
Abstract
Abstract
Background:
This study evaluated the efficacy and safety of ertapenem versus a combination of gentamicin plus metronidazole in pediatric patients with diffuse peritonitis attributable to perforated appendicitis.
Methods:
From January 2017 to January 2019, 80 pediatric patients with a median age of 13 years who underwent laparoscopic appendectomy because of perforated appendicitis with diffuse peritonitis were enrolled. The patients were randomly assigned to two groups of 40 patients each to receive ertapenem or combination therapy. The groups were compared regarding demographic/clinical data and outcomes of treatment. The main outcome measures were duration of hospitalization, time to achieving an afebrile state, post-operative complications, antibiotic treatment failure, and time to the start of enteral feeding.
Results:
The median length of the hospital stay was 5 and 8 days in the ertapenem and combination therapy groups, respectively (p < 0.0001). Patients in the ertapenem group took two days less to become afebrile (p < 0.0001). No post-operative complications were recorded in the ertapenem group, whereas in the combination therapy group, three complications were noted, but this difference was not significant (p = 0.2392). Furthermore, all patients in the ertapenem group responded to therapy, whereas in the combination therapy group, two antibiotic treatment failures were recorded, a diffrence that again was not significant (p = 0.4739). There was no difference in the time to the start of enteral feeding in the two groups.
Conclusion:
Both ertapenem and gentamicin plus metronidazole are safe and effective therapeutic options for the treatment of diffuse peritonitis in pediatric patients. Treatment with ertapenem results in lower complication rates, a shorter time to an afebrile state, and a shorter hospital stay.
Acute appendicitis is the the most common cause of sudden abdominal pain in pediatric patients, and diffuse peritonitis is its commonest complication [1]. In the pediatric population, complicated intra-abdominal infections usually are caused by perforation of the appendix, which may be one of the most important causes of morbidity [1,2]. The most important thing in the management of diffuse peritonitis is to establish the diagnosis in a timely fashion and to perform appropriate surgical treatment, followed by adequate antimicrobial therapy, promptly [3].
Nowadays, intravenous antibiotic therapy following appendectomy is standard treatment in pediatric patients with perforated appendicitis. Many protocols are used, and no consensus has yet been reached on the optimal regimen for children with diffuse peritonitis because of perforated appendicitis. Because diffuse peritonitis is a polymicrobial infection, the antibiotics given need to have broad-spectrum efficacy, especially against anaerobes and gram-negative enteric bacilli [4]. Many regimens have been evaluated in children with perforated appendicitis, and one effective combination is gentamicin once daily plus metronidazole three times daily. [5]. One the other hand, once-daily ertapenem, a carbapenem antibiotic, may be a useful alternative for the treatment of pediatric patients with mixed aerobic and anaerobic infections and severe intra-abdominal infections [6].
The primary endpoint of this randomized study was a comparison of combination antibiotic therapy (gentamicin plus metronidazole) with monotherapy (ertapenem) in children with diffuse peritonitis secondary to perforated appendicitis, especially in terms of treatment failure and post-operative infectious complications.
Patients and Methods
Patients
A total of 80 pediatric patients, 5 to 17 years of age, who underwent surgery because of perforated appendicitis with diffuse peritonitis between January 2017 and January 2019 in the Department of Pediatric Surgery, University Hospital of Split, were enrolled in this randomized study. The study protocol was approved by the Ethics Committee of our hospital. The inclusion criteria were patients of both genders, 5–17 years of age, with perforated appendicitis and diffuse peritonitis. Exclusion criteria were peritonitis of any genesis except appendicular, open appendectomy or conversion from laparoscopic to open appendectomy, local peritonitis or perityphlic abscess, history of allergy to the investigated antibiotics, chronic or terminal illness, and more than 24 h of any systemic antibiotic therapy. Diffuse peritonitis was defined as an inflammation of the entire serosal membrane that lines the abdominal cavity and the organs contained therein. Local peritonitis was defined as a localized inflammatory process (abscess).
The following data were recorded for each patient: Demographic information (age, sex, Body Mass Index [BMI]); pre-operative laboratory tests (white blood cell [WBC] count, serum C-reactive protein [CRP] concentration); clinical data (duration of symptoms, body temperature, and physical examination findings), and treatment outcomes (duration of hospitalization, time to becoming afebrile, post-operative complications, antibiotic treatment failure, and time to the start of enteral feeding). Treatment failure was defined as insufficient control of the source of the intra-abdominal infection (clinical signs, fever, elevated inflammatory markers) or as inadequate antimicrobial spectrum of the prescribed drug. A clinical examination and laboratory analysis were performed pre-operatively in all of the patients. The ALVARADO score and Pediatric Appendicitis Score were calculated in all patients prior to surgery [7]. Also prior to surgery, the majority of the patients received an abdominal ultrasound examination.
Randomization and sample size calculation
Calculation of the necessary sample size was based on the previously reported data (2 ± 2 days' difference in the length of the hospital stay [LOS] and a 10% difference in the proportion of post-operative infectious complications). We estimated that the minimum sample size needed to detect statistical significance at 0.05 and with a detection power of 80% was 37 patients in each group. Taking into account uncertainties in assumed standard deviation for LOS and possible loss of patients after randomization, the sample size was increased to 40 for each group, which we were able to achieve. Patients in the first group were treated with a combination (gentamicin + metronidazole), and patients in second group received monotherapy (ertapenem). The allocation of participants to each group was performed using a random number generator, and block randomization with a block size of four was used. A statistician who did not have any contact with the surgeons performed the randomization, with the probability of each participant entering either group being 50%.
Antibiotic usage and discharge criteria
In the first group of patients, a combination of gentamicin (Belupo, Koprivnica, Croatia) (3–5 mg/kg once daily) and metronidazole (Efloran, Krka, Novo Mesto, Slovenia) (7.5 mg/kg three times a day) was used, whereas in the second group, children received ertapenem alone. For children up to 12 years of age, ertapenem 30 mg/kg was divided into two daily doses, with a maximum total daily dose of 1 g. Children 13 years of age or older received 1 g of ertapenem as a single dose.
The criteria for hospital discharge included adequate post-operative food and water intake, pain control, and resolution of fever. Any patient who developed a post-operative abscess was treated with antibiotics chosen according to the causative pathogen(s). Microbiologic analysis of aspirates collected from the abdominal cavity at the time of surgery was performed in all children.
Outcome measurements
The primary outcome measures for comparison were post-operative complications, time to being afebrile, antibiotic treatment failure, and duration of hospitalization. Post-operative complications included incision infection, bleeding, bowel obstruction, ileus, and abscess formation. The secondary outcome variables were causative microorganisms and time to the start enteral feeding.
Surgery
A supine position, combined with the Trendelenburg and left lateral position, was used in all patients. A Veress needle was introduced through a 5-mm supra-umbilical incision, and CO2 was insufflated at a pressure of 8–12 mm Hg, depending on the patient's age and body weight. After achievement of pneumoperitoneum, laparoscopic appendectomy was performed using the three-trocar technique (two 5-mm and one 10-mm trocar). The first 5-mm trocar was placed through the supra-umbilical incision for introduction of the endoscope. The second 5-mm trocar was placed in the right upper abdominal quadrant and the 10-mm trocar in the left lower abdominal quadrant. Dissection of the mesoappendix was performed using a longitudinal or torsional Harmonic Scalpel [1]. The appendicael base was secured with an endoloop or polymeric clips [2]. A disposable specimen retrieval bag was used to remove the appendix from the abdominal cavity through the 10-mm trocar.
Statistical analysis
The data were analyzed using Statistical Package for the Social Sciences version 24.0 (IBM Corp, Armonk, New York, USA). Distributions of categorical data were described by absolute rates and percentages. Medians and interquartile ranges (IQRs) were used to describe quantitative data. Statistical analysis of the categorical data was performed using the χ2 test, while the Mann–Whitney U test was used to calculate differences between the groups in the median values of quantitative variables. All p values <0.05 were considered statisticaly significant.
Results
During the study period, 84 children, with a median age of 13 (IQR 10.5–15.5) years were found to have diffuse peritonitis because of perforated appendicitis and underwent laparoscopic appendectomy. Four children were removed from the analysis because they met one of criteria for exclusion. Thus, 80 children were included. No difference between the two groups was seen with respect to gender, age, BMI, fever, WBC count, CRP concentration, duration of symptoms, or clinical findings (Rowsing, Blumberg, or Grassman signs or abdominal guarding) was found at baseline (Table 1).
Demographic, Laboratory, and Clinical Data
Mann-Whitney U test.
χ2 test.
BMI = Body Mass Index; CI = confidence interval; CRP = C-reactive protein; IQR = interquartile range.
Overall, the monotherapy group (2 days; IQR 1–2.5 days) had a shorter time to becoming afebrile than the combination therapy group (4 days; IQR 3–5 days) (p < 0.0001) (Fig. 1). The LOS was significantly shorter in the monotherapy group (5 days; IQR 5–6 days) than in the combination therapy group (8 days; IQR 7–8.5 days) (p < 0.0001). The range of the LOS in the combination therapy group was 7–10 days, with two patients having unusually long stays (11 and 13 days), whereas in the monotherapy group, the LOS was 4–7 days, with no prolonged stays (Fig. 2). Regarding the time to full oral intake and consumptionn of a regular diet, therapy failure, and complication rates in the two groups, no significant difference was found (Table 2). Overall, the incidence of post-operative complications (3.75%; 3 of 80) and therapy failure (2.5%; 2 of 80) was low. Post-operative complications were seen only in patients in the combination therapy group. In this group, the abscess rate was 5% (2 of 40) and the incision infection rate was 2.5% (1 of 40). Therapy failure was recorded in 5% (2 of 40) of the patients in the combination therapy group and none in the monotherapy group (Table 2).

Box plot of time to achievement of afebrile state depending on antibiotic therapy (p < 0.0001).
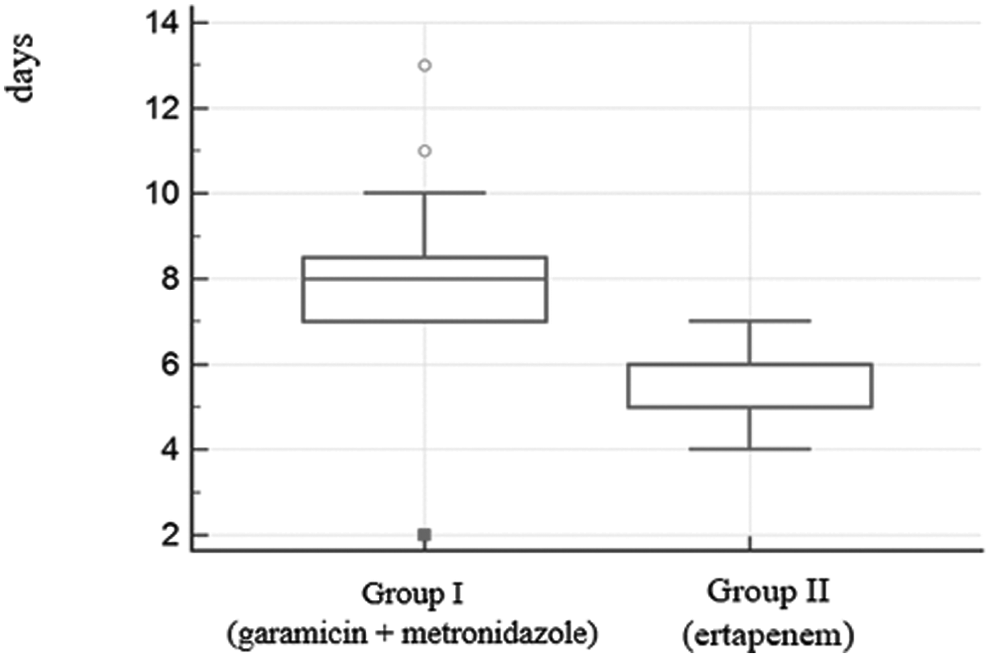
Box plot of hospital stay depending on antibiotic therapy (p < 0.0001).
Treatment Outcomes
Mann-Whitney U test.
χ2 test.
IQR = interquartile range.
A similar distribution of bacterial species was isolated from the abdominal aspirates at the time of surgery in both groups. The most common isolate in both groups was Escherichia coli (combination therapy group 28 [70%] and monotherapy group 30 [75%]). The distribution of other pathogens is presented in Table 3. In one case, a multi-drug-resistant Proteus was isolated in the combination therapy group, whereas no resistant pathogens were recovered from speciemns from the ertapenem group.
Microbiological Analysis of Aspirates from Abdominal Cavities of Patients with Perforated Appendicitis and Diffuse Peritonitis
Discussion
According to the results of the present study, monotherapy with ertapenem and combination therapy with gentamicin plus metronidazole are both effective for the treatment of diffuse peritonitis secondary to perforated appendicitis in the pediatric population. Both regimens showed low rates of post-operative complications, including formation of abscess. There were no cases of post-operative complications when ertapenem was used, and three post-operative complications were recorded in children who received combination therapy. Also, therapy failure was recorded in two patients in the combination therapy group and no failures in the monotherapy group. A significantly shorter time to an afebrile state and shorter LOS was found when ertpenem was used. In sum, compared with combination therapy, ertapenem showed higher efficacy and offers a simpler option for the treatment of diffuse peritonitis following perforated appendicitis in children.
The small number of the patients included in the analysis and the fact that the study medications were administered in an unblinded manner are the main limitations of this study. The study was open label because the antibiotics used have different administration frequencies. Also, administration of placebos is not possible in seriously or acutely ill children.
Currently, there are many antibiotic protocols used for the treatment of diffuse peritonitis attributable to perforated appendicitis following appendectomy by pediatric surgeons, as there are many opinions regarding choice of antibiotic, route of administration (oral or parenteral), and duration of treatment [6, 8]. Recent studies have shown that monotherapy with newer broad-spectrum antibiotics has been as effective as combination therapy [6, 9]. Many studies have shown that ertapenem is a valuable antibiotic against the bacteria most commonly isolated in children with intra-abdominal infections, but on the other hand, in patients with hospital-acquired infections infected with organisms such as Pseudomonas aeruginosa or enterococci, ertapenem is not the drug of choice [10]. Children are extremely sensitive to multiple daily parenteral administration of therapy, so one of the important advantages of ertapenem in the pediatric population is its simple (once daily) dosing schedule compared with combination therapy, which requires a multi-dosing schedule for the treatment of diffuse peritonitis. The other potential advantage of once-daily dosing of a single antibiotic in hospitalized children include reduction in the rate of possible medical errors and a decrease in resource utilization [11].
Yellin et al. in their randomized study, compared ertapenem with ticarcillin/ clavulanic acid in 112 pediatric patients with complicated intra-abdominal infections. In the children in whom ertapenem was used, the clinical response rates were significantly higher than in children treated with combination therapy [12].
In contrast, Dalgic et al. reported similar efficacy response rates in children who received combination therapy and those treated with ertapenem as judged by the length of antibiotic therapy, LOS, and time to initiation of oral intake and consumption of a regular diet [6]. As in our study, they noticed that children in the combination therapy group had a higher incidence of a post-operative abscesses than the patients in the group receiving ertapenem alone. Hurst et al. compared combination therapy (ceftriaxon plus metronidazole) and ertapenem and found that both regimens are effective in the treatment of perforated and non-perforated pediatric appendicitis, resulting in low rates of post-operative abscess formation. They reported shorter times than we did to reaching an afebrile state when combination therapy was used. However, they saw no difference in incision infection rates, LOS, re-admission, and abscess formation [12].
Catena et al. compared combination therapy (ampicilin + sulbactam) and ertapenem and found that ertapenem was associated with significantly lower rates of complications and treatment failure. They concluded that three-day treatment with ertapenem is safe and effective for patients with localized intra-abdominal infections [13].
In a meta-analysis, Falagas et al. collected data from six randomized clinical trials involving subjects with complicated intra-abdominal infections (only one performed in a pediatric population) that compared monotherapy with ertapenem against different combination therapies. They concluded that ertapenem is safe and effective for the treatment of complicated intra-abdominal infections [14].
Obinwa et al. performed microbiologic analysis of aspirates taken from the abdominal cavity intra-operatively in children patients with secondary bacterial peritonitis attributable to perforated appendicitis. They found that E. coli and mixed anaerobes were the microorganisms most commonly isolated. These findings are similar to those of our study, in which E. coli was the most common microorganism. The authors concluded that failed initial empirical antimicrobal therapy and amoxicillin/clavulanic acid-resistant E. coli contribute to a higher frequency of post-operative infectious complications [15]. Antibiotic therapy should be prescribed only in pediatric patients with perforated appendicitis, as there is no evidence endorsing routine prescription of antibiotics for pediatric patients undergoing appendectomy for non-perforated appendicitis [16].
In conclusion, this study showed that ertapenem is safe and effective therapy for perforated appendicitis with diffuse peritonitis in a pediatric population.
Footnotes
Author Disclosure Statement
The authors state that no competing financial interests exist.