
Abstract
Abstract
Purpose:
To survey current intensive care unit (ICU) practice in initiating antifungal therapy for prophylaxis and treatment of suspected candidiasis after abdominal surgery. The goal was to establish the need to prioritize research toward standardized care of such patients.
Methods:
Online questionnaire survey of clinical practice based on theoretical case scenarios. These were structured with expert input to investigate management of: hemodynamically stable/unstable patient after urgent upper/lower gastrointestinal surgery with/without fungal growth in culture. The link to the survey was sent to all active members of the European Society of Intensive Care Medicine (ESICM).
Results:
The survey was completed by 101 respondents from 29 countries. Fewer than half (48.5%) stated that in their center, ICU antibiotic and antifungal therapy is managed by a dedicated specialist physician/team that manages all ICU patients. Respondents exhibited a greater tendency toward administering antifungal agents, mainly fluconazole, to hemodynamically unstable patients. One week after surgery for a perforated duodenal ulcer, only half responded they would use antifungal agents when a patient develops septic shock. Most respondents chose to administer antifungal therapy in patients with septic shock if Candida had been identified in any culture. The source of infection, location of surgery, or type of Candida were not viewed as triggers for therapeutic decisions.
Conclusion:
The current survey demonstrates large variability in antifungal use. Decisions are made irrespective of existing guidelines and seem to be driven by patient hemodynamic condition and identification of any Candida in any culture alone.
Candida spp. is the most common invasive yeast infection in intensive care unit (ICU) patients [1]. Invasive candidiasis includes both blood stream infection (i.e., candidemia) or deep-seated tissue infection [2]. Although most research to date has focused on candidemia, during the last two decades it has become increasingly clear that invasive candidiasis can be a life-threatening complication in ICU patients [3–5]. The most common source of invasive fungal infection in immune-competent patients is intra-abdominal. Based on studies demonstrating a 40% rate of intra-abdominal candidiasis among patients with secondary or tertiary peritonitis, the 2016 guidelines published by the Infectious Diseases Society of America recommend that: “Empiric antifungal therapy should be considered for patients with clinical evidence of intra-abdominal infection and significant risk factors for candidiasis, including recent abdominal surgery, anastomotic leaks, or necrotizing pancreatitis.” The guidelines state that the duration of therapy should be determined by clinical response [6]. The European Society of Clinical Microbiology and Infectious Diseases support prophylactic administration of fluconazole in any patient with recent abdominal surgery and recurrent gastrointestinal perforations or anastomotic leakages [7].
A recent meta-analysis reported that administration of prophylactic antifungal treatment (i.e., fluconazole, ketoconazole) was associated with a 50% reduction in the rate of invasive fungal infections and a reduction in mortality rate by one-quarter in ICU patients [8]. However, this meta-analysis has been criticized that it extracted a signal that does not really exist, because all the studies it included had small sample sizes and none showed any such reduction. However, in real life, this finding translated into 100–200 patients needing to be treated in order to prevent a single episode of infection. This approach may not be justifiable given the theoretical concerns regarding the development of late complications in patients with prolonged antifungal therapy [9] as well as questions regarding the evolution of antifungal drug-resistant strains [10–12]. A later meta-analysis did not add much information as it noted that “untargeted antifungal treatment may be associated with a reduction of invasive fungal infections, but the quality of evidence is (still) low” [13].
We set out to survey current practice in initiating Candida prophylaxis and treating suspected abdominal candidiasis in ICU patients after abdominal surgery. Our aim was to establish whether there is a need to prioritize clinical research on this topic and standardize the care of such patients.
Materials and Methods
The study was an online, non-interventional questionnaire survey based on theoretical case scenarios mailed to all members of the European Society of Intensive Care Medicine (ESICM).
Study population
The physicians included in the survey constitute a convenience sample of ICU physicians who chose to respond to the online survey posted by the ESIC to active members of the society (n = 8,500). Physicians interested in intensive care medicine may register to become an ESICM member regardless of place of residence. Membership is approved following proof of professional training and is maintained by payment of membership dues. The study had no exclusion or withdrawal criteria.
Questionnaire structure
The questionnaire comprised two parts; the first included a series of case scenarios whereupon respondents were requested to provide information regarding their choice of action in the specific situation and the second included several questions regarding the respondents' professional expertise and their workplace. The case scenarios were constructed for the purpose of this study and underwent content validity testing by two experts in infectious diseases (D.R. and T.L.) and three experts in intensive care (S.E., M.L., and C.M.).
The scenarios were constructed with the intent to study the inclination of the physician to provide antifungal therapy in clinical situations involving upper gastrointestinal surgery, lower gastrointestinal surgery, or pancreatitis. Some scenarios included similar disease states accompanied by no hemodynamic compromise or severe hemodynamic compromise. Others described patients with similar hemodynamic stability and clinical presentation but with different surgical diagnoses. Others presented similar surgical diagnoses and clinical presentation accompanied by different growth in cultures (Table 1). The questions asked in relation to these scenarios addressed the preferences of the responding physician with regards to antifungal therapy; whether to prescribe antifungal agents, if yes, which antifungal agent to prescribe and, in specific scenarios, what loading dose to prescribe.
List of Scenarios
GI = gastrointestinal; ICU = intensive care unit.
The respondents were informed that all scenarios related to patients who are immune competent (i.e., not receiving chemotherapy or not receiving steroids unless indicated for adrenal replacement therapy in sepsis), have normal liver and kidney function, no previous comorbid conditions, and are being managed in an ICU setting. They were also told to assume all infections are community acquired unless information provided in the question specifically suggested otherwise.
Survey method
The questionnaire was made accessible online using the survey development cloud-based software SurveyMonkey® (SurveyMonkey, Portland, OR). Reminders to complete the questionnaire were mailed to potential participants three times at one-month intervals. Those who entered the survey received information regarding the target audience of the survey and regarding the survey aims (in writing, on the first page of the survey). It was clarified that the survey was intended for practicing ICU physicians only; respondents were requested to complete the survey only if they were currently employed as a specialist working in an ICU. They were also informed that participation in the survey was entirely voluntary, that participant responses would remain anonymous, and that survey completion implied consent to use the responses/data for research. The survey was offered only in English. All the study data were stored in an encrypted and password-secured drive; back-end access to the online survey tool was restricted to the ESICM research staff only.
Statistical analysis
Data were analyzed using SPSS Inc. software (SPSS Statistics for Windows, Version 17.0. Chicago, IL). The primary outcome measure was the proportion of practitioners supporting each type of treatment. Descriptive statistics alone were used throughout data analysis. This included counts, percentages, means with their standard deviations and medians with their interquartile ranges and ranges as required. Surveys were included only if they were more than 80% complete. Percentages were all calculated from the total cohort.
Results
Based on data provided during the registration process to ESICM, approximately one-third of the 8,500 ESICM members receiving the mail survey may have been eligible to participate in the study. A total of 101 responses were received from 29 countries. Among these, 84 respondents (83.2%) stated that they practice medicine in 19 countries within Europe and 17 respondents stated that they practice medicine in 10 countries outside Europe. More than a half of the respondents (51.5%, n = 52) stated that their hospital was an academic center or affiliated with a university and that the majority of their practice was within the public sector (57.4%, n = 58). The majority of respondents (56.4%, n = 57) stated that they worked in a mixed medical/surgical ICU and the average number of beds in their ICUs is 19.3 ± 14.1 (median, 16; interquartile range, [IQR] 9–24).
Antimicrobial protocols and stewardship
Almost one-third of the respondents (31.7%, n = 32) were either unwilling or unable to provide information regarding the existence of antibiotic protocols and stewardship in their ICUs (Table 2). Less than half of the respondents (48.5%, n = 49) stated that in their ICU, antibiotic therapy is managed by the dedicated specialist physician/team that also covers the overall care of all the ICU patients. One-fifth (18.8%, n = 19) stated that antibiotic therapy is managed by individual physicians who manage their own patients when they are admitted to the ICU.
Availability of Antibiotic Protocols and Stewardship
ICU = intensive care unit.
Prophylactic antifungal therapy (yes/no) for a hemodynamically stable versus a hemodynamically unstable patient when no cultures are available
Clinicians seemed more inclined to administer prophylactic antifungal therapy when their patient was hemodynamically unstable than when their patient was hemodynamically stable with upper gastrointestinal/disease but not with lower gastrointestinal surgery (Fig. 1). The proportion of physicians who elected to administer prophylactic antifungal agents to a patient with a perforated gastric/duodenal ulcer was 34% if the patient was unstable and 19% if the patient was stable (p = 0.002). The proportion of physicians who elected to administer prophylactic antifungal agents to a patient with acute necrotizing pancreatitis was 45% if the patient was unstable and 21% if the patient was stable (p = 0.005). Conversely, the proportion of physicians who elected to administer prophylactic antifungal agents to a patient with a perforated large bowel diverticulum with local peritonitis or to a patient with fecal peritonitis did not differ regardless of whether the patient was unstable or stable (for diverticulum, 44% and 31%, respectively [not significant], and for fecal peritonitis 53% and 44% [NS]).
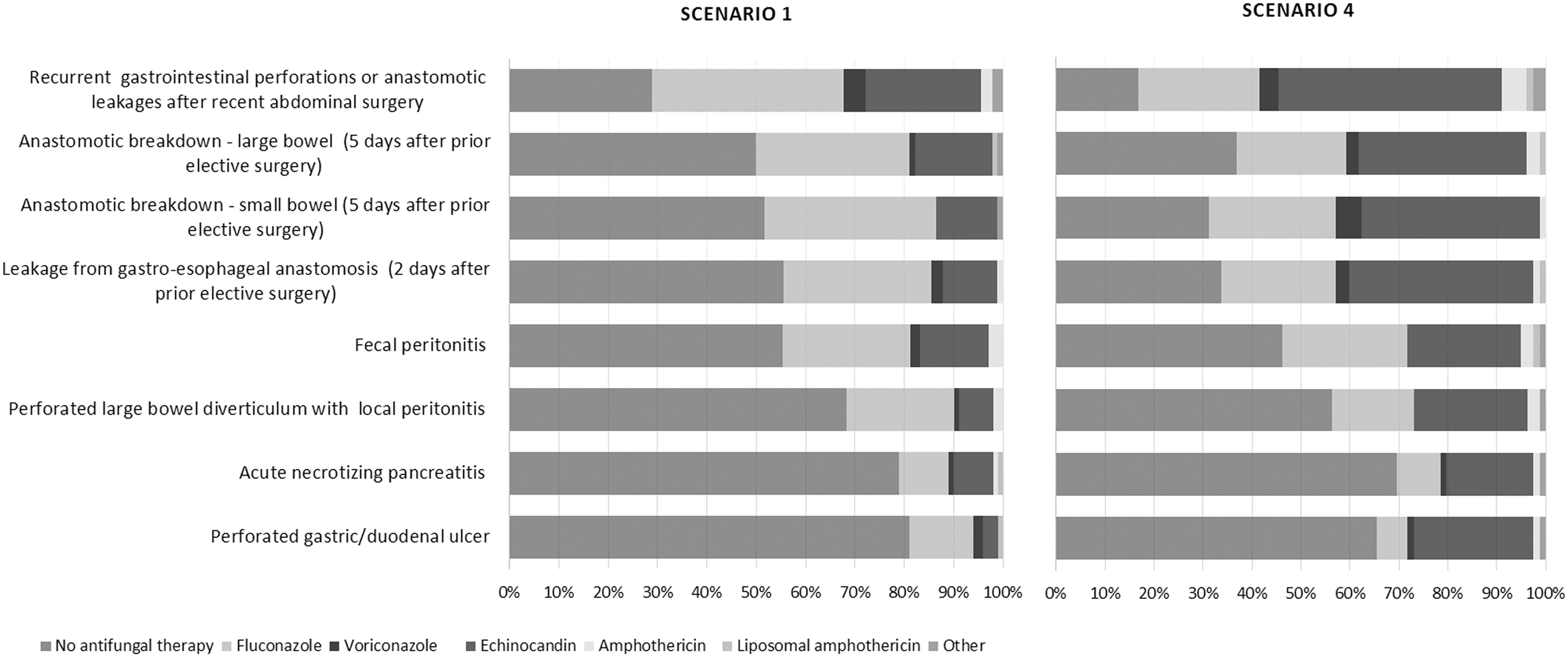
Choice of antifungal prophylaxis for a recently admitted intensive care unit (ICU) patient who is hemodynamically stable (scenario 1) versus hemodynamically unstable (scenario 4), when cultures are unavailable, based only on intra-operative findings.
Choice of fluconazole versus another antifungal agent
For a hemodynamically stable patient who has an abdominal culture with fungal growth (information was provided that the isolate is susceptible to fluconazole), the majority of respondents (>80%) chose to administer fluconazole rather than another antifungal agent regardless of whether the patient had undergone lower gastrointestinal surgery for perforated diverticulitis two days prior and has no clinical signs of infection or had upper gastrointestinal surgery for perforated duodenal ulcer two days prior and has clinical signs of infection (Fig. 2, left panel, p = 0.99). When the patient was admitted immediately after urgent surgery for a perforated duodenal ulcer and was noted to be hemodynamically unstable and no cultures were available, more than half of the physicians still chose fluconazole versus other antifungal regimens (85% vs. 56%, p < 0.001) (Fig. 2, left panel).

Choice of antifungal treatment (fluconazole vs. other) in the following clinical situations. A hemodynamically stable patient, post-lower gastrointestinal surgery with no clinical signs of infection, but with fungal growth in abdominal culture (scenario 2). A hemodynamically stable patient, post-upper gastrointestinal surgery who presents with clinical signs of infection and fungal growth in abdominal culture (scenario 3). A hemodynamically unstable patient post-upper gastrointestinal surgery when no cultures are available (scenario 5). A hemodynamically unstable patient, one week after upper gastrointestinal surgery with mixed growth in single abdominal culture (scenario 6). A hemodynamically unstable patient, one week after upper gastrointestinal surgery with fungal growth in two non-abdominal cultures (scenario 8). A patient in septic shock one week after perforation of a duodenal ulcer that has received no prior antifungal coverage with a culture taken from the abdomen during surgery growing either Candida albicans (scenario 7A) or non-Candida albicans (scenario 7B).
For a patient who had undergone urgent surgery for perforated duodenal ulcer and is already being treated with broad-spectrum antibiotics (but not antifungal therapy) but who then develops hemodynamic instability one week after surgery, the proportion of respondents choosing to administer fluconazole rather than another antifungal agent was 33% when the abdominal culture yielded mixed bacterial and fungal growth versus 47% when there was fungal growth from two non-abdominal sources (Fig. 2, middle panel; p = 0.01).
When the clinical case scenario described a hemodynamically unstable patient one week after perforation of a duodenal ulcer and the culture taken from the abdomen during surgery grew only Candida albicans, almost half of the respondents (48%) still chose not to administer fluconazole. Conversely, when the culture grew non-Candida albicans spp., six respondents continued to choose to administer fluconazole (Fig. 2, right panel).
Monitoring of azole concentrations and loading dose of fluconazole
Regardless of the clinical scenario presented (Table 1), the majority of respondents (81%–87%) elected to administer either 800 mg or 400 mg of fluconazole as a loading dose prior to initiating therapy. A loading dose of 800 mg was selected by 16% of respondents for hemodynamically stable patients with no clinical sign of infection. The rate increased to 40% if clinical signs of infection were provided. Most respondents stated that their laboratory did not routinely test fluconazole concentrations (61.4%, n = 62) but 28% of the respondents also responded that if specially requested to do so, the laboratory in their hospital could perform this test. The overall average loading dose was 721 ± 156 mg in centers that monitor fluconazole levels vs. 599 ± 234 mg in centers that do not monitor fluconazole levels (Fig. 3). We also examined whether respondents working in centers that monitor the levels of fluconazole would administer higher loading doses of fluconazole than respondents working in centers that do not monitor levels in three scenarios (2, 3, and 5; [Table 1] and found no difference. Given the small number of respondents, this finding should be viewed with caution.
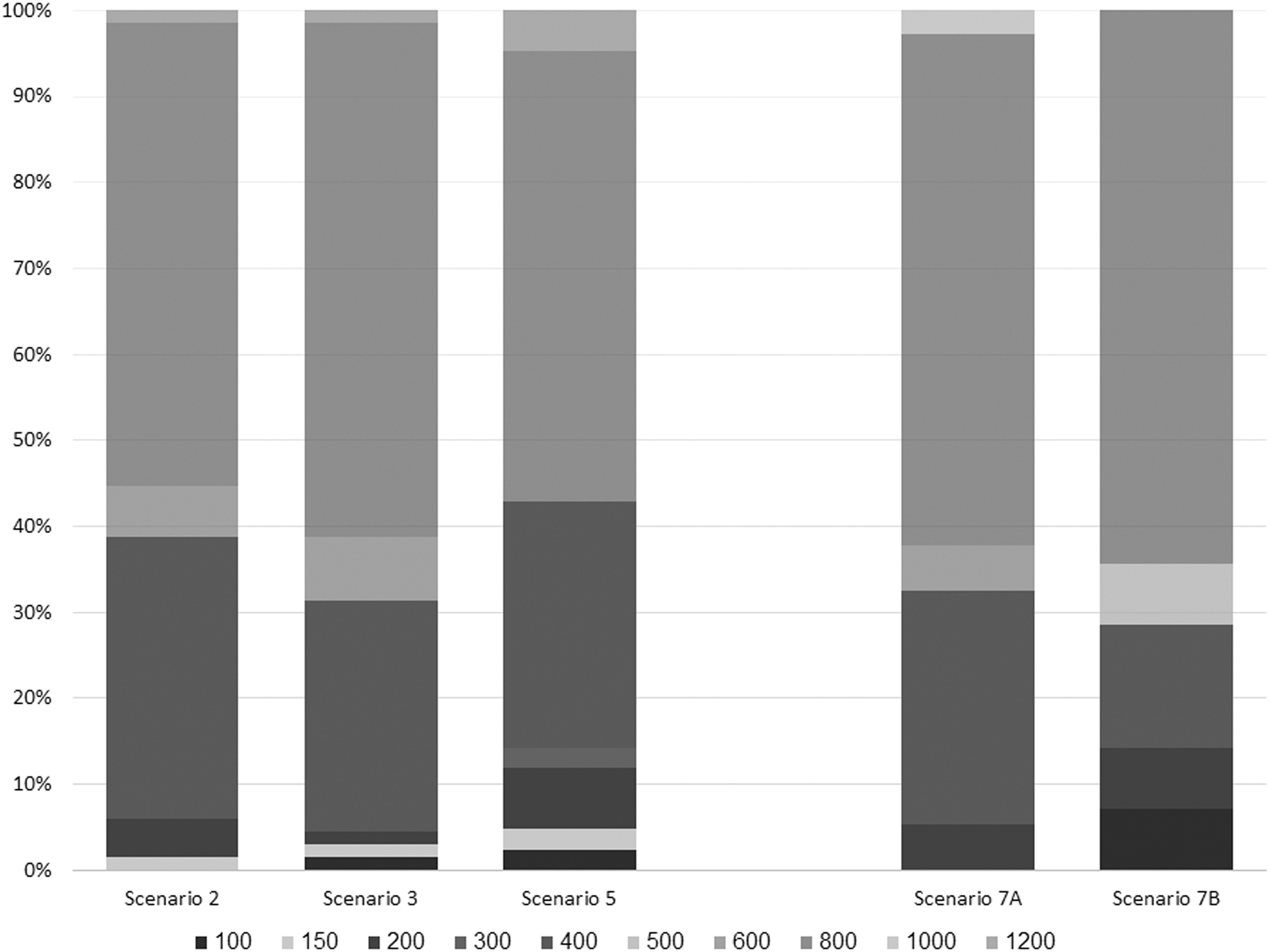
Loading dose of fluconazole selected, given that this antifungal drug had been chosen for treating the following clinical situations: A hemodynamically stable patient, post-lower gastrointestinal surgery with no clinical signs of infection, but with fungal growth in abdominal culture (scenario 2). A hemodynamically stable patient, post-upper gastrointestinal surgery who presents with clinical signs of infection and fungal growth in abdominal culture (scenario 3). A hemodynamically unstable patient post-upper gastrointestinal surgery when no cultures are available (scenario 5). A patient in septic shock one week after perforation of a duodenal ulcer who has received no prior antifungal coverage with a culture taken from the abdomen during surgery growing either Candida albicans (scenario 7A) or non-Candida albicans (scenario 7B).
The relation between the decision regarding administration of antifungal coverage for a patient in septic shock one week after perforation of a duodenal ulcer with no prior antifungal coverage and the reported findings in laboratory cultures
Any fungal growth in the abdominal sample taken during surgery, regardless of whether the growth was isolated fungal or mixed bacterial-fungal, triggered administration of antifungal treatment among most respondents (Fig. 4, left panel). The actual result obtained by culture had little bearing on the decisions made by the respondents with regards to actual administration of any antifungal coverage one week after perforation of a duodenal ulcer.
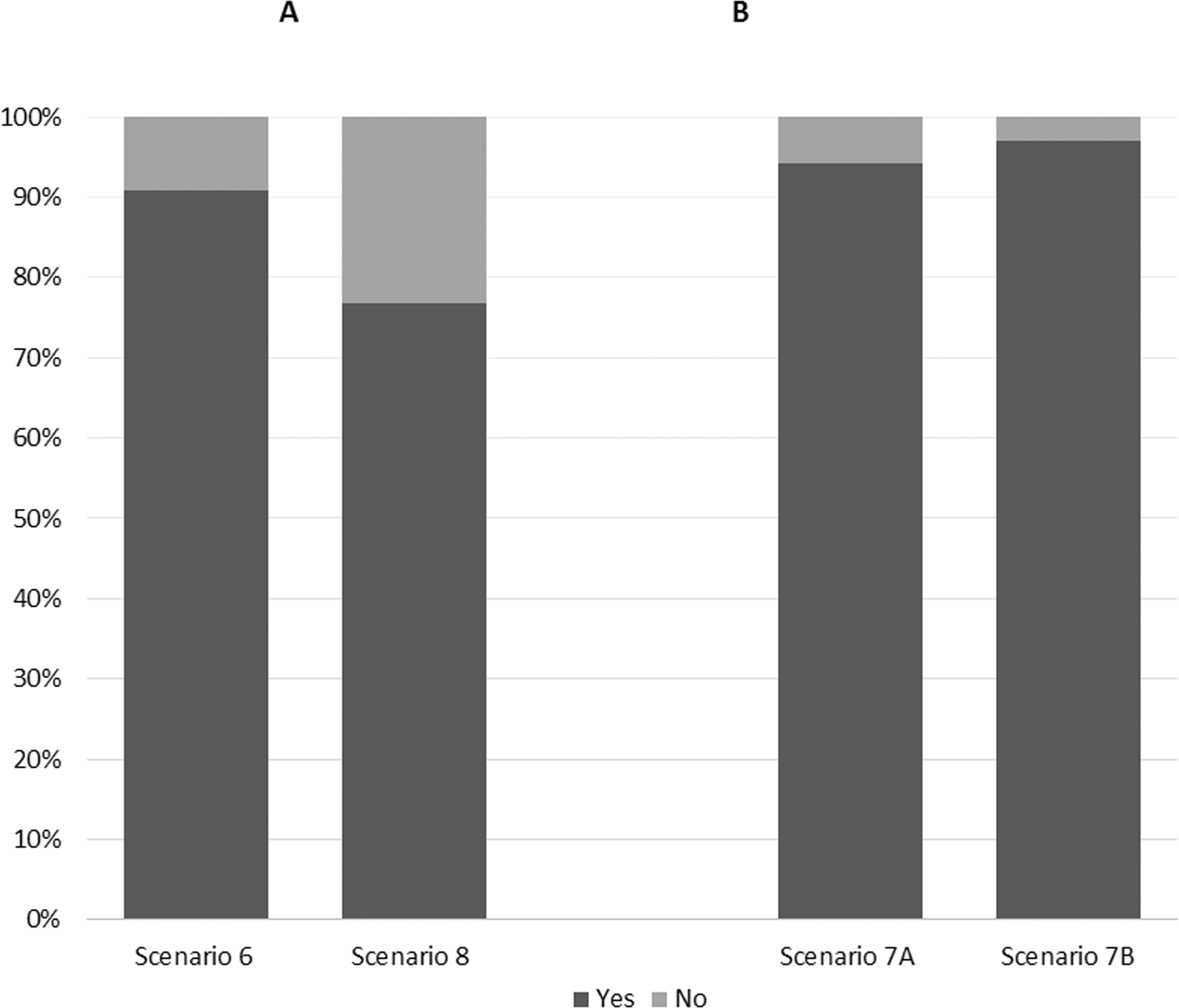
Physician decisions regarding administration of fluconazole coverage for a patient in septic shock one week after perforation of a duodenal ulcer (no prior antifungal coverage) when given information that there had been mixed bacterial and fungal growth in single abdominal culture (scenario 6) versus Candida albicans growth in two non-abdominal cultures (scenario 8) and physician decisions regarding administration of fluconazole coverage in the same clinical situation when given information that there was only fungal growth in the culture taken from the abdomen during surgery and it was either Candida albicans (scenario 7A) or non-Candida albicans (scenario 7B).
Discussion
The current survey demonstrates large variability in the reported practice of antifungal therapy among respondents. Antifungal therapy seems to be guided by the severity of patient condition and the presence of any Candida spp. growth, regardless of clinical circumstances (e.g., type and relation to the time of surgery) or the tissue cultured.
Patients at risk for Candida infection comprise three groups. The first consists of those patients with an acute perforation of a hollow viscus that is naturally colonized by Candida species. Antifungal agents are generally not indicated in such cases because even isolation of Candida in laboratory samples taken during surgery does not necessarily reflect intra-abdominal infection with Candida [1,3,16]. In these cases, questions arise particularly when the patient has septic shock and evidence of peritoneal contamination from an upper gastrointestinal source where fungal colonization is more predominant. Non-response to initial therapy triggers the dilemma regarding the need to cover at least the most common fungal infections.
The second group of patients comprises those with secondary intra-abdominal infection resulting from recurrent gastrointestinal perforations or an anastomotic breakdown after a surgical procedure. Such cases may benefit from early antifungal treatment [17,18] but important questions remain regarding the duration of treatment.
The third group comprises surgical patients who have multiple risk factors for invasive fungal infection. These factors include, among others, a prolonged stay in the ICU (during which broad-spectrum antibiotic coverage is often administered), the presence of multiple intravenous catheters, and the need for parenteral nutrition or renal replacement therapy [19]. In such cases, there may be progressive colonization and invasion with fungal species. Questions regarding antifungal therapy usually begin to be raised after two or three weeks in the ICU. These questions are particularly pertinent in the presence of organ dysfunction or septic shock given the lack of data regarding the impact of treatment delays in life-threatening cases of invasive fungal infection. As noted, a recent meta-analysis has suggested that administration of prophylactic antifungal treatment (i.e., fluconazole, ketoconazole) is associated with reductions in the rate of invasive fungal infections and mortality in ICU patients [8].
To the best of our knowledge, the current study is the only multicenter survey of adherence to antifungal recommendations following abdominal surgery. Recently an expert panel highlighted the need to address specifically the optimal diagnostic and therapeutic strategies for patients with abdominal candidiasis [20]. The case scenarios in this study were constructed with the purpose of eliciting precisely the discrepancies observed given the lack of good quality data. Clinical circumstances may often be more complex, theoretically justifying decisions that do not follow guidelines. Although our response rate was not particularly high, the questionnaire was designed to be complex enough to elicit responses from those with a specific interest in the topic. These responses also represent the opinions of physicians from multiple medical centers.
Ours is not the first study to report discrepancies between guideline recommendations and physician preferences for antifungal therapy. A point prevalence survey conducted among 2,047 ICU patients disclosed that 154 (7.5%) were receiving antifungal agents on a single day, yet two-thirds of these (n = 100) had no documented evidence of fungal infection [21]. De Souza et al. [22] studied adherence to antifungal recommendations in a single medical center in Brazil and found that the overall adherence to treatment guidelines was 29.4%. Nivoix et al. [23] retrospectively studied all ICU oncology and hematology patient charts in a single center in France and noted a 60% overall rate of reasonably appropriate use of antifungal therapy.
Defining actual Candida infection can be challenging; diagnosis of invasive candidiasis often remains an elusive concept and candidemia rarely occurs in non-neutropenic patients [24]. Differentiating between prophylactic, empirical and targeted treatment further complicates matters. The variation in the responses observed in the current study could easily have stemmed from uncertainty regarding definitions. These dilemmas are often compounded by the lack of timeliness (e.g., that of blood cultures) and the lack of consensus regarding the value of some of the tests being used currently to differentiate between clinically important fungal infections versus laboratory growth with no clinical impact. Furthermore, although positive Candida cultures in abdominal samples from patients with intra-abdominal infections have been associated with increased mortality [3,25,26], the use of antifungal agents has never been shown clearly to reduce mortality. Well-conducted randomized clinical trials have thus far failed to confirm that antifungal therapy is beneficial in non-immune–deficient critically ill patients [27]. There is an overall agreement that much research is still required to clarify the optimal therapeutic strategies for antifungal agents [28].
Subtle variations between guidelines for treatment of potential or proven Candida infection may also potentially undermine the treatment practices. The Infectious Disease Society of America recommendation states: “Empiric antifungal therapy for Candida is not recommended for adult and pediatric patients with community-acquired intra-abdominal infection” [6]. In contrast, French guidelines suggest that antifungal therapy should be initiated in any severe peritonitis presenting with at least 3 of the following criteria: hemodynamic failure, female gender, upper gastrointestinal surgery or antibiotic therapy for more than 48 hours [29]. The European Society of Clinical Microbiology and Infectious Diseases Fungal Infection Study Group (EFISG) support the prophylactic use of fluconazole after recent abdominal surgery particularly in case of recurrent gastrointestinal perforations or anastomotic leakages [7].
Treatment availability can also limit guideline implementation and may explain the choice of fluconazole as first-line empirical therapy by the respondents in the current study despite guideline recommendations to administer echinocandins in several of the scenarios that we presented [6,29]. Our respondents represent a relatively diverse set of ICUs, which is interesting in terms of guidelines diffusion, and there has been no prior multicenter survey on this topic. Nonetheless, the current study has several limitations. We studied declared practice, which may not reflect actual practice [30]. The small number of respondents raises concern regarding generalizability and precluded study of the relation between the response and hospital characteristics (e.g., academic vs. non-academic, number of beds). Our study may overestimate the level of knowledge; the willingness of those participating to complete the lengthy questionnaire suggests a priori selection of respondents with particular interest in the topic, and the platform used enabled approach only to physicians who are dues-paying ESICM members (i.e., ICU physicians with greater funding, academic interest, and access to international knowledge exchange). The sample size was not calculated because no other international surveys have been performed on this topic. Therefore, findings should be interpreted with caution; an α-error is possible. Our scenarios did not include data that could be used to score the risk of Candida infection. Scoring methods are mentioned in most guidelines but at this time are often given to individual preference for use [29,30]. Finally, our scenarios were presented in English only.
Conclusion
The present survey suggests that there may be large variability in antifungal therapy. To date, antifungal therapy seems to be guided by the severity of patient condition and the presence of any Candida positive cultures regardless of clinical circumstances (e.g., type and relation to the time of surgery) or the tissue cultured. Validation of these findings would raise important questions regarding the process of guideline diffusion and implementation as well as their relevance. Either way, more in-depth research is required to improve the evidence underlying all existing guidelines and to overcome the obstacles to guideline implementation.
Footnotes
Acknowledgments
The research group as a whole would like to express their gratitude to Prof. Jacques Duranteau who, as chair of the research committee, pushed this project forward within the framework of the ESICM. We also appreciate the work invested by Guy Francois in creating the online format of the survey and in sending timely reminders to members of the ESICM to provide their responses.
This project was not funded but was supported by ESICM who made available the society online survey platform.
The study was a survey of reported practice and information regarding clinical preferences was elicited using fictitious vignettes. The need for ethical approval was therefore waived. Prior to accessing the survey questionnaire, respondents were informed that responding is voluntary, that all information will be kept anonymous and that survey completion implies consent to use the responses/data for research.
Author Disclosure Statement
S.E. has no relevant conflicts of interest but has received funding for travel, given lectures, owns patents with and/or performed consultancy work for Zoll, Medtronic and Diasorin and has participated in multicenter trials run by Artisanpharma, Eisai, and Astra Zeneca. M.L. has relevant conflicts of interest that include lectures for MSD and Pfizer, and non-relevant conflicts of interest such as lectures for LFB and consultancy fees from Aguettant. I.M.L. has lectured on behalf of the Gilead Health Policy advisory board and is a member of the Accelerate advisory board. D.R., T.L., K.B., and C.M. have no conflict of interest