consisting of 330,146 THAs and 134,368 TKAs that showed no substantial difference in PJI risk for LAF compared with conventional ventilation (odds ratio 1.29 and 1.08 for THA and TKA, respectively). Based on these studies, the World Health Organization has now advised against the use of LAF to reduce the risk of SSI for patients undergoing arthroplasty surgery [26]. More recently, an International Consensus Meeting on PJI has also agreed that LAF is not necessary for elective joint arthroplasty surgery [27]. However, it is recognized that these recommendations are based on low to moderate quality of evidence. A summary of the evidence in hip and knee replacement surgery is presented in Table 1.
Summary of Evidence in Hip and Knee Replacement Surgery
LAF = laminar air flow (experimental group); CV = conventional ventilation (control group); PJI = periprosthetic joint infection; RCT = randomized controlled trial; RCS = retrospective comparative study; THA = total hip arthroplasty; TKA total knee arthroplasty; CS = case series; MA = meta-analysis.
The financial implications of installing LAF in hospital operating suites has also undergone cross examination. The costs for building and installing an exponential LAF system into a new operating room is estimated to range from $60,000 to $90,000 [28] whereas the estimated cost of treating an infected THA or TKA is approximately $88,623 to $116,383 [29,30]. An Italian study reported a 24% increase in building costs for LAF but this represented only a 5% increase compared with installing conventional ventilation [31]. A German study concluded that, based on performing four operations per day, the cost per patient was lower for those undergoing surgery in LAF compared with conventional systems [32]. An Australian cost-effectiveness analysis of infection prevention strategies in THA showed that although using antibiotic prophylaxis and antibiotic-impregnated cement lead to substantial improvements in health economic outcomes, the routine use of LAF was associated with a substantial cost increase of AUD $4.59 million and a negative effect on health outcomes [33]. This health economic analysis was based on a hypothetical model and is prone to bias from numerous clinical assumptions. Caution must therefore be applied when extrapolating these conclusions to different populations and timescales.
There are a number of possible explanations for the discrepancies seen in the published data on LAF. Most importantly, the etiology behind PJI is multi-factorial and involves a large number of risk factors many of which remain controversial and continue to be investigated. The overall rate of PJI is extremely low and in order to reduce the confounding effect of the many variables associated with infection, contemporary large-scale randomized controlled trials with sufficient statistical power would be required. Unfortunately, these types of study are limited by practical and financial constraints and may be unrealistic to achieve. Although joint registries can provide large data sets, these are not designed to calculate the efficacy of LAF and may introduce bias through under-reporting of infections, especially if not revised, and variations in infection control practice. Also, effective LAF is dependent on the operating room environment that is highly inconsistent between hospitals. Registry studies cannot take these factors into account and attempting to control this for a multi-center clinical trial would be unworkable. Laminar air flow systems and HEPA filtration units require regular maintenance because their functionality deteriorates with use. None of the presented studies attempted to verify the correct performance of the clean air systems under evaluation. This represents another important drawback because even small failures can result in a harmful effect on air quality [34].
Evidence in Non-Arthroplasty Surgery
The literature reporting on LAF in non-arthroplasty surgery is equally divided. Greunberg et al. [35] concluded from a comparative series of 179 patients undergoing posterior instrumented spinal fusion that LAF reduced wound infection rates substantially (12.9% vs. 0% in the conventional and LAF groups, respectively) [35]. However, patients were not randomly assigned and selection bias was introduced by favoring LAF for cases that were thought to carry a high infection risk. A multivariable analysis of 991 cardiothoracic surgery patients undergoing sternotomy showed an overall infection rate of 4.1% and found that conventional ventilation was an independent risk factor for wound infection [36]. A prospective multi-center cohort study of 2,091 patients undergoing gastric surgery also revealed that conventional ventilation was independently associated with a substantially increased risk of SSI [37]. In a comparative database review of 170 open vascular surgical procedures, Bosanquet et al. [38] reported a higher rate of SSI with conventional ventilation compared with LAF (17% vs. 7%, respectively) and also noted that SSI occurred at a higher rate in patients undergoing arterial bypass grafting procedures. The rate of SSI in this high-risk group was substantially higher with conventional ventilation compared with LAF (33% vs. 11%, respectively). A recent investigation into airborne bacterial contamination during minor orthopedic surgery found that compared with LAF, conventional ventilation increased bacterial counts substantially [39].
In contrast to these reports, others have found no benefit from LAF. Pinder et al. [40] performed a search of England's Hospital Episode Statistics (HES) database to evaluate the effect of ventilation on the rate of infection in 803,065 patients undergoing orthopedic trauma operations [40]. At 90 days, the observed SSI rate was similar for conventional ventilation and LAF (2.4% vs. 2.7%, respectively). The study also reported that hip hemiarthroplasties had a substantially higher SSI rate when performed in LAF compared with conventional theaters (3.8% and 2.6%, respectively) but was open to experimental bias because LAF status was determined through postal and telephone survey and may be subject to error. Hospital Episode Statistics data may also have poor specificity when used to identify infected cases (unpublished data). Additionally, some hospitals in the study (9.8%) used conventional theaters on weekends because LAF was not available and this may have caused an unintended cross-over effect. In their meta-analysis of 63,472 abdominal and open vascular procedures, Bischoff et al. [25] also found no notable difference in overall SSI risk for LAF compared with conventional ventilation (odds ratio 0.75).
Effect of Operating Room Environment
An important confounder on the clinical benefits of LAF is the detrimental effect of turbulence on clean airstreams. Laminar airflow alone does not guarantee ultraclean air because it is critically dependent on environmental factors such as direction of air flow, operating room equipment, personnel, door openings, and patient warming devices. Vertical LAF may be obstructed by objects positioned directly over the surgical field such as theater lights, image intensifiers, and surgeons' heads while horizontal LAF can also be interrupted by theater personnel and instrument tables at the periphery of the operating table. Both can cause bacteria-carrying particles to fall and aggregate on the surgical field leading to SSI. To investigate each type of LAF, Sadrizadeh and Holmberg [41] developed a computational fluid dynamics system to predict the air flow field in an operating room model. Simulated air sampling techniques revealed that horizontal LAF resulted in significantly fewer bacteria-carrying particles than vertical LAF and this was largely attributed to the detrimental effect of ceiling lamps on downward currents. In addition, thermal convection currents produced by operating lights and theater personnel had a far greater impact on vertical air streams. Refai et al. [42] showed a similar negative effect of ceiling operating lights on vertical LAF using neutral buoyancy helium bubbles to represent air particles during simulated TKA. Lights placed directly above the operative field were seen to eliminate unidirectional air flow and even lead to air particles rising to touch the non-sterile lamp before falling down onto the surgical field. However, both the absence of lights and lights placed 160 cm apart were effective in restoring LAF and moving air particles away from the surgical field.
The physical movements of theater personnel can also disrupt air flow currents. Noguchi et al. [43] investigated the generation and behavior of air particles during simulated TKA using a fine particle visualization system filmed with a highly sensitive camera. A large number of air particles were observed while unfolding surgical gowns, changing gloves, and draping the leg although fewer particles were detected under LAF compared with a non-ventilated room. These findings indicate that physical actions should be limited when in proximity to the surgical field and instrument trays [43]. Rezapoor et al. [44] measured the number of air particles in simulated operating room conditions and reported a positive correlation between the number of personnel and door openings on the number of particles measured within the LAF enclosure. The adverse effect of multiple door openings on LAF has been confirmed in several other studies [45,46]. Anesthetic screening drapes, colloquially termed the blood-brain barrier, have also been shown to disturb vertical LAF by reducing downward air velocity and causing turbulence [47].
A similar effect is also seen with the use of forced-air warming devices that can result in temperature gradients and convection currents that obstruct the downward flow of ultraclean air [48]. Within a laminar flow theater, McGovern et al. [49] compared forced-air warming devices to air-free conductive fabric warming blankets and showed that they were associated with substantially higher numbers of simulated particles over the operative field and substantially higher rates of post-operative PJI. It was proposed that this may be an explanatory factor in the changed fortunes of LAF when this warming method was introduced. In a predictive fluid flow simulation model, He et al. [50] illustrated substantial disruption to LAF currents around the operating table with forced-air warming blankets. Simulated skin cells initially were seen to rise with thermal convection currents created by the forced-air warmer, sometimes touching the non-sterile ceiling, then forced downwards toward the operative site by vertical LAF. Therefore, forced-air warmers could be considered detrimental to effective LAF and has been recognized in National Institute for Health and Care Excellence guidelines on peri-operative warming in orthopedic surgery [51]. Recommendations for effective LAF use are shown in Table 2.
Recommendations for Effective Laminar Air Flow Use
Conclusion
The etiology of SSI is multi-factorial and successful infection prevention strategies must consider the patient pathway in its entirety. The importance of appropriate theater ventilation must not be underestimated and meticulous attention to detail is required for it to be used effectively. Currently, the evidence behind LAF remains conflicting with recent meta-analyses not supporting it routine use. These are largely based on cohort studies that are prone to experimental bias because of their low methodological quality. The only randomized trial supports its use but conducting a contemporary large-scale prospective randomized study of the appropriate scientific standard is unlikely to be realistic or financially viable. Abandoning LAF based on recent evidence may be premature and instead consideration must be given to using it more effectively with respect to potential disrupters such as heat sources and physical barriers.
Footnotes
Author Disclosure Statement
No competing financial interests exist.