
Abstract
Abstract
Background:
Patients with periampullary tumors frequently undergo endoscopic biliary investigations and biliary drainage (BD) prior to surgery. Recent literature shows a shift of the biliary microbiome toward more resistant bacteria in patients having BD. This study aimed to evaluate the local microbiome and changes induced by BD and related antibiotic exposure and to consider the choice of antibiotic for peri-operative prophylaxis.
Methods:
A single-center retrospective cohort study included patients operated on for periampullary tumors between January 2013 and November 2017. All patients had intra-operative bile samples taken for culture and peri-operative antibiotic use as well as documentation of complications according to the Dindo-Clavien classification.
Results:
A total of 37 patients were included. All received pre-operative endoscopy, and 29 (78%) had BD preceded by administration of ceftriaxone or metronidazole. Intra-operative antibiotic prophylaxis consisted of cefuroxime (92%) or ceftriaxone (13%) combined with metronidazole (100%). Bacterial contamination of bile samples was more common in the BD group than in the no biliary drainage (NBD) group (93% vs 38%; p < 0.01). A shift was observed from bile containing mainly Escherichia coli and Streptococcus spp. toward Enterococcus faecalis (0 in the NBD group versus 44.8% in the BD group; p < 0.01), Enterococcus faecium (0 versus 23%; p = 0.3), and Candida albicans (0 versus 34.5%; p = 0.08). Post-operative antibiotic modifications were common. No difference was found regarding Dindo-Clavien complications, post-operative stay, or antibiotic use in the two groups, although one patient in the NBD group who had pre-operative biliary endoscopy with antibiotic prophylaxis developed a fatal septic clot caused by Escherichia coli resistant to cefuroxime.
Conclusions:
We observed a significant change toward colonization by enterococci and fungi in the microbiome of patients who had pre-operative biliary investigations or drainage with antibiotic prophylaxis. These findings indicate that bile samples should be obtained systematically during surgery for periampullary tumors to guide any post-operative antibiotic therapy and peri-operative antibiotic prophylaxis and might need adaptation to target the modified microbiome.
Pancreatic or periampullary tumors are rare, with an incidence of 1–10/100,000 person-years, but are associated with a high case–fatality rate, survival being as low as 6% in the five years following the diagnosis of pancreatic adenocarcinoma. Early detection is difficult, as no efficient screening method exists; and diagnosis often is made when patients exhibit signs of biliary obstruction such as jaundice and pruritus, suggesting locally advanced disease [1,2]. At the time of diagnosis, only 10%–20% of patients are considered candidates for surgery. Evaluation of resectability involves a multidisciplinary approach to obtain precise staging, because distant metastasis constitute a contra-indication to surgery and are present in 50%–60% of the patients, whereas locally advanced disease (30%–40%) might benefit from neo-adjuvant therapy to convert a non-resectable cancer to a resectable one [3]. Surgical resection is the only potentially curative treatment but rarely is feasible [2].
A long-lasting debate exists over whether surgery should be performed immediately in obstructive disease or if biliary drainage (BD) should be performed first. Many approaches exist to achieve biliary drainage, such as the endoscopic approach during which a plastic or metal stent is placed in the distal biliary tree after sphincterotomy, or by transhepatic radiologic drainage.
Initially, surgery in patients with jaundice was thought to increase post-operative complications, and biliary decompression was believed to improve liver function and coagulation [4]. However, a recent randomized controlled trial suggested that immediate surgery is associated with fewer complications than prior BD and might be preferred [5]. The high complication rate observed in this study in patients undergoing BD was explained partly by the use of plastic stents, which have higher occlusion rates and need for exchange than metal stents. However, pre-operative BD still is a common procedure, especially when the serum bilirubin concentration is high [6].
One growing concern regarding BD is bile contamination, favoring colonization with resistant bacteria. The aim of this study was to characterize the local bile microbiome and changes induced by BD and related antibiotic administration and to assess the pertinence of our institutional antibiotic prophylaxis. This study was approved by the Ethics Committee of the Commission Cantonale d'Ethique de la Recherche CCER (Project ID 2017-01912).
Patients and Methods
This was a single-center retrospective study conducted on patients operated on at Geneva University Hospital for periampullary tumors between January 2013 and November 2017. Details concerning patients who underwent cephalic duodenopancreatectomy were retrieved from the institutional registry. Only patients having microbiologic bile samples collected during surgery were included.
Prior to surgery, all patients underwent diagnostic endoscopy with concomitant placement of a plastic or metal biliary stent if symptomatic cholestasis was present. If this was unsuccessful, drainage was achieved by radiologic transhepatic manipulation. Depending on the procedure complexity, antibiotics (ceftriaxone, ciprofloxacin, and/or metronidazole) were administered during the procedure.
During surgery, metronidazole combined with cefuroxime or ceftriaxone was used as peri-operative antibiotic prophylaxis, the doses being repeated every three to four hours following local guidelines. After incision closure, antibiotic prophylaxis was either stopped or extended for as long as 48 hours, depending on the treating physician and intra-operative findings. Post-operative antibiotic therapy, if needed, was adjusted by the treating physician, sometimes with infectious disease team expertise.
Data concerning post-operative stay, bile samples, and antibiotic use were collected from the computerized institutional medical record system “Dossier Patient Informatisé.” Complications were graded until discharge according to the Clavien-Dindo scoring system [7,8]. Pancreatic fistula was defined as an amylase concentration in the drains exceeding three times the upper limit of normal for the serum amylase concentration and was managed mainly by percutaneous computed tomography-guided drainage, re-laparotomy, or both as appropriate.
The primary endpoint of this study was the difference in bacteriologic agents found in bile samples, focused mainly on cephalosporin-resistant species. On the basis of available data, we anticipated a prevalence of 35% for Enterococcus faecalis in the stented group vs 0 in the native group [4,9]. The calculated total sample size (using 5% alpha error and 80% power) was 38. SPSS for Mac (version 24) (SPSS Inc. Chicago, IL, USA) was used for statistical analysis. Significance statements refer to p values <0.05 in two-tailed tests. The Pearson χ2 or Fisher exact test were used for categorical variables. The Student t-test was used for continuous variables with a previous Levene-F test to assess variance.
Results
Thirty-seven patients were included in the study, 29 (78%) in the BD group and 8 (22%) in the no biliary drainage (NBD) group. Table 1 displays patient characteristics, and detailed histopathologic diagnoses are displayed in Fig. 1. Of the patients, 29 (78%) had a malignant disease. A higher proportion of malignant disease was found in the BD group (86.2%) than in the NBD group (50%) (p = 0.049).

Histopathologic findings.
Patient Characteristics
χ2 or Fisher exact test.
Student t-test.
NA = not applicable; NBD = no biliary drainage; BD = biliary drainage; SD = standard deviation.
Data concerning antibiotic use during pre-operative endoscopic stenting could be retrieved from 21 patients, 8 of them having been referred after BD. Nine (42.9%) of them had antibiotic prophylaxis during BD; eight of them received ceftriaxone (38.1%) and one received piperacillin/tazobactam (4.8%) in an infectious context for therapeutic purposes.
Micro-organisms grew from the bile cultures in 30 of 37 samples (81%). A higher proportion of positive bile cultures was found in the BD group (93.1%) than in the NBD group (37.5%) (p = 0.002). Micro-organisms found in the NBD group consisted of Escherichia coli and Streptococcus spp. Enterococcus faecalis, Enterococcus faecium, and fungal colonization by Candida albicans prevailed in the BD group. Figure 2 summarizes these findings, and Table 2 provides statistical significance data. The most common antibiotic resistance found was non-susceptibility to amoxicillin/clavulanic acid (25% in the NBD, 24.1% in the BD group). No statistical difference was found in antibiotic resistance between the groups (Table 3), but our study was not designed to observe this finding. Enterococcus species or fungi colonization of BD samples did not have a significant clinical impact.
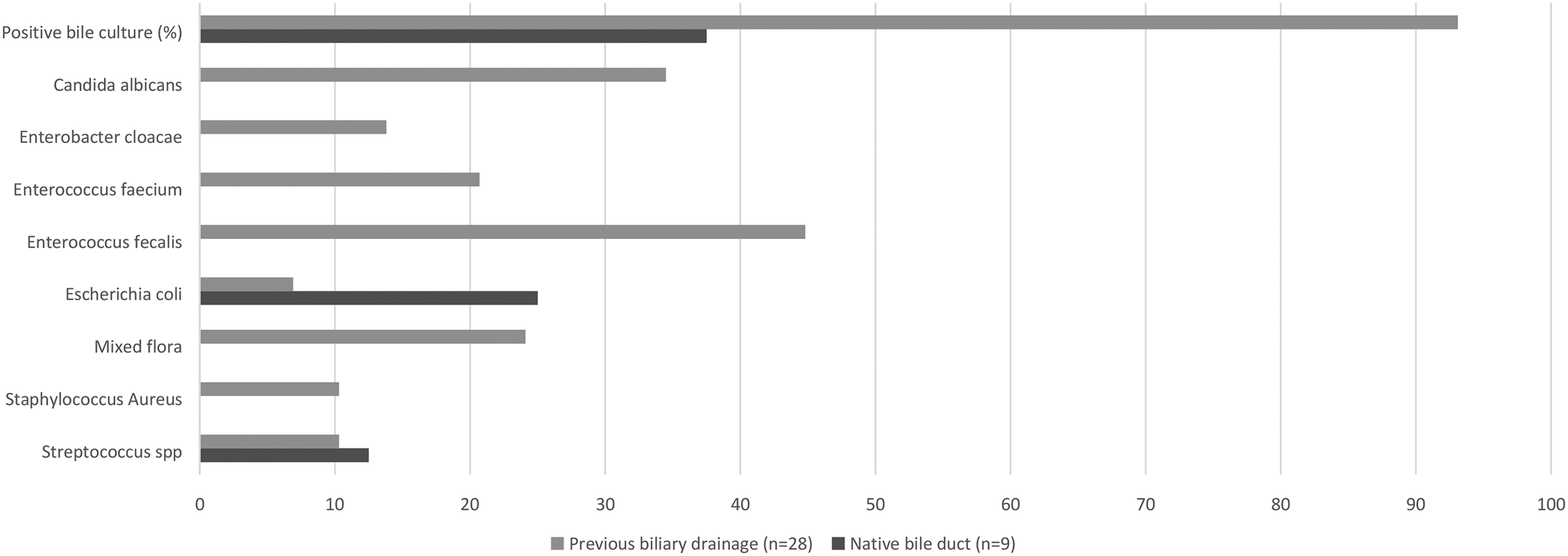
Microbiologic findings.
Microbiologic Findings a
Species accounting for fewer than three positive cultures not displayed.
χ2 or Fisher exact test.
NBD = no biliary drainage; BD = biliary drainage.
Antibiotic Resistance of Bacteriologic Agents (%)
χ2 or Fisher exact test.
NBD = no biliary drainage; BD = biliary drainage.
Post-operative complications observed in both groups included pancreatic fistula, ileus, collection requiring radiologic percutaneous drainage, and need for re-laparotomy. A Grade ≥3 complication was observed in 29.7% of the patients, without a significant difference between the groups. The most severe complication was the death of an 82-year old patient admitted for cholangitis related to an extensive duodenal ampulloma. Pre-operative work-up included endoscopic examination with antibiotic administration and no stenting. The patient developed a fatal septic clot in the early post-operative period while receiving conventional antibiotic prophylaxis, and bile cultures showed a cefuroxime-resistant E. coli.
Discussion
Standard of treatment: What is the role of pre-operative biliary stenting?
The use of BD rather than immediate surgery for patients with periampullary tumors is a continuing debate initially thought to be beneficial to patients, as judged by post-operative outcome. Increasing knowledge and evidence cast doubt on this assumption [10] in the absence of post-operative benefits, suggesting that immediate surgery might be the preferred option whenever possible. Biliary drainage increases post-operative infectious complications without an impact on severe complications or the mortality rate [11]. In our institution, endoscopic placement of a bile stent remains a popular procedure and often is a step toward surgery in obstructive tumors in symptomatic patients. Although some centers have described changes and declines in pre-operative biliary stent use, inertia and individual center guidelines still make it a widely used procedure [12].
Impact of bile contamination and microbiome change on post-operative course
Biliary drainage has been shown in many studies to increase bile contamination and thereby to modify the biliary microbiome [13,14]. A recent meta-analysis showed that positive bile culture was strongly associated with increased morbidity and mortality rates, although the data could not show this association to be linked directly to BD [15]. Scheufele et al. demonstrated a shift like the one observed in our study, with a native bile microbiome composed mainly of E. coli (45%) changing toward contamination with Enterococcus faecalis (37.7%) and Enterobacter cloacae (20.4%). Positive bile culture induced a fourfold increase in post-operative incision infection, and Enterococcus faecium as well as Citrobacter spp., typically not found in native bile, appeared as independent risk factors for site infection [4]. Fong et al. conducted a similar study with a sample of 1,623 patients, who underwent duodenopancreatectomy at three institutions, two of them realizing systematic bile culture. In these institutions, between 49% and 65% of the patients had previous biliary stenting. A difference in antibiotic administration during BD was found, with two institutions giving drugs to all patients and the last one to only 28.6% of them. Similar microbiologic findings were observed, with as high as a 98.8% positive culture rate in the BD group compared with 10.5% in the NBD group and a two-fold increase in incision infection in the first group (12.3% versus 4.5%). An interesting finding was the different prevalence of bacteria among centers, with the bacteria found mostly being E. faecalis, Klebsiella pneumoniae, E. coli, and Enterobacter spp. Streptococcus pneumoniae is the best example, with 47% isolated in culture from one institution compared with 4.5% at another institution [9]. This suggests that the bile microbiome is dependent on the institution epidemiology and strongly endorsed our desire to characterize the local microbiome. Many studies confirmed the increase of incision infection, but to our knowledge, no increase in complications graded ≥3 according to Clavien-Dindo was reported [16,17].
Antibiotic use: When, how long, and which one?
Our study was not designed or powered to study appropriate antibiotic use. Therefore, we decided to review current literature to address this issue.
There exists great heterogeneity in regard to antibiotic use during BD, surgery prophylaxis, and post-operative pre-emptive care. The issue of whether there is a need for specific antibiotic prophylaxis for patients undergoing BD is addressed by several studies, which suggest that it should include anti-enterococcal coverage [18,19]. However, this remains a matter of controversy [20].
Another question is the length of pre-emptive antibiotic therapy after skin closure. Conventional antibiotic prophylaxis should be discontinued within 24 hours, with recent guidelines recommending its stoppage immediately after skin closure [21]. During duodenopancreatectomy, the bile duct as well as various intestinal compartments are opened, causing them to be at high risk of being contaminated. The appropriate duration of antibiotic prophylaxis or therapy has been studied by Sourrouille et al., who compared patients at high risk of bacteriobilia receiving five days of pre-emptive antibiotic treatment with patients with a low risk of bacteriobilia receiving conventional prophylaxis, all undergoing duodenopancreatectomy [22]. Those investigators found fewer infectious complications in the longer antibiotic use group, which was explained mainly by a diminution of urinary tract infection, pulmonary infection, and bacteremia but without impact on the incidence of incision infection. Mohammed et al. compared conventional antibiotic prophylaxis with 10 days of antibiotic therapy in sequential groups of patients undergoing duodenopancreatectomy and showed a lower post-operative site infection rate in the prolonged therapy group [23]. Immediate intra-operative bile Gram staining, such as described in the study by Augenstein et al. [24], might be of use to evaluate rapidly the presence of bacteriobilia and maintain antibiotic treatment until final culture identification and antibiograms are available. To guide this otherwise empiric treatment, bile culture might be obtained during retrograde cholangiopancreatography. However, the findings might not be representative of further colonization. This should be the subject of further studies.
Despite the lack of increase in major complications, the specific microbiome of patients having BD should be kept in mind when considering antibiotic prophylaxis. Prophylaxis regimens differ among institutions, but first- and second-generation cephalosporins, or other beta-lactam agents, are most frequently suggested. High resistance rates to classical antibiotic prophylaxis during duodenopancreatectomy have been reported, with 53%–72% of patients undergoing major surgery receiving inadequate prophylaxis [4,9]. In this context, recent broad-spectrum antibiotic strategies have been tested, such as a recent comparison by Tanaka et al. of a control group receiving cefmetazole and an interventional group receiving piperacillin/tazobactam combined with vancomycin up to post-operative day 1. Fewer surgical site infections occurred in the latter group, as well as less necessity for and duration of further antibiotic therapy, but the rates of infection remained high (50% in the conventional group, 25% in the broad-spectrum drug group) [25]. De Pastena et al. described a strong correlation in multi–drug-resistant (carbapenem and vancomycin resistant, extended-spectrum β-lactamase producing) bacteria between bile culture and rectal swabs obtained two to three weeks prior to surgery [26]. This non-invasive evaluation allowed detection of highly resistant bacteria prior to surgery.
Study limitations
Several limitations of this study warrant attention. The first limitation is the absence of randomization and the potential selection bias inherent in retrospective studies. Another limitation is the small sample, which did not permit adequate analysis of complications, antibiotic use, or resistance and drug use because of lack of power. The higher prevalence of malignant disease in the patients having BD suggests more severe or obstructive disease in this group.
Conclusions
Pre-operative BD is a widely used procedure that induces significant microbiome shifts. Our study confirms previous findings suggesting a switch from E. coli toward Enterococcus spp., as well as colonization by C. albicans. At our center, conventional antibiotic prophylaxis consisted of a second-generation cephalosporin (cefuroxime) coupled with metronidazole, which does not provide coverage of these micro-organisms. Antibiotic prophylaxis remains a challenge concerning drug choice and duration. Therefore, we propose that recent antibiotic use be documented, with special attention to prophylaxis received during BD. Intra-operative bile samples should be obtained systematically to document the local microbiome and guide any post-operative antibiotic therapy.
Footnotes
Acknowledgments
We thank Fabienne Muster for her work in medical records data acquisition. We thank the colleagues from the Clinical Microbiology Laboratory for technical assistance.
Author Disclosure Statement
The authors declare that they have no competing interests.