
Abstract
Abstract
Background:
We describe the management and control of an outbreak of mediastinitis in a cardiac surgery department.
Method:
We performed a retrospective cohort study of 87 patients who underwent coronary artery bypass grafting (CABG), valve replacement, or both during a five-month period with a higher than normal number of cases of post-operative mediastinitis. In addition to medical records review, a survey was conducted among surgeons to estimate the frequency of cellulose-derived absorbable hemostatic (CDAH) use.
Results:
Eleven patients (12.5%) developed mediastinitis during the period. None of them died, and the course of the infections was benign. No differences were found between the infected and non-infected patients regarding clinical or demographic characteristics. The rate of infection by surgeon ranged from 0 to 21.4%. (p = 0.38). We found a significant linear relation between the frequency of CDAH use and the risk of infection, from 3.3% to 22.6% (p = 0.024). Cultures of unused CDAHs were negative. Cessation of product use led to no new cases for the following year and to a mediastinitis rate <1% for the following 24 months.
Conclusion:
We identified a cluster of undesired clinical outcomes compatible with mediastinitis that added morbidity and associated cost, but not deaths, related to the use of CDAH as a hemostatic. These data suggest keeping the use of CDAH in cardiothoracic surgery to a minimum.
Post-sternotomy mediastinitis is one of the most serious complications of cardiac surgery. Despite its relatively low incidence, it remains frightful, as it is associated with increased patient morbidity, deaths, and hospital costs [1]. Most series report the incidence of mediastinitis after cardiac surgery to be <2%, but it can be as high as 19% [2,3].
There are many risk factors for mediastinitis, such as older age, obesity, chronic obstructive bronchopneumonia, diabetes mellitus, critical pre-operative condition, need for peri-operative blood transfusion or vasopressor support, prolonged mechanical ventilation, and coronary artery bypass grafting (CABG), especially if using both internal thoracic arteries in female patients [3,4]. In the present study, we describe how an abnormal number of cases of mediastinitis was detected and managed in a tertiary-care hospital from November 2014 to March 2015.
Patients and Methods
The temporal onset of new cases of mediastinitis in the cardiothoracic surgery department of a tertiary-care center in Spain during the period November 1, 2014–March 15, 2015 (epidemic period) is described. The department's caseload encompasses a variety of cardiovascular procedures including heart transplantation. There is an infection control unit on site. It runs a plan for the prevention of surgical site infections (SSIs), including reporting of SSI rates to the surgeons. The plan includes pre-operative preparation of the patient, antimicrobial drug prophylaxis, as well as post-operative prevention measures.
Only patients who underwent CABG, valve replacement, or both were included in this analysis. To confirm the existence of the epidemic SSI rate, the epidemic period was compared with the previous 21 months. The primary end-point was mediastinitis (organ/space SSI as defined by the European Centre for Disease Prevention and Control (ECDC) criteria) [5]. In order to disclose the source of the infection, the clinical records of patients undergoing bypass procedures or valve replacement were reviewed for demographic, clinical, and potential risk factor variables in addition to the variables routinely gathered for the concurrent surveillance system. These included, among others, the type of surgical procedure, pre-operative length of stay, antimicrobial prophylaxis, main surgeon, National Healthcare Safety Network (NHSN) category (American Society of Anesthesiologists (ASA) Index, length of operation, and surgery class). Furthermore, changes that could have occurred since November 2014 were investigated. Finally, a survey was conducted among surgeons to determine the estimated frequency of cellulose-derived absorbable hemostatic (CDAH) use. Unopened samples of CDAH were cultured for bacteria and fungi by standard methods.
Comparisons between groups were performed by the Student t-test or non-parametric tests as appropriate to compare quantitative variables, as well as χ2 and the Fisher exact test to compare categorical variables. A χ2 test for trend was used to test the linearity of the use of CDAH on the risk of mediastinitis. All tests were two-sided with significance set at p < 0.05.
Results
From the beginning of November 2014 until March 15, 2015 (epidemic period), 87 patients were operated on for valve replacement, CABG, or both. Twenty-one of these were combined procedures.
Eleven patients (12.5%) from the total number of patients undergoing bypass procedures (30) or valve replacement (57) developed mediastinitis compared with 1.7% in the pre-epidemic period (January 2013–October 2014) (Fig. 1). The period from operation to diagnosis of infection ranged from 8 to 35 days (mean 18.3 days; median 12 days). The mean age of the total series was 68.6 years (range 43–89), and 49 of them (56.3%) were male. Most patients (88.5%) received cephazolin as antimicrobial prophylaxis. None of the infected patients died (Table 1).
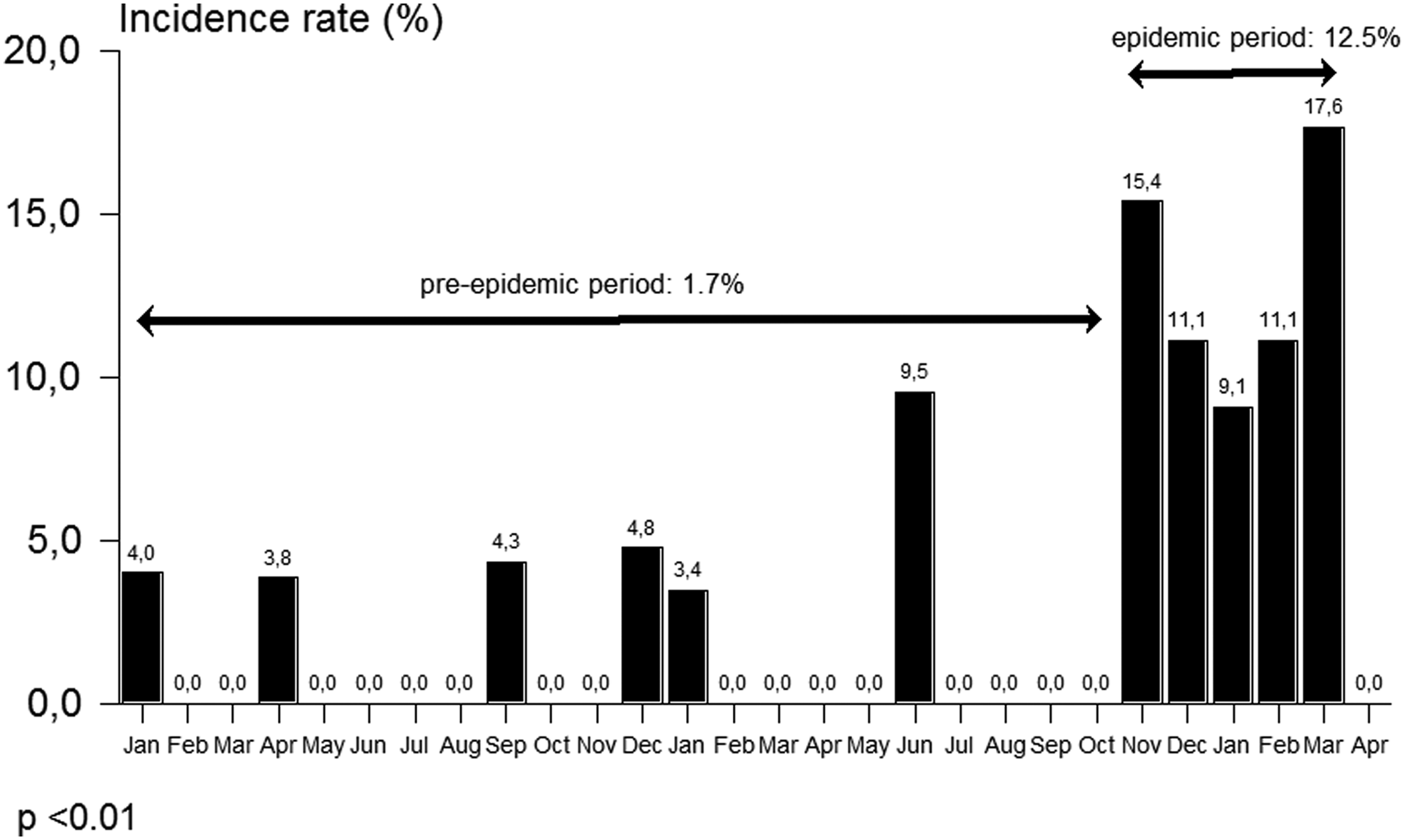
Incidence of mediastinitis by month, January 2013–March 2015.
Demographic Data, Risk Factors, and Outcome of Infected and Uninfected Patients, Epidemic Period (November 2014–March 15, 2015)
No differences were found between the infected and non-infected patients in terms of surgical procedure, demographic characteristics, antibiotic prophylaxis, elective or emergency surgery, pre-operative length of stay, principal surgeon, or ASA score. Infected patients had a trend toward a poor NHSN risk score (2.76 versus 2.20), but the difference did not reach statistical significance. The rate of infection by main surgeon ranged from 0 to 21.4% (p = 0.38).
In eight of the eleven infected patients, incision exudate cultures yielded micro-organisms: Staphylococcus aureus (2); Candida albicans, Propionibacterium acnes, S. epidermidis, Enterobacter cloacae (1 each); and one each of mixed Morganella morganii and S. epidermidis and E. aerogenes and coagulase-negative Staphylococcus.
Aspergillus fumigatus and Aspergillus spp. grew in two of the samples 3–4 weeks after the onset of infection, which was considered post-incision contamination. In the other three patients, the culture results were negative. Routine and ad hoc sampling for filamentous fungi of air from the two operating rooms where the patients were operated on showed negative results.
We conducted a survey of the cardiovascular surgeons to determine the frequency of use of cellulose-derived absorbable hemostatic product (Pahacel®). We found a significant linear relation between the frequency of CDAH use and the risk of infection (p = 0.024). Surgeons who “never” or “almost never” used CDAH had an infection risk of 3.3% (95% confidence interval [CI] 0.17–15.4%); surgeons who used it “sometimes” had a risk of 11.5% (95% CI 3.0–28.3%); and those who used it “always” or “almost always” had a risk of 22.6% (95% CI 10.4–39.6%) (p = 0.024) (Fig. 2).

Effect of use of cellulose-derived absorbable hemostatic product on risk of mediastinitis.
Consequently, on March 13, 2015, a recommendation was issued to discontinue the use of this new CDAH because it was the suspected causal factor. For the 12 months of follow-up after removal of the product from the operating rooms, the incidence of mediastinitis remained as low as 0.
Discussion
A cluster of eleven cases of mediastinitis in cardiothoracic surgical patients over a four-and-a-half-month period was identified, and we describe the research used to identify the cause and to control the outbreak. To our knowledge CDAH has not been identified previously as a risk factor for mediastinitis.
Because of the sharp increase in the rate of mediastinitis in patients operated on from November 2014, factors that could have been modified in the care of the patients were investigated (see Fig. 1). Cardiothoracic surgeons, ward and operating room nurses, and anesthesiologists among others, were interviewed to see if they recalled any new practice trends, devices, or products implemented or used beginning November 1. It soon was realized that a new cellulose-derived absorbable hemostatic had replaced the original product beginning in the summer of 2014. However, no change was evident immediately in the likelihood of mediastinitis, as stocks of the old product remained in place in the operating room (OR) depository and were used until they were gone. As the use of CDAH is at the discretion of the surgeon and no tracking of its use is kept in the clinical records, the individual use of the new product could not be determined.
Sterile, unopened samples of the new CDAH were cultured for bacteria and fungi as soon as we suspected their involvement in the infections, but all of them were negative for micro-organisms. Immediately, the Infection Control Team issued a recommendation of not using the product.
The CDAH was used according to the preference of the surgeon when there was risk of excessive bleeding at the surgical site. Theoretically, the product becomes saturated with blood at the site and swells into a brownish or black gelatinous mass, which aids in the formation of a clot. When used in small amounts, CDAH is absorbed from the site of implantation with little or no tissue reaction. In addition, regenerated cellulose has bactericidal properties. The fabric strip is recommended for use in minimal amounts and is laid on the bleeding site or held firmly against the tissues until hemostasis occurs [6].
In order to establish whether this product increased the risk of mediastinitis, and because the use of the product differed from one surgeon to another, a survey was conducted by asking each principal surgeon to classify from 0 (never) to 5 (always) the frequency of CDAH use during the epidemic period. Because of the small sample, we collapsed the answers into three categories: never or almost never (1), sometimes (2), or always or almost always (3). Those who used it “always” or “almost always” had a higher risk of infection in their patients than those who used it “never,” “almost never,” or “sometimes.”
Although we do not have individualized information about CDAH use in every patient and cannot fully verify this hypothesis, the data on the preference of use of CDAH by surgeons strongly suggest that the new CDHA was the main risk factor for mediastinitis during the epidemic period. As soon as CDAH was suspected and the idea was supported by the epidemiologic data as a risk factor for mediastinitis, the manufacturer was informed of our findings.
This report is the first showing a direct relation between CDAH use in cardiovascular surgery and a diagnosis of mediastinitis, although it is doubtful that these cases truly were mediastinitis or rather were a less serious condition. However, cases complied with the criteria for organ/space SSI issued by the ECDC, were managed as mediastinitis by clinicians, and were associated with a much larger post-operative length of stay than was found in patients without the condition (median post-operative length of stay 49 days versus 10 days; p = 0.002). On the other hand, the clinical course of these patients was favorable, with no sepsis or deaths. Furthermore, a foreign-body reaction to this material has been reported when it is not totally removed, and this could result in sternal dehiscence as well as contamination of the incision and space [7–10]. Even though CDAH is a relatively non-irritating substance and is completely absorbed by the body in most instances, it is nonetheless a foreign body and should be used in the smallest possible amounts.
It should be emphasized that after the cluster of cases was identified, a recommendation was issued not to use the product or indeed any other CDAH product. Surgeons were encouraged to apply other hemostasis strategies. Remarkably, the rate of SSI was as low as zero during the following 12 months (much lower than the 1.7% in the pre-epidemic period), and it has been maintained below 1% until December 2018 (data not shown).
There are some singularities in this cluster of mediastinitis: A single pathogen could not be identified as the causative agent, the product cultures were negative, and the course of the infections was benign. No infected patient required creation of a flap. Site vacuum plus antibiotic therapy was efficacious for the treatment of all patients. In addition, no patient died even though mediastinitis has a high mortality rate [3,4]. The most likely explanation is that the cases were adverse tissue reactions that subsequently became infected with skin or environmental contaminants. Furthermore, removal of the product from the surgical armamentarium was followed by no new cases for the following year and to a mediastinitis rate <1% up to the time of the writing this manuscript.
In conclusion, we report a cluster of undesired clinical outcomes compatible with mediastinitis that added morbidity and associated cost, but not death, to the patients, related to the use of a particular brand of CDAH as a hemostatic in cardiothoracic surgery. These data suggest the need to keep the use of CDAH to a minimum.
Author Disclosure Statement
The authors report no conflicts of interest relevant to this article. No financial support was received for this work.