
Abstract
Abstract
Background:
Abdominal infections following surgery have many severe consequences. Several effective, well-evaluated infection prevention and control processes exist to avoid these infections.
Methods:
This manuscript reviews and provides supporting evidence for common management strategies useful to avoid postoperative abdominal infection.
Results:
Prevention of abdominal infection begins with preparation of the environment using standard infection control practices. Peri-operative use of systemic antibiotics, an antibiotic bowel preparation in colorectal surgery, and effective antiseptic preparation of the surgical site all reduce infection rates. Peri-operative supplemental oxygenation, maintenance of core body temperature, and physiologic euglycemia will reduce both incisional and organ-space infections in the abdominal surgery patient. Strategic use of irrigation and drain placement may be useful in some circumstances.
Conclusion:
Specific methods of prevention are documented to reduce intra-abdominal infections. Prevention requires a multi-disciplinary team including the surgeon, anesthesiologist, and all operating room personnel.
A
Preparing the Environment for Surgery
Operating room preparation
The operating room is an environment that can be optimized to prevent infection. Cleaning protocols focusing on surfaces in contact with patients and providers need to be established and executed (Fig. 1). The best approach is to move from least contaminated to most contaminated areas and to first wash and then disinfect appropriate surfaces [3]. Microbicidal solutions such as glutaraldehyde, peracetic acid, and hydrogen peroxide provide high-level disinfection and are used to neutralize vegetative bacteria, mycobacteria, viruses, fungi, and most spores; these compounds are highly toxic. Intermediate-level disinfection can be obtained using chlorine-containing compounds (e.g., sodium hypochlorite) and alcohols, as well as certain types of iodophors and phenolics.
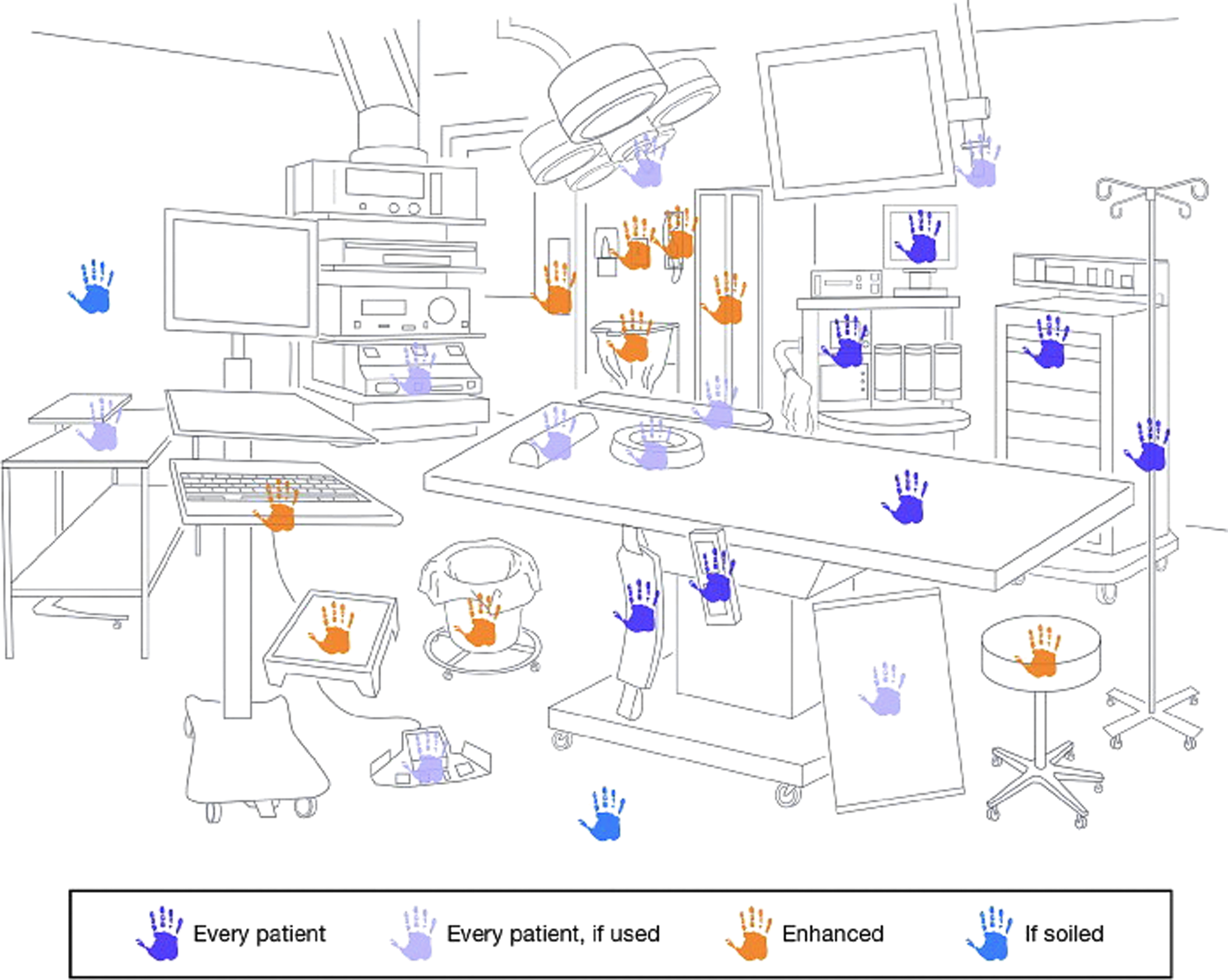
Recommended cleaning frequency for operating room surfaces. (Reprinted with permission from Spruce L, Wood A. Back to basics: Environmental cleaning. AORN J 2014;100:55–61.)
Ideally, contaminated cases should be separated from clean cases, either physically or temporally (with contaminated cases being completed at the end of the workday to allow overnight cleaning). That said, plenty of field hospitals have been set up in less than ideal settings without a clear detriment to patients who underwent operations as a result of the environment itself [4]. The use of laminar airflow for the prevention of surgical infections has not been recommended by the World Health Organization (WHO) in their recent guidelines for preventing surgical site infections (SSIs). There has not, to our knowledge, been any definitive study of the operating room environment and what specific measures need to be undertaken to ensure maximum environmental sterility for infection control; however, specific outbreaks have prompted the hunt for causative contaminants and implicated environmental sources in the past.
Surgical instrument sterilization
Sterility is an important step to ensure instruments used in surgery do not act as vectors between patients or as fomites introducing pathogens into the surgical incision. In many parts of the world, instrument cleaning and sterilization is neither standardized nor appropriately protocoled [5]. There are no universal guidelines for instrument decontamination; however, both WHO and Jhpiego have produced comprehensive documents on medical device and instrument reprocessing and decontamination, [6,7], and a number of national organizations such as the National Health Service have clear guidance for the cleaning and sterilization of reusable surgical instruments [8]. Many guidelines that exist locally in poorer parts of the world are based on inaccurate or outdated information [5].
Instruments should be cleaned and sterilized as part of an instrument processing cycle (Fig. 2). Pre-cleaning is typically accomplished at the point of use by removing visible gross debris and proteinaceous material from the surface of the instrument. This is followed by a more thorough cleaning process in a designated “dirty” area where instruments undergo multiple cleaning steps using an enzymatic detergent solution (not bleach, as this is corrosive to instruments) that denature proteins. The ideal solution should have high germicidal activity against a wide range of micro-organisms (including spores), be chemically stable, compatible with the material being disinfected, and ideally inexpensive and able to penetrate groves and joint surfaces. The instruments are then moved to a clean area to undergo inspection for rust, retained debris, and malfunction (Fig. 3) before being packaged using a protective cloth or metal barrier. Finally, terminal sterilization is required, usually in a steam autoclave that reaches a threshold temperature and pressure for a specified amount of time. Sterile indicators, both external to, and within, the sterilized trays help ensure quality control by verifying sterility.
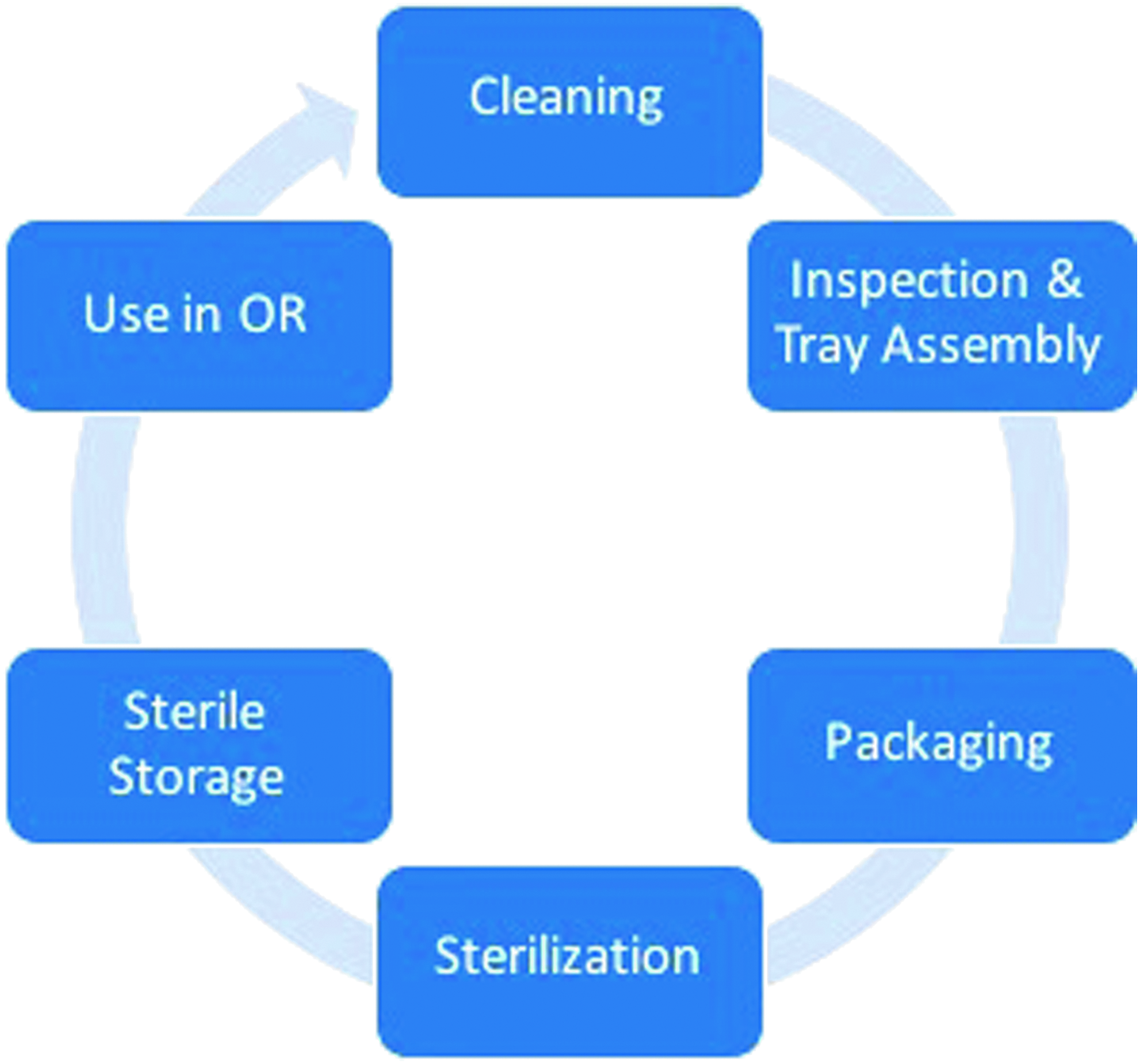
Cycle of decontamination of reusable surgical instruments.
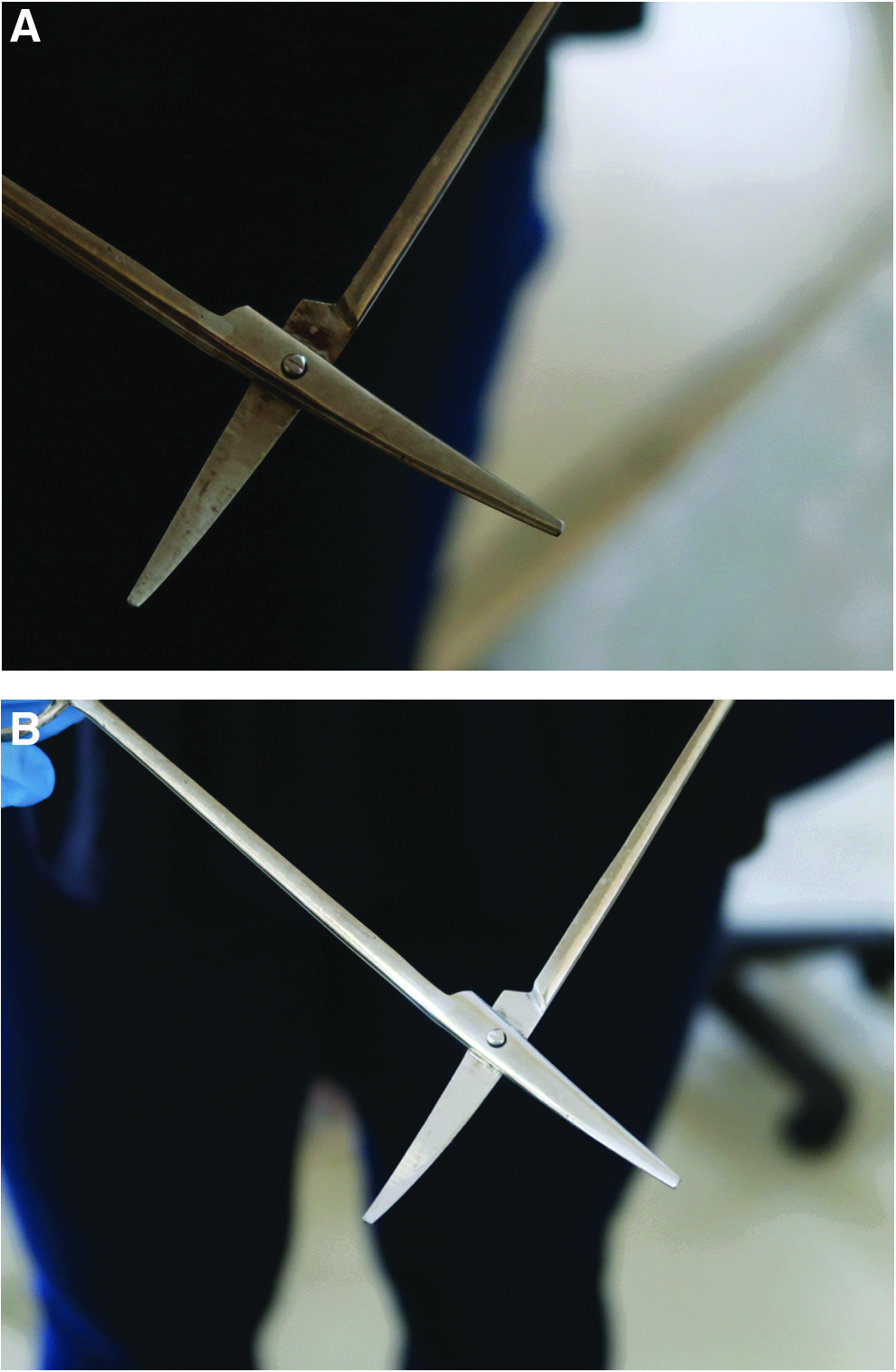
Instruments after appropriate cleaning, stain removal, and polishing. (Image copyright by and courtesy of SPECTrust.)
Surgical team preparation
Maintenance of the sterile field through the establishment of a sterile barrier with drapes, gowns, and gloves is a central tenant of surgery. Full barrier precautions are indeed recommended for any sterile procedure, such as the placement of central lines, chest tubes, and epidural catheters. As noted in a classic study of the central line bundle, full barrier precautions are one of the key standards for preventing infection during line insertion [9] even though there was no specific assessment of the proportional contribution of this standard to the global reduction in central line infections. Past studies have evaluated specific types of gowns and drapes [10] (woven versus non-woven and impregnated drapes, for example), but a comprehensive assessment of the contribution of gloves, gowns, and drapes to preventing incision infection is unlikely to be undertaken; historic assessments have informed their use and the materials that are currently recommended for gowns and drapes (either nonwoven disposable or woven reusable non-cotton material) [11,12].
Preparing the Patient for Surgery
Modifiable patient risk factors
Although the specifics of patient risk factor control are beyond the scope of this review, factors contributing to a higher risk of infection such as obesity, smoking, diabetes mellitus, immunosuppression, malnutrition, and concomitant infections are ideally addressed and optimized in the pre-operative period to the extent possible.
Hair management
The use of clippers rather than shaving, or simply avoiding hair removal altogether, is now standard of care and well supported by the literature [13]. From a practical perspective, many surgeons routinely remove hair for perceived hygienic or cosmetic reasons or to facilitate the application and removal of dressings. Regardless, shaving should be abandoned.
Bowel preparation for colorectal surgery
For patients undergoing colorectal surgery, bowel preparation has gone through its share of permutations in practice [14,15]. The latest evidence demonstrates conclusively that a mechanical bowel preparation coupled with oral antibiotics is the appropriate manner to decontaminate the large bowel prior to surgery [16–18]. The mechanism is straightforward: clear most feculent material, reduce bacterial load in the lumen, and neutralize the remaining flora with a locally active antimicrobial drug. This typically is accomplished through the institution of a low-residue diet 48 hours prior to surgery, followed by the use of a cathartic drug such as magnesium citrate in series starting the afternoon before surgery to evacuate the bowels, coupled with an oral antibiotic the evening before surgery (Table 1). Published studies have focused on surgery of the colon for this issue because of the high bacterial load; the effect of preparation on the small bowel has not been as extensively evaluated.
Options for Mechanical Bowel Preparation and Oral Antibiotics Prior to Abdominal Operations
PEG = polyethylene glycol.
Patient decontamination
Skin decontamination has been studied extensively, although mostly in terms of superficial and deep incisional infections as opposed to organ space or intra-abdominal infections. There is a demonstrable benefit to pre-operative bathing, and even using something as simple as plain soap prior to surgery (the night before or the morning of) is beneficial. Medicated soap, such as chlorhexidine, is common in places where it is available, and likely has some additional antiseptic benefits, but whether those are truly additionally beneficial over soap when appropriate skin antisepsis is undertaken prior to incision has yet to be determined. An additional consideration is the systematic decontamination of Staphylococcus aureus carriers with mupirocin ointment to the nares [19,20]. This protocol requires the routine screening of appropriate patients undergoing surgery (in particular, those undergoing cardiac or orthopaedic procedures, where its value has been well documented, but presumably in all surgical patients as a means of preventing auto-infection), followed by twice-daily application of mupirocin ointment to the nares for five days. Thus, a strict pre-operative protocol must be instituted and followed in advance of surgery for this measure to be effective.
Perioperative Care
Pre-incisional antibiotics
For minimizing risks for intra-abdominal infection, actions taken during the immediate peri-operative and intra-operative periods may have the most significant benefits. A top priority is administering the appropriate antibiotic at the appropriate dose at the most opportune time for preventing infection—that is, at a point when the peak tissue concentration is achieved immediately prior to incision [21]. For many common prophylactic antibiotics (vancomycin being the main exception), this time typically occurs about 30 minutes after administration. In practice, this usually translates to the administration of antibiotic prophylaxis in the operating room at the time of anesthetic induction, as this roughly equates to the appropriate time to reach a therapeutic blood concentration before the skin is incised. The WHO, U.S. Centers for Disease Control and Prevention (CDC), and other expert groups have provided strong recommendations on this practice, with the specific recommendation that administration occurs no more than 120 minutes prior to incision [12,22]. The purpose of this is to establish a tissue environment that is poorly conducive to bacterial contamination should it occur. The classic study by Classen et al. established this practice, which has been dictum ever since [23].
Although the issue of post-operative use of antibiotics continues to be debated, best evidence indicates that antibiotics used for prophylaxis to prevent infections should be discontinued within 24 hours after surgery and ideally immediately after surgery [24,25]; this is true regardless of the presence of drains or implants. This recommendation has frequently been ignored across a range of operations [26,27] despite its considerable adverse risks [28]. Much work remains to be done to convince clinicians of the wisdom of appropriately stopping antibiotics after surgery [29].
Skin antiseptics (skin preparations)
The choice of skin antiseptic preparation has differed over the years, but the current recommendations include an alcohol-based scrubbing solution coupled with chlorhexidine for all appropriate surgical sites; examples of sites that are best decontaminated with povidone–iodine alone are mucosal surfaces such as the vagina, mouth, and anus. Prior studies comparing chlorhexidine with iodine reduced the risk of incision infections by 40% compared with povidone–iodine skin scrub alone but lacked the alcohol base in the iodine solution [30]. However a recent randomized controlled trial demonstrated a benefit of chlorhexidine and alcohol over iodine and alcohol in caesarean delivery, with a 45% reduction in SSI driven mostly by reductions in deep wound infections [31]. Given the strong evidence of the benefits of chlorhexidine, and its mechanism of action and safety profile [33], its use can be recommended as the skin antiseptic of choice.
Normothermia
Normothermia is important, as hypothermic patients are at greater risk of post-operative infections. This effect has been well studied in colorectal surgery, but there is a presumption that such effects hold true for other operations as well. Maintaining normothermia is the job of the entire operating room team, as interventions such as room warming, fluid warming, and active patient warming through the use of hot air devices and body cavity lavage with warmed (38°C) fluids helps maintain normal body temperature during surgery.
Avoidance of hypoxia
High fractional inspiration of oxygen (FiO2) is recommended for patients undergoing general anesthesia when there is no risk to the airway of a combustion event. High FiO2 (>0.8) maximizes the tissue oxygen concentration, making the element available for the development of free radicals and the destruction of micro-organisms through the normal inflammatory pathway. A high FiO2 probably should be continued in the post-operative recovery period to provide maximum tissue concentrations of oxygen after the initial surgical insult [22]. This recommendation has come under scrutiny recently, as there are potential negative clinical implications of high FiO2, such as absorption atelectasis and other pulmonary and cardiac complications. Studies are under way to assess the effects of a high FiO2 in a broad population of surgical patients and should lend insight into this question.
Normoglycemia
Normoglycemia is an important factor for reducing surgical infections, and routine peri-operative and intra-operative control of blood glucose is standard practice. Typically, the goal is a glucose concentration <180 mg/dL while guarding against hypoglycemia. Diabetic patients require especially close glucose monitoring, as patients with intra-operative hyperglycemia are at higher risk of an elevated glucose concentration in the immediate post-operative period.
Mitigating the Effects of Established Contamination or Soilage
Irrigation
When contamination does occur, the appropriate lavage of both the body cavity and the operative site can help reduce infection risk. The adage “dilution is the solution to pollution” seems appropriate, and removal of gross contamination through high-volume irrigation is both aesthetic and beneficial. Intra-peritoneal lavage should be accomplished using warm isotonic solution, as this maintains normothermia and does not disrupt immune cells already present in the abdomen that are potent signalers of infection and are required for an inflammatory response. Once the peritoneum and fascia are closed, an irrigant of dilute povidone–iodine may be used and indeed is preferable to an antibiotic solution for washing the subcutaneous tissue after contamination, as it has rapid toxic effects on bacteria present in the incision and does not promote antimicrobial resistance [22].
Ensuring adequate perfusion
Goal-directed fluid therapy during surgery has become standard practice for anesthesiologists. Historically, fluid was administered according to the time on the table. Now fluid is delivered with specific goals in mind: Optimum heart rate and blood pressure and acceptable urine output. This is accomplished using invasive and non-invasive monitoring such as measurement of arterial, central venous, and pulmonary artery pressure when such devices are in place and data are available, and dynamic changes and pulse pressure variations during the respiratory cycle. Ensuring optimum intravenous volume ensures appropriate tissue perfusion while avoiding edema and fluid sequestration that can, in the days after surgery, collect at the surgical site and in the lungs and potentially contribute to poor incision healing, slower recovery, and a greater risk of infection.
It nearly goes without saying that meticulous and gentle tissue handling, removal of dead tissue, the minimization of trauma to surrounding tissues and structures, and the closing of dead space are all tenants of surgical technique. In as much as possible, injury to tissue should be avoided, blood and debris removed, and spaces closed to prevent the accumulation of fluid and the creation of an environment conducive to bacterial propagation, the goal being adequate perfusion throughout the surgical field.
Drains
The value of drains in preventing intra-abdominal infection has never been supported. Multiple systematic reviews, inclusive of randomized controlled trials, demonstrate no patient outcome improvement (SSI rate, hospital length of stay, leak or other morbidity) attributable to the prophylactic use of drains after most gastrointestinal operations [34], regardless of contamination. This includes appendectomy for acute appendicitis [35,36], cholecystectomy for acute cholecystitis [37], small bowel resection for spontaneous perforation from typhoid infection [38], or after colonic anastomosis [39–42]. For routine spillage of pus or gastrointestinal contents, local suction and irrigation of the area without placement of drainage catheters is appropriate. Drain placement should be considered carefully and only for those patients for whom a leak could result in high morbidity or death (i.e., those having pancreatic resection). Additionally, there are no data to support the use of antibiotics to prevent infection solely because a drainage catheter is in place.
Conclusions
The combination of many of these mechanisms, strategies, and maneuvers likely has a synchronous effect in reducing infections [43]. Several bundled strategies have been proposed with promising results, including by the Hospital Corporation of America, the Michigan collaborative, and the Cleveland Clinic [44–46]. This result is in keeping with the profound effects bundled care packages have had on clinical outcomes through compliance with a suite of best practices [47]. Importantly, these strategies cannot be instituted without a strong commitment from several disciplines, for example, the surgeons, the anesthesiologist, the nurses, the ward staff, the cleaners, and the central sterilizing unit. The partnership between the surgeon, the anesthesiologist, and the nurses involved in care is particularly powerful and must be promoted and maintained for the betterment of our patients and our profession.
Footnotes
Acknowledgment
We thank Christina Fast from SPECTrust for assistance reviewing parts of this manuscript.
We declare no conflicts of interest related to this work.
Author Disclosure Statement
No competing financial interests exist.