
Abstract
Abstract
Background:
Prophylactic antibiotic therapy is given routinely in the peri-operative period to prevent surgical site infection. However, in pediatric cardiac surgery, an optimal schedule has not been defined. Pediatric recommendations follow the guidelines for adults, which might be improper because of the inherent challenges in pediatric research and the heterogeneity of the population. Implementation of an effective prophylaxis protocol is needed for children undergoing cardiac surgery, especially in view of worldwide antibiotic overuse and the development of drug resistance. In this review, we analyze the current knowledge supported by up-to-date publications about antibiotic prophylaxis in pediatric cardiac surgery.
Methods:
The PubMed® database was searched for full-text journal articles describing peri-operative antibiotic prophylaxis in pediatric cardiac surgery published since 2000. Antibiotics used for standard prophylaxis with dosing schema, time of the first dose, additional dosage in extracorporeal circulation (ECC) priming, and prophylaxis duration were analyzed. Additionally, we looked for special clinical situations such as antibiotic prophylaxis in children with the sternum left open after surgery and patients with β-lactam allergy or pre-operative methicillin-resistant Staphylococcus aureus (MRSA) colonization or those requiring extracorporeal membrane oxygenation (ECMO).
Results:
A total of 1,546 articles were evaluated, and we identified 20 for further analysis. On the basis of the current peri-operative antibiotic prophylaxis recommendations for cardiac surgery and the papers reviewed, we tried to propose a schedule for peri-operative antibiotic prophylaxis in pediatric cardiac surgery.
Conclusions:
There is a need for careful use and examination of the schedule proposed because the pharmacokinetics of antibiotics in pediatric patients with ECC is not fully understood. This should be evaluated further. Formulating uniform recommendations concerning peri-operative antibiotic prophylaxis is difficult.
The infection rate in children after cardiac surgery with extracorporeal circulation (ECC) remains unknown, but such infections often are fatal. The surgical site infection (SSI) rate in pediatric cardiac surgery, which usually is considered “clean,” should be close to zero, but it is 1%–9%; and the post-operative nosocomial infection rate reaches 23% [1–4]. In the National Registry of Cardiac Surgery Procedures (KROK), the SSI rate in Poland is reported to be 1% [5]. Prophylactic antibiotic therapy is given routinely in the peri-operative period to prevent such infections. However, an optimal schedule has not been defined. Heterogeneity of antibiotic prophylaxis schedules at pediatric cardiac surgery centers is a fact, and the schedule often is determined on a historical, institutional, or personal basis [3]. Local recommendations follow the guidelines for adults, which might be improper because of the inherent challenges in pediatric research and the heterogeneity of the population [6]. In this review, we analyze current knowledge, supported by up-to-date publications, about antibiotic prophylaxis in pediatric cardiac surgery.
Materials and Methods
The PubMed® database was searched for the following keywords: Pediatric cardiac surgery; Children cardiac surgery; Antibiotic prophylaxis; and Perioperative prophylaxis. The keywords were combined with the “AND” Boolean operator. Only full-text journal articles describing peri-operative antibiotic prophylaxis in detail and in the English language were analyzed. The references of the articles were screened and, if proper, included in the study. The inclusion criteria were original papers or reviews concerning peri-operative antibiotic prophylaxis in children undergoing heart surgery with the use of ECC published since 2000 and including at least one of the following pieces of information: Antibiotic name, dosage, and time of either the first dose or prophylaxis completion post-operatively. The exclusion criteria were: Type of publication other than original paper or review, paper in language other than English, and schemes concerning only adult patients.
In publications included in this review, we analyzed peri-operative antibiotic prophylaxis in children undergoing cardiac surgery with the use of ECC. Because of the many clinical situations, we analyzed mainly antibiotics used for standard prophylaxis with dosing schema, time of the first dose, additional dosage at ECC priming, and prophylaxis duration. Additionally, we looked for special clinical situations such as prophylaxis in children with the sternum left open after surgery, β-lactam allergy, or pre-operative methicillin-resistant Staphylococcus aureus (MRSA) colonization and patients requiring extracorporeal membrane oxygenation (ECMO).
We report this review in accordance with the PRISMA statement [7]. Because this is a review study, we did not require the approval of an ethics committee.
Results
A total of 1,546 articles were evaluated, and 86 articles were identified for further review (Fig. 1). After a careful search for references, we identified an additional 8 of 48 papers relevant for the analysis. After the removal of duplicates, exclusion of reports other than original papers or reviews, and reports that did not fulfill the inclusion criteria, we identified 20 publications for the final analysis [1–3, 8–24]. Detailed information included in these 20 papers is provided in Table 1.
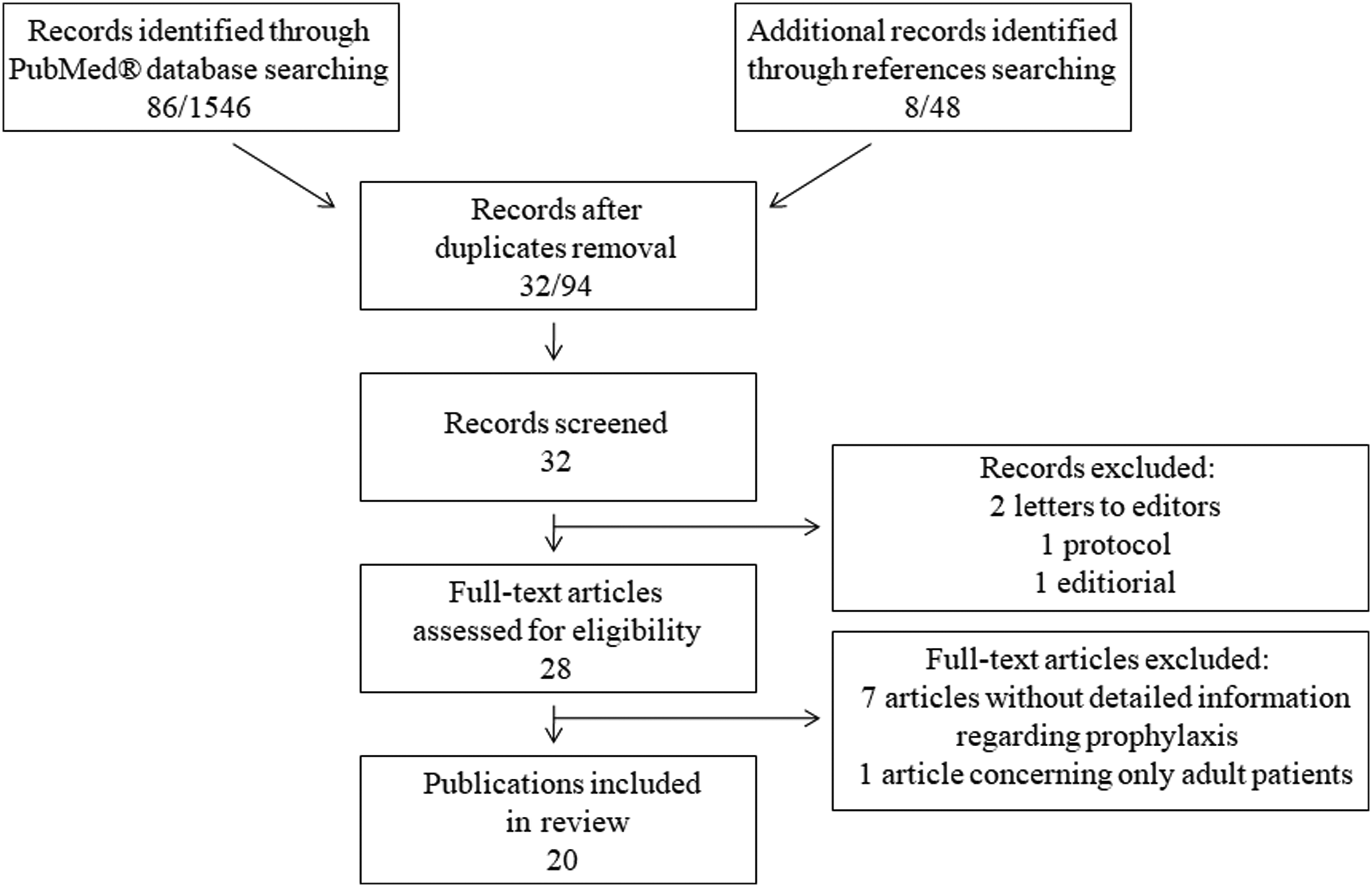
Flow of publications search through different phases of a systematic review for antibiotic prophylaxis in pediatric cardiac surgery in accordance with the PRISMA statement [7].
Summary of Chosen Papers on Antibiotic Prophylaxis in Children Undergoing Cardiac Surgery a
All antibiotic doses are intravenous.
ECC = extracorporeal circulation; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; MRSA = methicillin-resistant Staphylococcus aureus; VAD = ventricular assist device.
In 13 of the 20 studies (65%), the main antibiotic given for peri-operative prophylaxis was a first-generation cephalosporin, which was cefazolin in 12 papers. Each dose of this drug ranged from 20 mg/kg (one study) to 50 mg/kg (one study) and was mostly 25 or 30 mg/kg (nine studies). In two studies (10%), the main antibiotic used for prophylaxis was a second-generation cephalosporin, and in one study (5%), either a first- or a second-generation cephalosporin was given. In another study, the authors write about cephalosporins but do not specify the generation of the drug given (5%), and three studies (15%) do not specify in any way what kind of antibiotic was used. In 14 studies, prophylaxis with one antibiotic was described, and two studies reviewed combined prophylaxis of a first-generation cephalosporin and an aminoglycoside (gentamicin). One study concerned the use of penicillin with β-lactamase inhibitors as an alternative to any cephalosporin prophylaxis, and a final study discussed vancomycin use.
The time of the first dose was described in 15 studies: In 14, it was within 60 minutes before skin incision, and one study described the first dose being administered at the induction of anesthesia. In five studies (25%), there was no information on the timing. An additional antibiotic dose at ECC priming was described in five studies: three of them discussed an additional dose being given at ECC initiation (dosage the same as the first dose), one report dealt with an additional dose of cefazolin 25 mg/kg and one of 30 mg/100 mL given at ECC priming. Additional information about intra-operative redosing was found in nine reports: Six groups of authors reported intra-operative redosing every three to four hours, one author reported an additional dose at the start of rewarming, one an additional dose after separation from ECC, and one if ECC lasted more than two hours or the overall operation time exceeded 6 hours.
After an operation, cefazolin was administered every six hours (two studies) or every eight hours (five studies) or in only two doses, except in neonatal infants (younger than 7 days), in whom the reported redosing was every 12 hours (two studies). If cefuroxime was given, then post-operative redosing was every eight hours (one study), and gentamicin was administered every 12 hours (one study).
The post-operative prophylaxis duration was reported in 15 studies (75%) and was 24 hours after surgery (three studies) or for 48 hours (10 studies). In one study, administration was continued until all chest tubes had been removed and in one study at 48 hours after the removal of the tubes.
The antibiotic prophylaxis in children with delayed sternal closure was described in eight of the reports. In these children, the reported standard antibiotic prophylaxis was continued for 24 hours (one study), 48 hours (one study), or until the removal of all chest tubes after sternal closure (one study). In five studies, there was a change from standard antibiotic prophylaxis to another schedule if the sternum was left open post-operatively. In one study, a post-operative change to vancomycin was described, and four reports included the use of two antibiotics: cefazolin + aztreonam (one study), cefazolin + vancomycin (one study), and vancomycin + gentamicin (two studies).
Information about peri-operative antibiotic prophylaxis in children with β-lactam allergy was described in six reports: Vancomycin, clindamycin, and clindamycin + gentamicin was used in four, one, and one study, respectively. In patients with known nasal MRSA colonization in two studies, intranasal mupirocin was prescribed, and antibiotic prophylaxis with vancomycin (four reports) or teicoplanin (one report) was given. In one study, intranasal mupirocin was administered to all children regardless of their MRSA status. Antibiotic prophylaxis in children on ECMO was described in only two studies. The standard prophylaxis with cefazolin was reported in one of them and with vancomycin in the other.
Discussion
Prophylactic antibiotic therapy is given routinely in the peri-operative period in pediatric cardiac surgery to decrease the risk of SSI; however, a specific optimal schedule has not been defined. Difficulties related to the design and performance of studies with randomization in children are known. Hundreds of decisions made every day in the management of pediatric patients in different centers can influence children's colonization, surgical site protection, and post-operative management [6]. Nevertheless, in view of the European Union Guidelines for the Prudent Use of Antimicrobials in Human Health, the general recommendation is to reduce inappropriate use and promote the prudent use of antimicrobial drugs [25]. The exposure of micro-organisms to antimicrobial agents creates a selective pressure that can lead to resistance, and the inappropriate use of antimicrobial agents accelerates the emergence and dissemination of resistance.
To the best of our knowledge, currently, there have been no randomized trials concerning peri-operative antibiotic prophylaxis in children undergoing cardiac surgery. In well-known clinical practice guidelines for antimicrobial prophylaxis in surgery presented by Bratzler et al. in 2013, it is stated that in most cases, all recommendations for the pediatric population except for dose are the same as for adult patients [26]. Surgical techniques and post-operative management, bacterial resistance patterns, and antibiotic usage have changed in recent years, and therefore, we tried to summarize current schedules. Our review includes manuscripts published after the year 2000. What is interesting is that although some medical centers designed and implemented proper procedures, restricted observance of them could be problematic. Murray et al. point to the fact that after a strict schedule implementation, timing of antibiotic prophylaxis was not proper in about 20% of patients, 27% of patients did not receive appropriate intra-operative redosing, and 84% had inadequate post-operative doses [17]. Surprisingly, after the implementation of an antibiotic prophylaxis protocol in this special group of patients, some authors observe that additional antibiotics for empirical treatment are initiated more often after the intervention than before (26.9% vs. 18.6%, respectively) [12]. It is to be hoped that this is a transient phenomenon, as implementation of proper tools for diagnosing infections with accurate interpretation is essential.
Cardiopulmonary bypass impairs humoral immunologic defenses and causes systemic inflammatory response syndrome with degradation of clotting factors. Patients with congenital heart disease who are operated on with ECC may be at even higher risk of SSI development than adult patients. In children, there are many additional factors that can increase this risk. The immature renal function and altered circulatory pathways can alter the absorption, distribution, metabolism, and elimination of antibiotics [3]. The immature immunologic system of children, use of deep hypothermic circulatory arrest, long operation time, delayed sternal closure, complex reconstructions, ECMO, longer duration of chest tube drainage (e.g., Fontan patients), and delayed return to normal feeding are other potential risk factors for SSI development [3]. There are studies involving adults and children undergoing ECC that show significant decreases in the concentrations of vancomycin, cephalosporins, and gentamicin at the onset of ECC [3]. In contrast to adult patients, in children, ECC priming volume causes significant hemodilution. The increased distribution volume after ECC start should be taken into consideration because it can decrease antibiotic serum concentrations. Therefore, adding antibiotics to the priming fluid seems reasonable.
Standard peri-operative antibiotic prophylaxis should be the first line to prevent SSI. The predominant micro-organisms causing SSI in children are staphylococci [1,26]. That is why the reasonable option for the peri-operative antibiotic prophylaxis that covers these micro-organisms is a first- or second-generation cephalosporin. In the papers reviewed, these antibiotics were often recommended, as in the adult population. Nevertheless, it has been confirmed that adult guidelines are safe to use also in neonatal infants [17]. In such infants, Alvares et al. recommend ampicillin with an aminoglycoside as an alternative to cephalosporins [1]. Some authors add an aminoglycoside to a cephalosporin; however, there is no evidence of a higher rate of infection with gram-negative bacteria after pediatric cardiac surgery, even in patients with delayed sternal closure [3]. That is why the addition of gentamicin may be questionable. The routine use of vancomycin, even though it was not reported in our review, should be abandoned except in certain cases because of its additional problems [26]. For example, it is well known that vancomycin can cause nonimmunologic release of histamine. Clinically, this can be manifested as hypotension, red-man syndrome (flushing), bronchospasm, and even cardiac arrest [3,27,28]. Another important problem is the emergence of vancomycin-resistant bacteria as for example Staphylococcus aureus (VISA) and Enterococcus spp. (VRE) [3]. It also should be mentioned that, in the scope of preventing SSIs induced by methicillin-susceptible S. aureus (MSSA), vancomycin is less effective than cephalosporins, and therefore, given its pharmacokinetics, vancomycin might be used in combination with cefazolin if needed.
In patients receiving therapeutic antimicrobial drugs in relation to a remote infection, antimicrobial prophylaxis should be given before surgery also to ensure an adequate concentration of the drug in the serum and tissues [26]. If prescribed agents are appropriate for surgical prophylaxis (i.e., they cover the appropriate antimicrobial spectrum), administration of an extra dose within 60 minutes before the surgical incision should be sufficient. Otherwise, standard antimicrobial prophylaxis should be added to the therapy [26]. Peri-operative antibiotic prophylaxis in children with β-lactam allergy differs from the routine schedule. The use of vancomycin in these patients is recommended in most of the papers in our review, although clindamycin may be an option [26]. Both antibiotics can be supported by addition of an aminoglycoside.
Effective prophylaxis depends on an adequate serum antibiotic concentration at the time of the skin incision, as well as during and shortly after the operation. Proper timing of antibiotic administration therefore is essential. All reports we reviewed said that the first dose of cephalosporins should be given within 60 minutes before the skin incision. There also is a need to ensure adequate drug concentrations in the serum and tissue if the surgery time exceeds the half-lives of the drug or there is excessive blood loss during the procedure [26]. In pediatric cardiac surgery, the risk of SSI increases with surgery duration [10,11]. A study by De Cock et al. based on pharmacokinetics suggests that an optimal protocol for children undergoing cardiac surgery may be as follows: Cefazolin 40 mg/kg within 30 minutes before the surgical incision, 20 mg/kg at start of ECC, 20 mg/kg at the start of rewarming on ECC, and 40 mg/kg eight hours after the third and fourth dose [20]. In children, a dose of cefazolin of 25 mg/kg before the incision and 25 mg/kg to the ECC priming volume may not achieve the proper serum concentration and therefore may not be effective for full prophylaxis in infants [16]. Nevertheless, intra-operative redosing every three to four hours is recommended by most of the publications reviewed.
Another issue discussed is the duration of post-operative antibiotic prophylaxis. As stated by Alphonso et al., many cardiac surgeons consider, either correctly or not, that their patients are at particularly high risk for SSI. Some of them therefore prolong antibiotic prophylaxis until all chest tubes or even central intravenous lines have been removed [3]. Maher et al. compared three protocols in children with congenital heart defects and concluded that giving antibiotic prophylaxis for as long as thoracic tubes are in place may reduce the SSI rate [8]. However, other authors report many weaknesses in this study [3]. Nowadays, there is no scientific evidence from properly designed studies suggesting that continuing the administration of antibiotics until the chest tubes are removed enhances protection against infections, and prolongation of antibiotic prophylaxis raises concerns about encouragement of multi-drug resistant organisms, superinfections, and drug toxicity [26]. Therefore, the duration of antibiotic prophylaxis should not be dependent on drains, lines, or catheters. In 2007, Alphonso et al. described a worldwide survey of antibiotic prophylaxis in pediatric cardiac surgery facilities of at least 50 units, with response by 42 units [3]. Of these, 36% used post-operative antibiotic prophylaxis for the maximum period of 24 hours, 24% for as long as 48 hours, 9% for as long as 72 hours and 31% for more than 72 hours or until the removal of central lines and chest tubes. In our review, most of the centers discontinue antibiotic prophylaxis before 24–48 hours. Many authors conclude that suspension of antimicrobial prophylaxis during the first 48 hours after surgery did not increase the rate of nosocomial infections [1,19]. It should be mentioned that there are studies showing that the incidence of infections was significantly higher in patients in whom prophylaxis was maintained post-operatively for more than 48 hours than in the others (16.2% vs. 6.7%; p < 0.05) [1].
In patients with delayed sternal closure after the primary operation, the authors of the selected studies recommend the continuation of standard prophylaxis or varied combinations of antibiotic schedules until 24–48 hours after sternal closure. Nevertheless, there are no scientific reasons to change primary antibiotic schedules [26]. This issue requires further detailed evaluation. There are few studies concerning antibiotic prophylaxis post-operatively in relation to ECMO or ventricular assist devices (VAD). It is worth mentioning that none of papers reviewed describe antibiotic prophylaxis in children requiring VAD. However, there is no evidence to change the standard peri-operative antibiotic therapy approach taking MRSA colonization or delayed sternal closure into account [26].
In pediatric populations, MRSA is rarely considered as a risk factor for SSI. However, patients at high risk for this infection are those with pre-operative MRSA colonization or with a history of MRSA infection as well as neonatal infants and children with complex congenital heart disease [26]. For these patients, a glycopeptide is recommended for peri-operative prophylaxis. Adding cefazolin to vancomycin may be in order to increase the antimicrobial power, especially if gram-negative infections occur locally [26]. Nasal mupirocin decontamination can lower the risk of post-operative infections, although there are limited data supporting its use peri-operatively [2,26]. Current recommendations support the application of intranasal mupirocin for all patients with documented S. aureus colonization, not only with MRSA strains [26]. Conducting studies on this issue in pediatric populations should be considered.
Another issue concerning peri-operative antibiotic prophylaxis not reported in the studies reviewed is the intra-operative use of implanted gentamicin collagen sponges. Kowalewski et al. concluded in their meta-analysis that implantable gentamicin collagen sponges significantly reduce the risk of sternal wound infection after cardiac surgery in adults [29]. However, two well-designed randomized trials failed to show any efficacy in adult patients [30,31]. There are still limited data supporting its use in children undergoing surgery with the use of ECC, and given that safety and efficacy are not clearly established, this technique cannot be recommended for routine use [26].
Based on current peri-operative antibiotic prophylaxis recommendations for cardiac surgery and on the papers reviewed, we tried to achieve compromise in the proposed schedule [26]. The presence of β-lactam allergy or S. aureus colonization (with resistance pattern) should be known pre-operatively. In children with S. aureus colonization, intranasal mupirocin should be prescribed for a minimum of three days pre-operatively. Standard antibiotic prophylaxis consists of cefazolin 30 mg/kg given 5–60 minutes before the skin incision with an additional dose as part of ECC priming. Intra-operative redosing every three to four hours and post-operative continuation every six hours until 48 hours post-operatively should be followed. In patients with β-lactam allergy, clindamycin or vancomycin with gentamicin is proposed. In MRSA-colonized patients, vancomycin with cefazolin is recommended. In patients with delayed sternal closure after operation, antibiotics should be administered for another 24 hours after the closure, while in patients on ECMO or VAD, standard antibiotic prophylaxis should be used with discontinuation for 48 hours after the operation (except in patients with delayed sternal closure). Detailed information is presented in Table 2.
Suggested Schedule for Peri-Operative Antibiotic Prophylaxis in Children Undergoing Cardiac Surgery
ECMO = extracorporeal membrane oxygenation; ECC = extracorporeal circulation; MRSA = methicillin-resistant Staphylococcus aureus; VAD - ventricular assist device.
Conclusions
Children with congenital heart disease undergoing surgery with the use of ECC constitute a special group of patients in whom many factors concerning proper peri-operative antibiotic therapy should be taken into account. The implementation of an effective prophylaxis protocol for children undergoing cardiac surgery is needed, especially in view of worldwide antibiotic overuse and increasing development of resistance. Strict control of patients' clinical status especially in terms of infection while implementing all peri-operative antibiotic prophylaxis schedules is essential. There is a need for the careful use and for examination of the schedule proposed because the pharmacokinetics of antibiotics in pediatric patients with ECC is not fully known, and this should be evaluated further. Formulating uniform recommendations concerning peri-operative antibiotic prophylaxis is difficult. Studies are needed with randomization estimating safety and efficacy of particular schedules of antibiotic prophylaxis in children.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest related to this manuscript.