
Abstract
Background:
The grading systems for intra-abdominal sepsis (IAS) are not employed commonly in clinical practice because they are too complicated or too specific. We propose to grade IAS with a simple grading system: the TNM system, which is an acronym borrowed from cancer staging, where T indicates Temperature, N indicates Neutrophils, and M indicates Multiple organ failure (MOF). The aim of this prospective observational study is to assess the predictive value of the TNM score on deaths of patients with complicated IAS.
Patients and Methods:
We considered 147 patients with complicated IAS. Three classes of attribute were chosen: Temperature (T), Neutrophil count (N), and MOF (M). After defining the categories T (T0–T4), N (N0–N3), and M (M0–M2), they were grouped in stages (0–IV). We analyzed specific variables for their possible relation to death: Age, gender, blood transfusion, causes of IAS, T, N, pre-operative organ failure, immunocompromised status, stage 0, I, II, III, and IV. Odds ratios were calculated in a uni-variable and multi-variable analysis.
Results:
This was the distribution in classes, based on TNM stages: One patient was in stage 0; 15 patients in stage I; 47 patients in stage II; 56 patients in stage III; 28 patients in stage IV. Death occurred in 45 (30.6%) patients. The N, pre-operative organ failure, immunocompromised status, stage III–IV were potential predictors of post-operative death in uni-variable analysis. Only pre-operative organ failure and stage IV were significant independent predictors of post-operative death in multi-variable analysis.
Conclusions:
The TNM classification is an easy system that could be considered to define the death risk of patients with IAS and to compare patients with sepsis.
Intra-abdominal sepsis (IAS) is defined as infection of any intra-abdominal organ and can be classified as uncomplicated or complicated. We refer to uncomplicated IAS if infection is confined to a single organ without disruption of the viscus (i.e., acute cholecystitis). Complicated IAS develops when infection spreads from the affected organ and involves the peritoneal cavity (i.e., perforated peptic ulcer) [1–3]. After the infection spreads into the peritoneal cavity, it can form an abscess or it could cause generalized peritonitis [4–7]. Intra-abdominal sepsis has a wide spectrum of clinical manifestations and possible outcomes. Thus, grading the severity of an IAS at the moment of diagnosis represents a clinical necessity.
The analysis and definition of prognostic factors, combined with patient characteristics and treatments, led to several grading systems [8–18]. Some of them are complicated because they combine many different clinical variables. The Acute Physiology And Chronic Health Evaluation (APACHE score) was formulated in 1981 [8] and combines 12 different physiologic variables with patient age and comorbidities (APACHE II) [8]. The APACHE III score [19] is useful to have a detailed description of disease severity, but it is also complex and laborious. Other grading systems, such as the Mannheim Peritonitis Index (MPI) [14] or Ranson criteria [15], are useful and usable only in some secondary peritonitis (MPI in colonic perforation, Ranson criteria in acute pancreatitis).
At present, the grading systems are not employed commonly in clinical practice, although they seem to give precise clinical indications, because some of them are too complicated (APACHE II and III) and others are too specific (MPI and Ranson criteria).
We propose to grade the severity of IAS with a simple grading system: TNM system, which is an acronym borrowed from cancer staging, where T indicates Temperature, N indicates Neutrophil count, and M indicates Multiple organ failure (MOF).
The aim of this prospective observational study is to assess the predictive value of the TNM score, determined on the day of diagnosis/admission, on deaths of patients with complicated IAS.
Patients and Methods
The TNM system was developed based on a study of 147 patients with complicated IAS who were treated at our institution from April 2012 to May 2018. Patients younger than 18 years, with pancreatitis, or with primary peritonitis were excluded from the study. Pre-operative evaluation of the patients included clinical examination, blood tests, abdominal and chest radiography, abdominal ultrasonography, and computed tomography (CT).
Before any surgical procedure, all patients benefited from a period of resuscitation and restoration of intra-vascular volume. If hypotension or a lactate level ≥4 mmol/L was present, a rapid infusion of crystalloid was administered at a dose of 30 mL/kg. If hypotension persisted during or after resuscitation, a vasopressor was administered (dopamine) to maintain mean arterial pressure (MAP) ≥65 mm Hg. Before antibiotic administration, cultures of blood were performed. Antibiotic therapy included gram-negative as well as anaerobic coverage (ciprofloxacin 200 mg
In all patients, the infection (localized or generalized peritonitis) was confirmed by examination during the surgical procedure. The most common origin of infection was appendix (n = 61), followed by the stomach and duodenum (n = 34), colon (n = 27), small bowel (n = 10), biliary system (n = 8), and anastomotic leak (n = 7) (Table 1). We considered immunocompromised patients with human immunodeficiency virus/acquired immunodeficiency syndrome, with malignancies, those who received a transplant organ, or were receiving immunosuppressive therapy.
Complicated Intra-Abdominal Sepsis
The data were collected twice for each patient, verified, and stored in an electronic database. Consequently, an exhaustive list was compiled with clinical characteristic and laboratory evidence of the septic state, and three classes of attribute were defined to grade appropriately the severity of sepsis. The chosen classes were T, N, and M. For the assessment of organ failure, the definitions are listed in Table 2. The scoring within the classes is shown in Table 3. After defining the categories T, N, and M, these were grouped in stages (Table 3).
Definition of Organ Failure
Temperature-Neutrophil-Multiple Organ Failure Staging System for Intra-Abdominal Sepsis
Oral temperature.
Temperature should be recorded at least four times in 24 h
TNM = Temperature-Neutrophil-Multiple organ failure.
For the elaboration of this grading system, data were retrospectively analyzed from January 2001 to January 2012 for 461 patients with complicated IAS; afterward, a prospective observational clinical study was conducted. The TNM stage was collected at enrollment and then every day until death or discharge from the surgical department. The primary end point of the study was to evaluate the importance of the initial TNM stage in predicting death. The 30-day hospital mortality rate was assessed, and patients discharged alive before 30 days were contacted 30 days after admission to determine whether they were still alive.
Statistical analysis
The characteristics of the study sample were analyzed using descriptive statistics, and the discrete and nominal variables were expressed using frequencies and percentages. Uni-variable and multiple logistic regression were used to obtain predictors of death with associations reported as odds ratios (ORs) and 95% confidence intervals (CIs). The alive/deaths were chosen as dependent variables, and the explanatory variables were age, gender, blood transfusion, causes of intra-abdominal sepsis, degree of temperature elevation, N, pre-operative organ failure, immunocompromised status, stage 0, I, II, III, and IV.
Predictors that had a p value inferior to 0.05 in uni-variable models were considered in the multiple logistic regression models. Backward stepwise selection with the Akaike information criterion (AIC) was used to determine the predictive factors of death. Model discrimination was evaluated using the receiver operating characteristics (ROC) curve. This curve shows whether the model is able to distinguish between cases in the two groups. All the data were recorded electronically, and statistical analyses were performed using the Stata Statistical Software: Release 15/IC, College Station, TX: Stata Corp LP. All the tests were two-tailed, and p ≤ 0.05 was considered statistically significant.
Results
There were 147 consecutive patients included in the study, with a mean age of 60.9 years (range 18–86 years). The male:female ratio was 79:68, with no significative differences of ages between the sexes. Ninety-three patients (63.2%) were affected by localized peritonitis or abscesses while 54 (36.7%) had generalized peritonitis. The TNM staging assessed at diagnosis on the bases of clinical findings and laboratory values was: One patient at stage 0; 15 patients at stage I; 47 patients at stage II; 56 patients at stage III; 28 patients at stage IV (Table 4). Death occurred in 45 (30.6%) patients. The mean age of non-survivors was 61.7 (range 23–84) years while the mean age of survivors was 60.5 (range 18–86) years. Death was higher in the small and large bowel group—50% and 40.7%, respectively (Table 1).
Intra-Abdominal Sepsis: Stage Temperature-Neutrophil-Multiple Organ Failure on the Day of Diagnosis/Admission and Death
TNM = Temperature-Neutrophil-Multiple organ failure.
No patient with stage 0 or I died; death progressively increased (stage II: 6.3%; stage III: 25%) to 100% at a stage IV (Table 4).
Neutrophil count, pre-operative organ failure, immunocompromised status, stage III–IV were significant concerning post-operative death in uni-variable analysis (Table 5). Three of these potential predictors were included in the multi-variable analysis (Table 5), according to the stepwise selection based on AIC. Multi-variable analysis showed that pre-operative organ failure and stage IV independently influenced post-operative death (Table 5). A smaller AIC value indicated a better-fitting model, and discriminant ability was good (area under ROC curve = 0.9106, standard error = 0.0279) (Fig. 1).
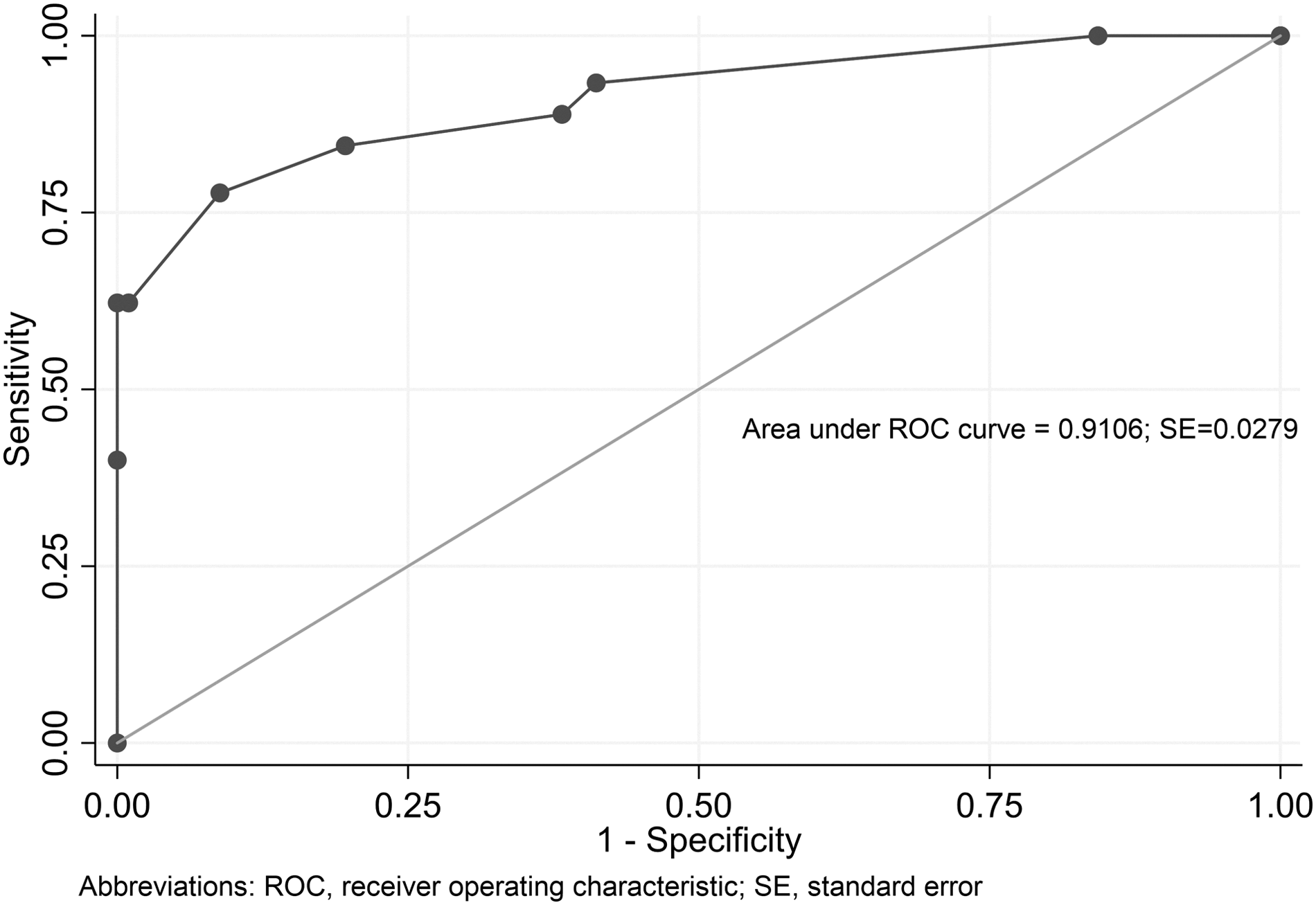
Area under receiver operating characteristics (ROC) curve for model fit. SE = standard error.
Factors Associated with Death (Uni-Variable and Multi-Variable Analysis)
reference category: oadjusted odds ratios for the other variables in the model* perforation of appendix, stomach, duodenum, and gallbladder, anastomotic leaks.
OR = odds ratio; CI = confidence interval; IAS = intra-abdominal sepsis; AIC = Akaike information criterion.
A significant difference was not demonstrable between the data prospectively collected and those retrospectively evaluated. A significant difference has not been demonstrated among data prospectively collected and retrospectively analyzed. The most common origin of infections was appendix (40.1%), followed by stomach and duodenum (20.3%), colon (18%), small bowel (7.6%), biliary system (7.4%), and anastomotic leak (6.5%). Death occurred in 144 (31.2%) patients. The mortality rate was 8.1%, 24.8%, and 100% at stages II, III, and IV, respectively. Death in the small and large bowel group was the highest—51.4% and 42.1%, respectively. In multi-variable analysis also immunocompromised status influenced post-operative death.
Discussion
In spite of improvement in intensive care medicine [20, 21] and the introduction of aggressive surgical techniques, the prognosis of complicated IAS remains scarce, particularly when MOF develops [22–30].
Several studies [31,32] have evaluated different therapeutic options for IAS. The transfer of therapeutic options from one institution to another and the comparison between studies about the same illness has been difficult, because of the impossibility to compare analogous populations and similar illnesses. Furthermore, death rates from IAS reported in the literature present a wide range (from 1% [33] and 6.7% [34] to 60% [22–28,35,36]) that is difficult to explain in the absence of patient stratification and in the absence of reliable comparison between different studies.
In the past, many scoring system have been developed [8–18]. The study by Bohnen et al. [37] supported a strong association between increasing APACHE II score and death. Billing et al. [38] showed that the accuracy of the MPI was comparable to or even better than APACHE II. In this regard, Bosscha et al. [17] affirmed that: “However the quality of prediction did not allow individual decision making or limitation of the therapy, because 41 per cent of patients with a score over 29 ultimately survived.” In their study [17], “combination of the APACHE II score and MPI was far superior to use of the two scores alone. All 14 patients with an APACHE II score of 20 or more and Mannheim score of 27 and above died.” Hence, they supported the thesis that “combination of the APACHE II score and MPI should therefore be the standard classification system for grading the severity of peritonitis and intra-abdominal sepsis.”
In our study, it seemed that the initial TNM stage might allow a high definition of patients related to their risk of death. We studied whether and how some prognostic factors influenced the mortality after complicated IAS. Neutrophil count, pre-operative organ failure, immunocompromised status, and stage III–IV were all predictive factors of death in uni-variable analysis. Otherwise, multi-variable analysis showed that only pre-operative organ failure and stage IV significantly influenced death.
All 28 patients at stage IV died. The high mortality rate (100%) for M2 patients (from MOF) was reported mainly for patients in the first phase of the study, when treatment was not so aggressive as in the last cases considered. The significant difference is that APACHE II score and MPI are too complicated or too specific, whereas our method shows a possible, simple way of grading a patient's with IAS. Moreover, APACHE II significance in peritonitis has been disputed because this grading system has difficulties in the assessment of surgical operations, although interventions might modify many physiological variables [39].
The need for intensive care is increasing worldwide [40]. In high-income countries (HICs), critically ill patients routinely are treated in intensive care units (ICU) by specialized physicians, nurses, and support staff. Sepsis is a major cause of ICU admission, also in resource-poor settings. A recent observational study on the worldwide spread of critical illness, although with limited representation from low and middle income countries (LMICs), showed that sepsis remains a major health problem globally, with significant association between death and national income [41].
The ICUs in LMICs face many challenges that could affect patient outcomes. Lack of human resources, adequate training, equipment, and infrastructures are all obstacles to safe and effective use of life-saving treatments in these settings [42]. The HIC ICU treatments may not be feasible in low-income settings, because of multiple barriers identified in a recent study, showing that implementation of current sepsis guidelines in Sub-Saharan Africa was limited by lack of facilities, equipment, and medications.
The TNM could facilitate evidence-based care of critically ill patients by standardizing interventions such as early appropriate antimicrobial treatment and rapid identification and management of cardiovascular, respiratory, and renal failure. Such scoring requires only clinical and routine laboratory data and provides a framework to optimize care and prognosis.
Furthermore, the TNM stage is dynamic, allowing observation and critical re-evaluation of the evolution of the clinical picture. Among complicated IAS, if we consider the definition of septic shock, severe sepsis, and sepsis [43], we could refer septic shock as stage IV, severe sepsis as stage III, moderate sepsis as stage II, and mild sepsis as stages I and 0 (Tables 3 and 4).
At this point, the grades attributed to the different characteristics of IAS are widely subjective, although their order, for a specific feature, is likely exact. Many remarks can be made concerning the individual scores. The range of temperature graded higher than T0 is beyond the normal value of 36.9 ± 0.47°C [44], and the score of temperature has been influenced by the findings of Altemeier et al. [45] and of Elebute and Stoner [12]. The range of N reflects the works of van Ruler et al. [46–50]. An attempt has been made to score MOF, despite the difficulty of getting a precise definition accepted universally. The rating of MOF was supported by data of Goris et al. [13] who in 1985 published the MOF score, grading the pulmonary, cardiovascular, hepatic, renal, nervous, hematologic, and gastrointestinal dysfunction on a three-point scale.
Our study, however, being a preliminary study, obviously has some limitations. The heterogeneous group of patients, the prolonged period of data collection, the small sample size, and the collection of data in a single center are the main ones, because these factors may influence the evaluation of the TNM. Moreover, it should also be considered that a long lead time between the onset of illness or the severe period of disease and then the evaluation of score may contribute to the performance of the TNM.
Therefore, to better evaluate the TNM classification in patients with IAS and in other situations (for example, thoracic sepsis, burns, etc.), large-scale multi-center clinical studies should follow. Our score needs further validation before being used in clinical practice.
Conclusions
Even though there is a need for additional studies, we have been stimulated to share these preliminary results about the development of the TNM classification, which would be useful to grade IAS, define patients, assess their risk of death, and finally allow comparisons of patients with sepsis to make the studies performed in different centers objective.
Moreover, the TNM system has the advantage of being very easy to use, compared with other grading systems.
Footnotes
Author Disclosure Statement
No competing financial interests exist.