
Abstract
Background:
Osteomyelitis of the diabetic foot is a costly health problem worldwide. Early and accurate diagnosis of the disease in patients with diabetic foot infections is needed urgently and will have an important role in diabetic foot management.
Methods:
This was a case-control study of subjects with diabetic foot ulcers admitted to Beijing Shijitan Hospital from September 2015 to April 2018. We compared differences in the atherogenic index of plasma (AIP) in patients with or without osteomyelitis.
Results:
The mean AIP of 165 patients with osteomyelitis was 0.23 ± 0.24, which was significantly higher than the mean AIP of patients without osteomyelitis. Higher AIP values were associated with a considerably higher risk of osteomyelitis with an odds ratio of 1.81 (95% confidence interval [CI] 0.71–4.61), 4.70 (1.88–11.75), 5.03 (2.06–12.25) and 1.74 (1.33–2.28). Moreover, at a cut-off of 0.184, the AIP value showed a sensitivity of 84.3% and a specificity of 83.1% in the discriminatory identification of diabetic foot osteomyelitis.
Conclusions:
Elevated AIP was significantly associated with diabetic foot osteomyelitis, supporting the use of this index as a biomarker for the diagnosis in clinical practice.
Diabetic foot ulcers (DFUs) and the often-resulting lower-extremity amputations are a common, complex, and costly complication of diabetes. The prevalence of foot ulcers among patients with diabetes is estimated to be 15% [1], and the lifetime incidence of DFUs may be as high as 25% [2]. Diabetic foot osteomyelitis (DFO) is a serious complication of DFU or diabetic foot infections. The presence of osteomyelitis delays wound healing, increases the likelihood of surgical intervention, and extends the duration of treatment with antibiotics [3,4]. Therefore, early and accurate diagnosis of osteomyelitis in patients with diabetic foot infections has an important role in diabetes management.
Diagnosing osteomyelitis in a patient with diabetic foot lesions often is difficult. Although bone biopsy is currently the gold standard, this technique is not widely used because of its invasiveness and the high skill level required for sample procurement [5]. Moreover, bone biopsy sometimes leads to false-negative or false-positive results because of variables such as culturing technique and site of sampling [5]. The clinical probe-to-bone test and magnetic resonance imaging examinations also are widely applied in the diagnosis of diabetic foot osteomyelitis [6,7], although the accuracy of these two methods remains controversial. Importantly, a false-positive osteomyelitis diagnosis may lead to prolonged use of antibiotics or unnecessary surgery, including amputation. False-negative diagnosis can result in wound healing complications, progression of the infection, and systemic sepsis [8]. Thus, an unmet need exists for new methods to diagnose osteomyelitis accurately in patients with diabetic foot infections.
The use of plasma and serum biomarkers for the prediction and diagnosis of disease can be a noninvasive and widely available resource for clinical management. Atherogenic index of plasma (AIP), the logarithmic ratio of triglyceride (TG) to high-density lipoprotein–cholesterol (HDL-C) concentration [9], is an indicator of atherosclerosis and related diseases such as cardiovascular dysfunction and peripheral artery disease (PAD) [10–13]. Defined as atherosclerotic occlusive disease of the lower extremities, PAD is associated with an increased risk of lower extremity amputation and serves as a biomarker for atherothrombosis in the cardiovascular beds [14]. Additionally, PAD can cause significant long-term disability in diabetic patients and is associated with greater severity and more diffuse PAD relative to nondiabetic patients [14–16]. However, there currently is no direct evidence of a connection between AIP and diabetic foot osteomyelitis. In the present study, we examined the relation between AIP, routine blood lipid concentrations, and diabetic foot osteomyelitis and demonstrate that AIP is a more clinically useful biomarker for that disease than traditional blood lipid assays.
Patients and Methods
Design and participants
This was a case-control study in which all study subjects were patients with DFU who had been admitted to Beijing Shijitan Hospital from September 2015 to April 2018. The subjects had osteomyelitis, while the control cases were patients without osteomyelitis. Propensity score matching based on age, gender, and diabetic history was applied when selecting controls. The study protocol was reviewed and approved by the institutional ethics committee, and consent was obtained from each patient.
Diagnosis of diabetic foot osteomyelitis
The criteria for the admission of patients were defined by the World Health Organization (WHO) guidelines on diabetic foot disease published in 1999: “Diabetic foot” refers to lower limb infection, ulceration, or deepness in diabetic patients associated with neuropathy and various degrees of vascular disease.
According to the guidelines of the International Diabetes Foot Working Group, there are several diagnostic criteria for osteomyelitis including: (1) the presence of cellulitis in ulcer wounds; (2) exposure of bone; (3) positive pathogenic bacteria culture in deep bone tissue; (4) radiologic or radionuclide scanning images suggestive of inflammatory manifestations of bone tissue; and (5) bone histopathologic biopsy diagnosis and neutrophils or chronic inflammation cell invasion. With a history of diabetic foot disease, patients meeting three of the above criteria can be said to have osteomyelitis [17].
We excluded participants who met any of the following criteria: (1) took lipid-lowering drugs in the past three months; (2) had seriously deficient investigation data; (3) had severe liver and kidney disease or heart failure; (4) had a malignant tumor or immune system disease; (5) had hypothyroidism or hyperthyroidism; or (6) presented with severe infection.
Color Doppler ultrasound (CDU) test
The GE LOGIQ9 and SIEMENS ACUSON Sequoia 512 CDU detector was used, with a probe frequency setting of 7.5–12 MHz. The angle between the sound beam and the blood flow was controlled to 60° or less. Before examination, patients were instructed to maintain the supine position to expose the lower limbs fully and extend the thighs slightly outward. The probe was placed at the root of the thighs along the inguinal area to scan the femoral, popliteal, anterior tibial, posterior tibial, and dorsal pedal arteries. The smoothness, intima–media thickness (IMT), plaque size, and the shape and echo of the lower-extremity arterial intima were determined by two-dimensional ultrasound scans. We also examined the tissues to see if there was stenosis and occlusion of lower-extremity arterial lumen. Hemodynamic changes were observed by color Doppler flow imaging (CDFI).
Body examination
A health check was performed in the morning after patients fasted overnight. The anthropometric index was operated by a qualified physician. Patients were required to wear shoes to measure weight using a calibrated balance scale. Patient height was measured using a calibrated range finder. Body mass index (BMI) was calculated as body weight (in kilograms) divided by the square of their height (in meters).
All participants were required to fast for at least 12 hours, and elbow venous blood was collected in a vacuum tube the next morning. Peripheral blood was mixed with ethylene diamine tetraacetic acid and stored in a refrigerator at 4°C for analysis within 24 hours. Fasting blood glucose (FBG) was measured by the oxidase method (HOMA, Beijing, China). Blood lipid indicators, including TG, total cholesterol (TC), HDL-C, and low-density lipoprotein–cholesterol (LDL-C), were measured with a Hitachi 7600 automatic analyzer (Hitachi, Tokyo, Japan).
Statistical methods
Normality distributions of continuous variables were determined by the Kolmogorov-Smirnov test. Continuous variables underlying normal distribution were reported as mean±standard deviation (SD) and compared using analysis of variance. Otherwise, nonparametric methods were utilized. Categorical variables were described with percentages and compared using the χ2 test. Multivariable logistic regressions were applied to evaluate the odds ratio (OR) and 95% confidence interval (CI). We then tested the discriminating ability for atherogenic index of plasma (AIP) for osteomyelitis. The cut-off values of AIP as an osteomyelitis predictor were determined by receiver operating characteristic (ROC) analysis and area under the curve (AUC) values.
Results
Anthropometric index of participants
From September 2015 to April 2018, 440 participants were enrolled in this study with an average age of 66 years; 65.7% of the participants were male. We selected 165 diabetic patients with osteomyelitis and 275 control patients without osteomyelitis using group matching by age, gender, and diabetic history (Table 1). Using these diagnostic criteria, we investigated the prevalence of each symptom among all the 165 patients with a diabetic foot and osteomyelitis. Our analysis revealed that 151 patients (91.5%) had cellulitis in ulcer wounds, 88 (53.3%) had bone tissue exposure, 112 (67.8%) had positive pathogenic bacteria culture in deep bone tissue, 143 (86.7%) had inflammatory manifestations of bone tissue indicated by radiologic or radionuclide images, and 145 (87.8%) had immune cell invasion revealed by histopathologic bone biopsy.
Baseline Characteristics According to Presence of Osteomyelitis in Patients with Diabetic Foot Disease
AIP = atherogenic index of plasma; BMI = body mass index; FBG = fasting blood glucose; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; TC = total cholesterol; TG = triglycerides.
Compared with controls, patients with osteomyelitis had significantly higher white blood cell counts and percentage of neutrophils and lower concentrations of albumin and hemoglobin (p < 0.001) (Table 1). According to the examination results, osteomyelitis patients and controls had no differences in height, weight, BMI, or FBG concentration (Table 1). However, patients with osteomyelitis had significantly higher concentrations of TC and LDL-C, with lower HDL-C levels (p < 0.001).
All patients were examined by CDU to study the arterial blood supply to the lower extremities. As shown in Table 2, this study revealed that the prevalence of plaques, stenosis, and occlusion was higher in the osteomyelitis group than in the non-osteomyelitis group, so patients with osteomyelitis had a poorer arterial blood supply to the foot.
Comparison of Lower-Extremity Arterial Status in Patients with Diabetic Food Disease with (DFO) and without (DF) Osteomyelitis
Impact of AIP on diagnosis
The AIP, calculated as the logarithmic transformation of the TG/HDL-C ratio, ranged from −2.18 to 2.28 among the 440 participants. The mean AIP in the 165 patients with osteomyelitis was 0.23 ± 0.24, which was significantly higher than the mean AIP of the controls (0.11 ± 0.39) (see Table 1).
The AIP value was entered in the logistic regression model as quartiles, defined as < −0.029 (Q1), −0.029 to 0.142 (Q2), 0.142 to 0.317 (Q3), and >0.317 (Q4), with the lowest quartile (Q1) used as the reference. Compared with patients with low AIP values (< −0.029), patients with higher AIP had a considerably higher risk of osteomyelitis, with ORs of 2.15 (95% CI 1.16–3.99), 3.53 (1.93–6.47), and 4.56 (2.49–8.35), respectively. After fully adjusting for age, gender, BMI, TC, TG, LDL-C, HDL-C, FPG, white blood cell count, percentage of neutrophils, albumin concentration, and hemoglobin concentration, the AIP remained associated with a higher risk of osteomyelitis, with ORs of 1.81 (95% CI 0.71–4.61), 4.70 (1.88–11.75), and 5.03 (2.06–12.25), respectively (Table 3). Additionally, we performed subgroup analysis according to age and gender. Significant associations were identified between AIP and osteomyelitis among participants older than 65 years old as well as male participants with ORs for trend 2.59 (95% CI 1.65–4.04) and 1.82 (1.29–2.56), respectively (Table 3).
Odds Ratio (OR) and 95% Confidence Interval (95% CI) of Diabetic Foot Osteomyelitis According to Atherogenic Index of Plasma (AIP)
Adjusted for age, gender, BMI, total cholesterol, triglycerides, low-density lipoprotein-cholesterol, high-density lipoprotein-cholesterol, and free blood glucose.
Adjusted for age, gender, body mass index, total cholesterol, triglycerides, low-density lipotrotein-cholesterol, high-density lipoprotein-cholesterol, free blood glucose, white blood cell count, percentage of neutrophils, albumin and hemoglobin concentrations.
Next, we created an ROC plot depicting specificity (shown on the X axis) as a function of sensitivity (indicated on the Y axis). The ROC and AUC analysis for AIP are shown in Fig. 1. With an AUC value of 0.870, we determined the optimal cut-off value for AIP as a diagnostic biomarker to be 0.184. This cut-off provides a sensitivity of 84.3% and a specificity of 83.1% for diagnosing osteomyelitis, the optimal values that could achieved with our dataset. These results indicate that an AIP >0.184 has the strong potential to discriminate osteomyelitis among patients with diabetic foot disease.
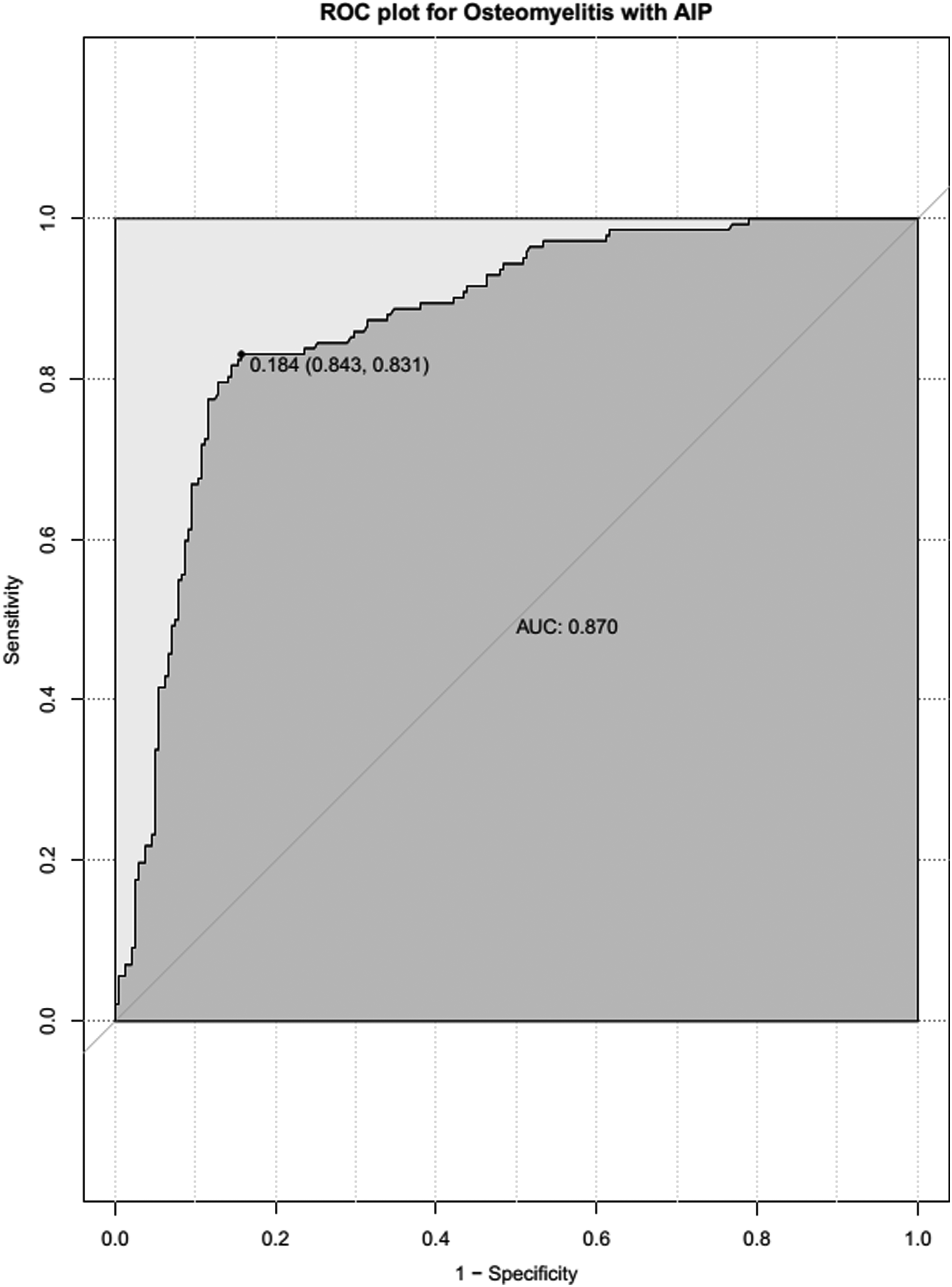
The ROC curve for diabetic foot osteomyelitis with atherogenic index of plasma (AIP). The area under the curve value of AIP in the discriminatory analysis of diabetic foot osteomyelitis was 0.870. The cut-off value for AIP of 0.184 presented the most significant sensitivity of 84.3% and specificity of 83.1%.
Discussion
In this case-control study, we examined the relation between AIP values and the presence of osteomyelitis in patients with diabetic foot disease. The results support the use of AIP as a diagnostic indicator for osteomyelitis among both male and female patients and suggest that this index could be applied in clinical practice. Almost all cases of osteomyelitis in the feet of patients with diabetes result from continuous transmission to soft tissue from adjacent ulcer infections [17]. In these cases, PAD is associated with an approximately two-fold higher risk of foot infection, as well as greater severity of infection in the lower extremities [6]. Therefore, lower extremity atherosclerosis has been proposed to have a central role in the development of diabetic foot osteomyelitis [18].
The small and dense LDL and serum HDL-C esterification rate can be used to evaluate the occurrence of atherosclerosis and the severity of the disease, but these metrics are prohibitively expensive and are not ideal for large-scale clinical application [19]. In contrast, AIP is determined by calculations based on traditional blood lipid measurements and is more convenient and economically feasible than the esterification rate and appears to have greater diagnostic value when applied clinically. Therefore, as a new comprehensive indicator of blood lipids, AIP has received increasing attention. Once AUC and ROC analysis was applied to assess the discriminatory potential of AIP in osteomyelitis among patients with diabetic foot disease, we achieved high sensitivity and specificity for the prediction of osteomyelitis, indicating that AIP could be valuable in the clinical management of these patients.
Even when used alone, AIP could be particularly useful in predicting the presence of osteomyelitis. This view is supported by our clinical evidence suggesting that elevated AIP values are more common among diabetic patients with foot ulcers than in those without ulcers, and even higher AIP values can be found in patients with infected DFUs versus those with noninfected DFUs. At a cut-off of 0.184, AIP was our most sensitive and accurate single marker for diabetic foot osteomyelitis and was able to identify nearly 85% of subjects with underlying bone involvement. Based on this finding, calculation of AIP could begin to have a heightened role in primary care and other non-specialty settings, where ulcer characteristics such as wound depth are not immediately usable as patients wait to be seen for ulcer debridement by the appropriate consultant.
Despite strong evidence for the utility of AIP in the diagnosis of osteomyelitis, several limitations exist that warrant further study. First, the design of this case-control study was observational, which produces a correlated association rather than a causality correlation. Experimental testing using animal models of diabetic foot disease will be required to establish the causal relations between elevated AIP and osteomyelitis. Second, our study highlights the heterogeneous use of fast and efficient reference tests to confirm the diagnosis of diabetic foot osteomyelitis and does not yet achieve the robustness and accuracy of a “gold standard” method. Third, most of the patients in our study had neuroischemic ulcers; only 23 had neuropathic diabetic foot lesions without ischemic condition. Although we identified a positive relation between AIP and diabetic foot osteomyelitis with neuroischemic ulcers, the number of patients with neuropathic ulcers was insufficient to examine the correlation between AIP and diabetic foot among patients with neuropathic ulcers with an adequate blood supply. Finally, inherent advantages and limitations exist in a single-center analysis, and we encourage treatment centers elsewhere to confirm our findings and examine the potential use of AIP in the clinical management of diabetic foot lesions.
Conclusion
This study investigated the relation between the atherogenic index of plasma (AIP) and osteomyelitis among patients with diabetic foot disease. We found that AIP was significantly associated with diabetic foot osteomyelitis and had potential use as a biomarker for the diagnosis of this disorder in clinical practice in the future.
Footnotes
Author Disclosure Statement
All authors warrant that they have no conflict of interest in connection with this article. They all had access to the data used in the study and hold final responsibility for the decision to submit this manuscript for publication. This study was supported by the National Natural Science Foundation of China (No. 81473502)