
Abstract
Background:
We performed a systematic review of the literature on antibiotic prophylaxis practices in open reduction, and internal fixation of, facial fracture(s) (ORIFfx). We hypothesized that prolonged antibiotic prophylaxis (PAP) would not decrease the rate of surgical site infections (SSIs).
Methods:
We performed a systematic review of four databases: PubMed, CENTRAL, EMBase, and Web of Science, from inception through January 15, 2017. Three independent reviewers extracted fracture location (orbital, mid-face, mandible), antibiotic use, SSI incidence, and time from injury to surgery. Mantel-Haenszel and generalized estimating equations were carried out independently for each fracture zone.
Results:
Of the 587 articles identified, 54 underwent full-text review, yielding 27 studies that met our inclusion criteria. Of these, 16 studies (n = 2,316 patients) provided data for mandible fractures, four studies (n = 439) for mid-face fractures, and six studies (n = 377) for orbital fractures. Pooled analysis of each fracture type's SSI rate showed no statistically significant association with the odds ratio (OR) of developing an SSI. For mandible fractures treated with ORIFfx, the OR for an SSI after 24–72 hours of prophylaxis relative to <24 hours was 0.85 (95% confidence interval [CI] 0.62–1.17), whereas for >72 hours compared with <24 hours, the OR was 1.42 (95% CI) 0.96–2.11). For mid-face fractures, there was no improvement in SSI rate from PAP (OR 1.05; 95% CI 0.20–5.63).
Conclusions:
We did not demonstrate a lower rate of SSI associated with PAP for any ORIFfx repair. Post-operative antibiotics for >72 hours paradoxically may increase the SSI risk after mandible fracture repairs.
Facial fractures account for more than 260,000 emergency department visits each year in the United States [1,2]. Nearly 40% of these injuries require open surgical management [3]. Avoidance of surgical site infections (SSIs), especially in the setting of implanted hardware, is crucial; and there is a broad consensus that the administration of prophylactic antibiotics post-operatively helps reduce this risk [4–6]. However, the role of antibiotic prophylaxis (PAP) for more than 24 hours in the operative management of facial fractures is controversial. Two studies, published more than 30 years ago, encouraged widespread use of PAP in facial fractures [4,5]. However, contemporary data suggest that PAP with open reduction and internal fixation of facial fractures (ORIFfx) likely is unnecessary [6–14]. Despite these findings, a review from 2015 included a survey of US plastic surgeons that found that 75% employ PAP routinely for >24 hours, and the majority of respondents reported continuing antibiotic prophylaxis for at least one week [15]. This practice is potentially problematic, as the emergence of multi-drug-resistant organisms and antibiotic-linked complications (e.g., Clostridioldes difficile colitis) create substantive healthcare issues. Furthermore, these complications are associated with greater morbidity, length of stay, deaths, and healthcare costs [16–19].
Habib et al. performed a systematic review and meta-analysis of 13 studies on post-operative antibiotic prophylaxis for facial fractures [20] and demonstrated that there was no discernible difference in the SSI rate between those individuals who received PAP (>24 hours) and individuals who received <24 hours of antibiotic prophylaxis. Although the study was well designed, it did not differentiate between the duration of antibiotic prophylaxis behind a binary point around 24 hours, and their analysis by anatomic fracture location was limited.
Our understanding of infection and the limitations of antibiotic prophylaxis continues to improve, and shorter courses of antibiotics are being implemented in many diseases [21–23]. The mounting evidence against PAP for facial fractures prompted this systematic review and meta-analysis focusing on different durations of prophylaxis. To avoid further dilution of already heterogeneous data and isolate fracture patterns with likely disparate infection rates, we elected to review the three major zones (i.e., orbital, mid-face, mandible) of facial fractures discretely (i.e., analysis of mandibular fractures apart from orbital and mid-face fractures). We hypothesized that the use of PAP after ORIFfx would not decrease the rate of post-operative SSIs for any anatomic fracture zone.
Methods
Search strategy
A systematic search of PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), EMBase, and Web of Science was performed to retrieve studies published from the inception of the databases to January 15, 2017. The Preferred Reported Items for Systematic-Reviews and Meta-Analyses (PRISMA) guidelines were followed where possible [24]. We included randomized controlled trials (RCTs) and prospective, observational, retrospective, cohort, and case-control studies focused on prophylactic antibiotic use in pre- and post-operative patients with acute facial fractures. We developed the optimal search strategy in PubMed and applied filters to restrict the final search results to adult participants (Supplement 1). The search strategy was modified as necessary for use in the Cochrane Library (Wiley InterScience, John Wiley and Sons, Inc., Hoboken NJ), EMBase (Elsevier, Inc., Atlanta, GA), and Web of Science (Clarivate Analytics, Philadelphia, PA) databases.
Clinicaltrials.gov also was searched to identify any ongoing or recently completed trials. Additionally, we contacted principal investigators of clinical trials that we identified in Clinicaltrials.gov for potential unpublished studies, but no additional studies were obtained. All search results were managed in EndNote v. 8 (Clarivate Analytics), wherein duplicate studies were removed.
Inclusion/exclusion criteria
The search was restricted to peer-reviewed manuscripts of original research published within the time-frame of our search. For inclusion in this meta-analysis, the study participants must have undergone an operative intervention for facial fracture, with a reported post-operative SSI rate, of the mandible, orbit, and mid-face (including fractures of the zygomatic arch of the temporal bone and maxillary fractures except for the infraorbital rim, whether or not of the LeFort type). Parietal, temporal (except for the zygomatic arch), or frontal bone skull fractures were excluded. Each study also had to provide a duration of antibiotic administration and clear identification of which study participants received a particular post-operative antibiotic course. We placed no restrictions on the type or timing of operative intervention performed or the type or class of antibiotic administered. Facial fractures of non-traumatic origin or from an existing condition were not included. Studies that did not identify clearly the anatomic fracture location were included in a subgroup of “mixed” fracture patients. Studies performed in pediatric patients (≤18 years old) were excluded. Systematic reviews were not considered for inclusion, nor were opinion articles or case reports.
Classification of studies
Each study was classified according to the National Health and Medical Research Council levels of evidence [25]. A study was included if it compared an intervention with a control group, irrespective of randomization (Level II and III studies). In order to maximize the number of studies selected for analysis, studies were included if they followed a clinical effectiveness design wherein outcomes were compared before and after the institution of an intervention (Level III and IV studies).
Study selection
Titles and abstracts were screened independently by three reviewers for eligibility, with each reviewer assessing two-thirds of the identified candidate studies. Any discrepancies among reviewers were mediated by a senior reviewer (JN). Included studies then underwent full-text review to confirm that sufficient data were present and that the inclusion criteria were met. A flow chart of the study selection process can be seen in Fig. 1.
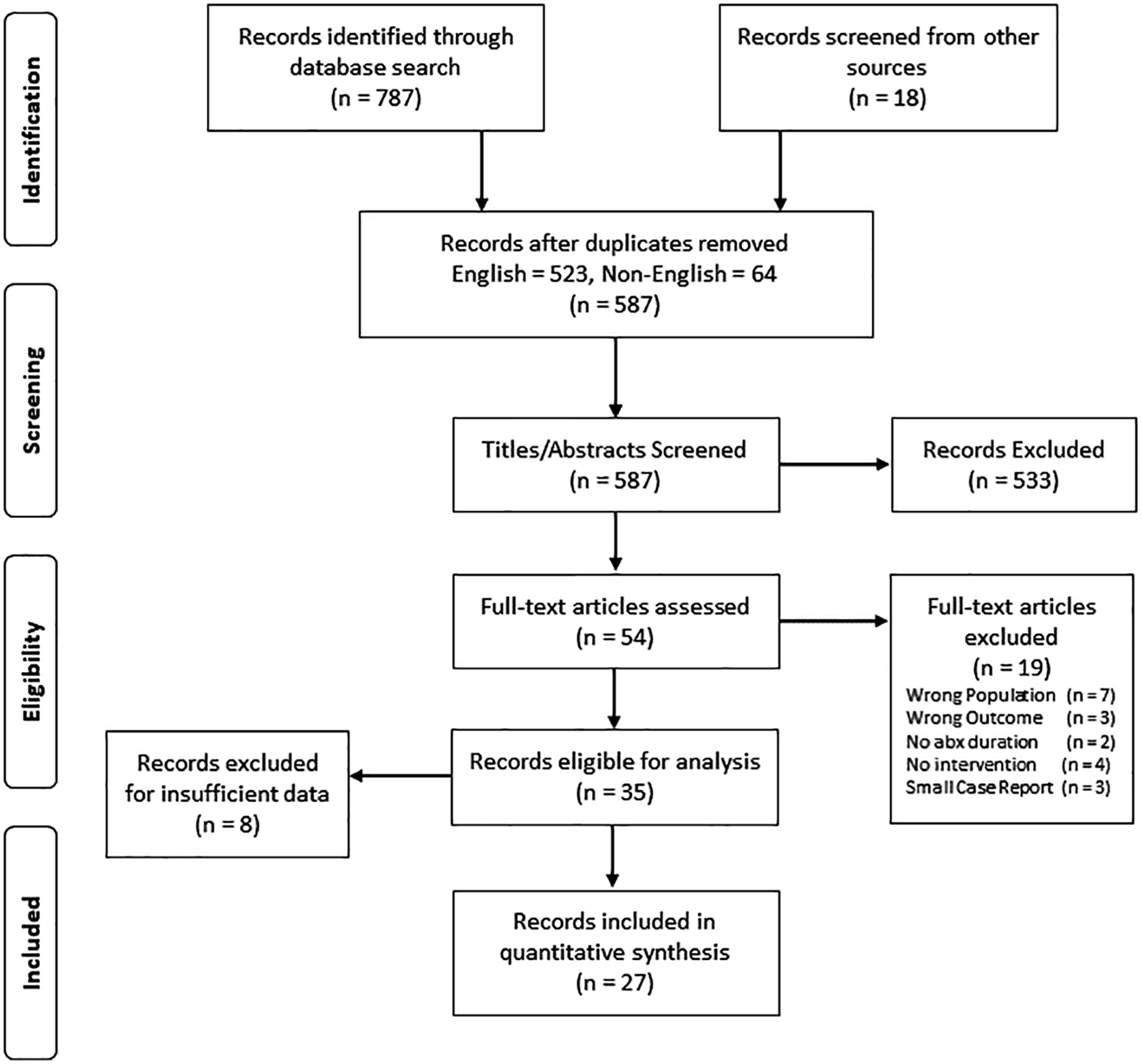
Overview of literature search and review for manuscripts included in meta-analysis.
Data extraction
Extracted data were: (1) Publication year; (2) study design; (3) number of years studied; (4) age range of study subjects; (5) number of study subjects; (6) follow-up interval; (7) types of fractures; (8) antibiotic duration; (9) antibiotic used; and (10) time from injury to intervention. For each study, the relevant antibiotics administered were classified into three general categories, with all patients receiving pre-operative antibiotics: Peri-operative (<24 hours post-operatively), post-operative (24–72 hours post-operatively), and extended post-operative (>72 hours after surgery).
Risk of bias/study quality assessment
Because we included RCTs as well as non-randomized prospective and retrospective studies, we employed the modified Downs and Black checklist [26] to determine the risk of bias. This form was completed for each of the included studies by an independent reviewer not involved in the initial data collection (Supplement 2). It focuses on several domains of study quality, including reporting of data, external validity, internal validity (bias and confounding/selection bias), and power. Study quality was then reported (Table 1) on the basis of the score as a categorical rank: Excellent (26–28 points), good (20–25), fair (15–19), and poor (≤14).
Summary of Studies Used in Quantitative Meta-Analysis
Studies used in both MH and GEE analysis.
Study quality based on modified Downs and Black checklist score [26]: excellent (26–28); good (20–25); fair (15–19); and poor (≤14) points.
Extended = antibiotics discontinued >72 h from surgery); IM = intramuscularly; NA = not applicable; N/S = not specified; Peri-op = antibiotics discontinued <24 h from surgery), Post-op = antibiotics discontinued 24–72 h post-operatively); RCT = randomized controlled trial.
Meta-analysis and data synthesis
To present meaningfully the association between the development of post-operative SSI and the prophylactic use of antibiotics, the focus of the data synthesis was an estimate of the odds ratio (OR). Given the great deal of disparity in how findings were presented in different studies, two approaches were taken in the quantitative synthesis of the data. Studies that provided clear information on SSI rates for two or more of the general antibiotic treatment groups were tabulated and analyzed using the Mantel-Haenszel (MH) approach [27]. A number of studies assessed the rate of SSI for only a single prophylactic regimen; in an effort to utilize as much as possible of the available literature, we employed generalized estimating equations (GEEs) to arrive at marginal (population-wide) estimates of the odds of developing an SSI given a particular prophylactic regimen. Exchangeable correlation structure was assumed for the models, and a robust variance estimator was used.
Results
We identified 787 abstracts via the database search, and, after exclusion of duplicates, there were 587 articles that underwent screening. On full-text review, 35 articles met the criteria for qualitative synthesis, although eight could not be included in the final quantitative analysis because of insufficient data (Fig. 1). In the end, 11 articles had sufficient data to be included in the MH meta-analysis (Nos. 4, 12, 13, 28–35); 20 articles (including most of the MH group) were used in the GEE approach (Nos. 4, 8, 11, 12, 28–31, 33–44), and five studies were used only for pooled data regarding the incidence of SSI (Nos. 14, 45–48) (Table 1).
During the final analysis, 16 studies contributed to the data on SSI and antibiotic use in patients with mandibular fractures (Nos. 4, 11, 12, 28–31, 33–35, 37, 38, 40, 42–44), four to mid-face fractures (Nos. 13, 32, 44, 46), six to orbital fractures (Nos. 14, 44–48), and four to mixed fractures (Nos. 8, 36, 39, 41). Pooled analysis was carried out separately for each fracture type whenever enough information was available. Results per fracture type are presented in more detail in the sections below.
Mandibular fractures: ORIF with or without maxillomandibular fixation (MMF)
Sixteen studies (Nos. 4, 11, 12, 28–31, 33–35, 37, 38, 40, 42–44) were included in our analysis of post-operative infection after ORIF was performed for mandibular fractures. Three studies compared SSI rates for patients treated with peri-operative antibiotics only versus post-operative antibiotics (Nos. 29, 30, 33). Eight studies compared SSI rates between peri-operative antibiotics only and extended antibiotic prophylaxis (Nos. 4, 11, 28–31, 35, 43). Four studies compared patients who received post-operative antibiotics with those who received extended antibiotic prophylaxis (Nos. 12, 29, 30, 34). Five studies had information only on a single regimen (Nos. 37, 38, 40, 42, 44).
Overall, the results of the MH analysis showed no significant association between the odds of a post-operative SSI and any of the antibiotic regimens examined. Specifically, we found no significant association between the odds of developing an SSI and the treatment regimen administered when comparisons were made between peri-operative and post-operative (OR 0.84; 95% confidence interval [CI] 0.43–1.61) (Fig. 2), or post-operative and extended prophylaxis (OR 1.17; 95% CI 0.70–1.96) (Fig. 3).
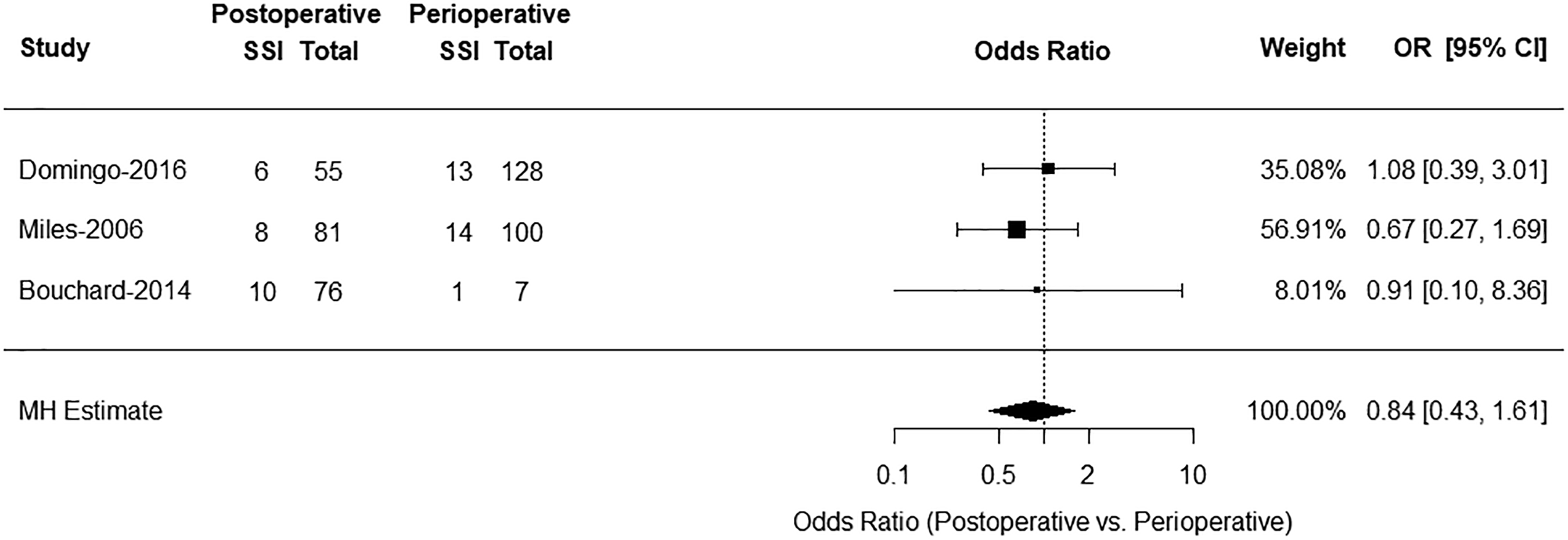
Forest plot of Mantel-Hanszel estimates of odds ratios of post-operative surgical site infections among patients in post-operative antibiotic group (antibiotics discontinued 24–72 h post-operatively) relative to the peri-operative group (antibiotics discontinued <24 h from surgery).
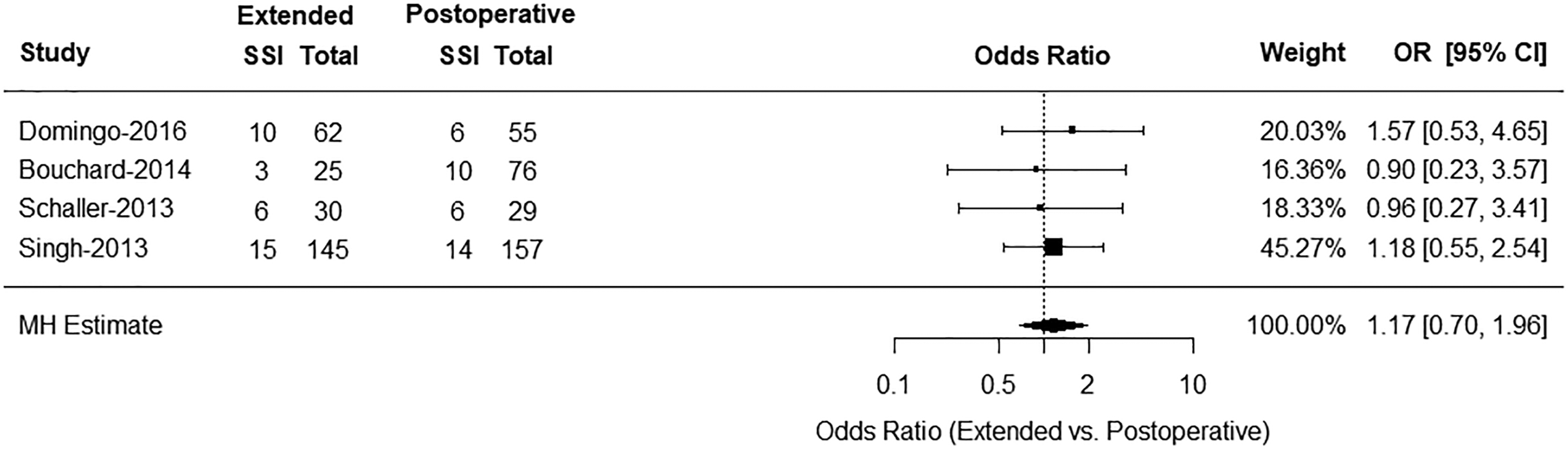
Forest plot of Mantel-Hanszel estimates of odds ratios of post-operative surgical site infections among patients in extended antibiotic group (antibiotics continued >72 h post-operatively) relative to post-operative antibiotic group (antibiotics discontinued 24–72 h post-operatively).
However, there was some heterogeneity among estimates in the peri-operative only and extended antibiotic groups. Specifically, the study performed by Zallen et al. appears to have an impact on the pooled estimates [4]. To capture the effect size of that particular study, MH estimates were summarized with (OR 1.42; 95% CI 0.96–2.11) (Fig. 4) and without (OR 1.63; 95% CI 1.0–82.46) (Fig. 5) this study. Exclusion of this study showed a statistically significant increase in the risk of SSI in patients who received extended antibiotic prophylaxis compared with those who received peri-operative antibiotics alone. The difference in SSI rates between the pooled studies is demonstrated further in a L'Abbe plot (Fig. 6), in which the SSI rates of the two treatment regimens are plotted against one another for each study.
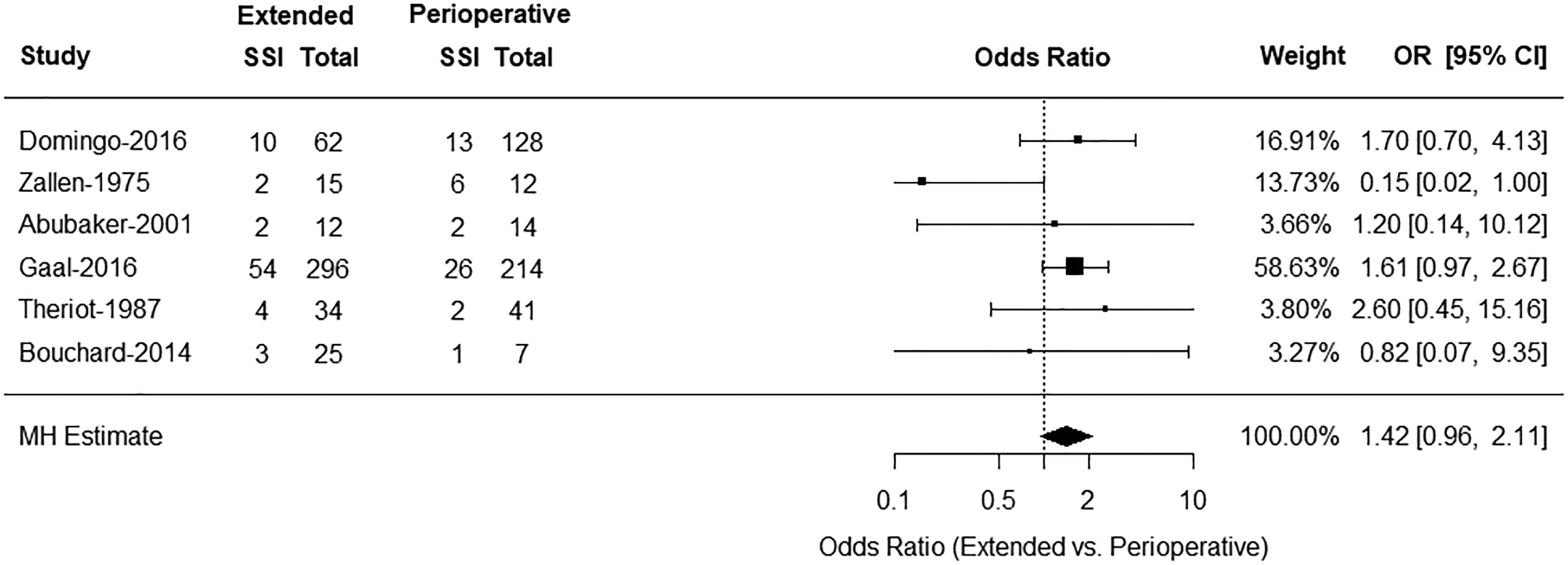
Forest plot of Mantel-Hanszel estimates of odds ratio of post-operative surgical site infections among patients in extended antibiotic group (antibiotics continued >72 h post-operatively) relative to peri-operative antibiotic group (antibiotics discontinued <24 h from surgery).
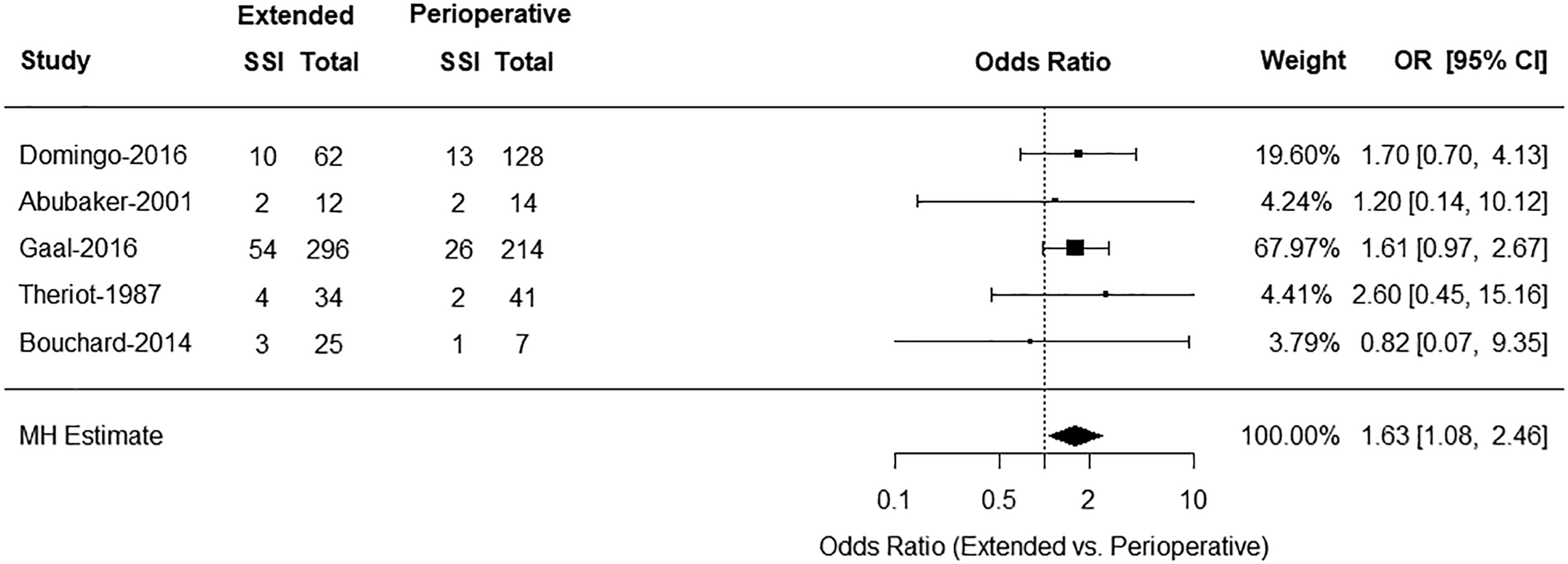
Forest plot of Mantel-Hanszel estimates of odds ratio of post-operative surgical site infections among patients in extended antibiotic group (antibiotics continued >72 h post-operatively) relative to peri-operative antibiotic group (antibiotics discontinued <24 h from surgery) with article by Zallen et al. removed from analysis.
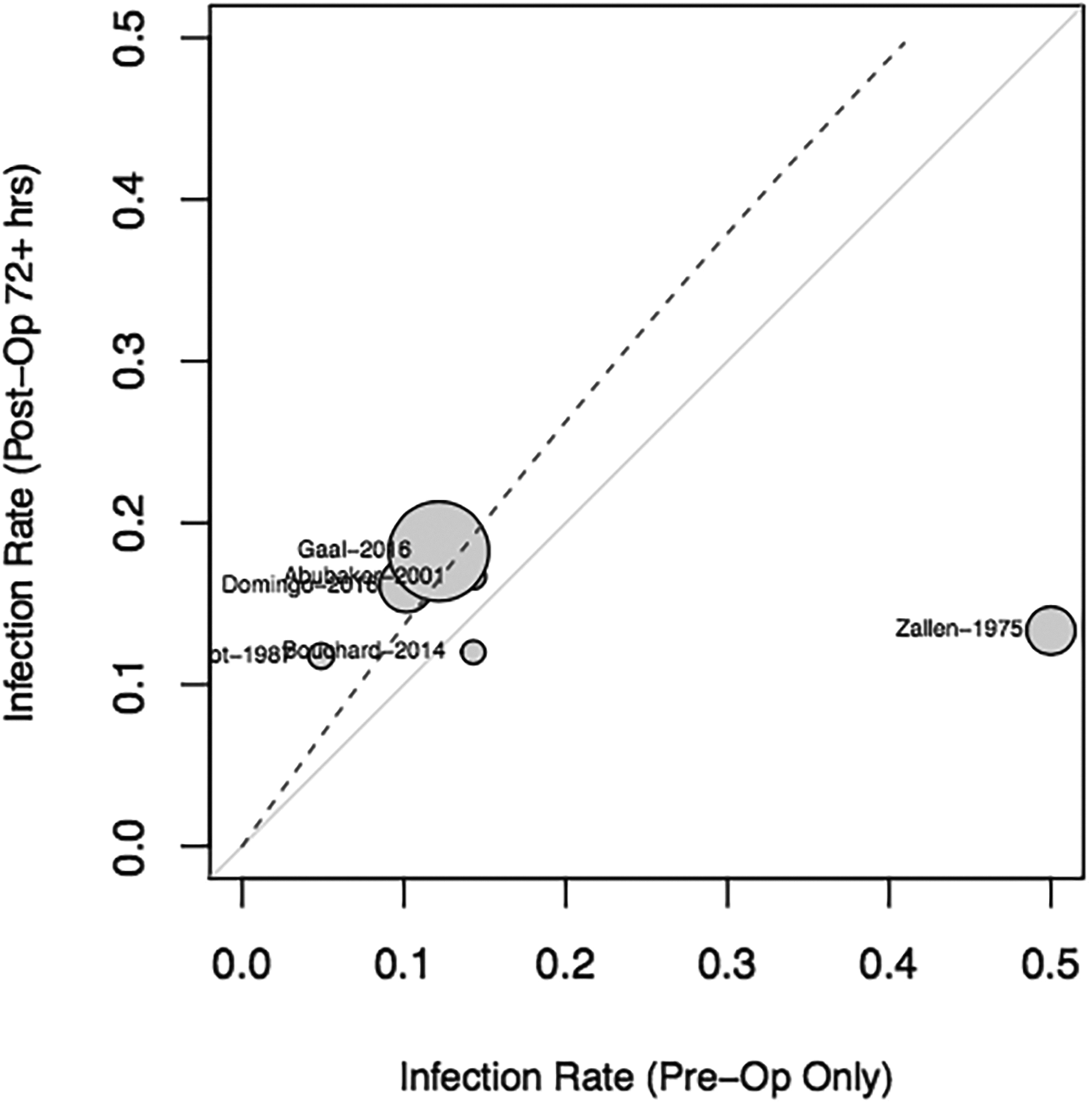
L'Abbe plot for extended antibiotic group (antibiotics continued >72 h post-operatively) versus peri-operative antibiotic group (antibiotics discontinued <24 h from surgery). The points show surgical site infection (SSI) rates in the two groups. Solid diagonal line represents points at which studies do not differ in rate of SSI in the two groups. Points falling below this line represent studies where rate was lower in extended treatment group. Similarly, points above this line represent studies where rate was higher in extended group. Size of points is proportional to study size.
All 16 studies (4, 11, 12, 28–31, 33–35, 37, 38, 40, 42–44) were then used for further analysis using GEE estimates (Fig. 7). Similar to the MH analysis, there was no statistically significant association between the risk of developing SSI and the prophylactic antibiotic regimen.

Summary of generalized estimating equation (GEE) estimates of odds ratios of developing post-operative surgical site infection according to antibiotic treatment group in patients with mandibular fractures undergoing open reduction and internal fixation. Note that all confidence intervals contain the value 1.
Mid-face fractures
Two studies had sufficient data to include in an MH analysis comparing peri-operative antibiotics alone with extended antibiotic prophylaxis among those with mid-face fractures (Fig. 8) [13,32]. We found no difference in the odds of developing a post-operative SSI in the two groups (OR 1.05; 95% CI 0.20–5.63).

Forest plot of Mantel-Hanszel (MH) estimates of odds ratios (OR) of post-operative surgical site infection among patients in extended antibiotic group (antibiotics continued >72 h post-operatively) relative to peri-operative antibiotic group (antibiotics discontinued <24 h from surgery) in patients with mid-face fractures.
Among the 439 patients in this pooled group, only seven (1.6%) developed a post-operative SSI. This low incidence precludes further analysis with the GEE model.
Orbital Fractures
Six studies contributed to the incidence of post-operative SSIs in patients with orbital fractures [14,44–48]. Similar to the patients with mid-face fractures, the incidence of SSI was low (1.77%). Among 452 patients, only eight had a post-operative SSI—none of whom was in the peri-operative group. Unfortunately, insufficient comparisons were available across studies on orbital bone fractures to allow MH or GEE analysis.
Mixed fractures
We identified four studies in which the categorization of facial fractures was not well documented and thus could not be included in any of the three anatomic fracture zones [8,36,39,41]. These studies represent a heterogeneous group of 703 patients with an overall post-operative SSI incidence of 6.26%. In order to avoid bias by inclusion in a single group, these studies were analyzed separately as a “mixed” group. Unfortunately, neither GEE estimates nor MH analysis could be performed reliably, as the available data for the “mixed” treatment group were scant.
Discussion
After a thorough systematic review of the current literature, our quantitative meta-analysis demonstrated no difference in the risk of SSI for most anatomic facial fracture locations, regardless of the antibiotic prophylaxis regimen that was administered. This suggests that PAP courses likely are unnecessary. Unfortunately, the reporting of adverse antibiotic events among the examined studies was nearly absent, so it cannot be concluded directly whether PAP is harmful.
Habib et al. published recently a similar meta-analysis on the risk of SSI associated with the use of post-operative antibiotic regimens [20], which included approximately 1,200 patients across 13 studies. Whereas that study and ours came to the same principal conclusion—that PAP for facial fractures is unnecessary—the focus of the two analyses is different. Habib et al. defined post-operative antibiotics as anything >24 hours, whereas our meta-analysis examined multiple regimens of post-operative antibiotics and demonstrated that both post-operative (24–72 hours) and extended (>72 hours) courses of post-operative antibiotics failed to reduce the rate of SSI.
Other major differences between the two analyses dealt with inclusion criteria and methods of quantitative analysis. Broader inclusion criteria and the use of two quantitative analyses (MH and GEE) allowed us to comment specifically on both the mandibular and mid-face fracture zones, for both of which no overall benefit was shown. In addition, we showed a greater risk of SSI with PAP in mandibular fractures. It is possible that the broader inclusion criteria employed for quantitative analysis introduced some additional bias, but if this finding is corroborated, it will be the first evidence that PAP actually may be harmful to some patients.
As expected, the findings of this study are consistent with five RCTs addressing the utility of post-operative antibiotic prophylaxis for ORIFfx (12–14,28,33). Despite accumulating evidence, a large questionnaire study found that the majority of facial surgeons in the Unites States use PAP for their patients, with 64%–70% choosing courses longer than 24 hours (15,49,50). This practice is not without risk, as it may expose patients needlessly to adverse reactions to antimicrobial agents, opportunistic infections such as C. difficile colitis, and the emergence of resistant bacterial strains (51–53). We are unable to comment directly on adverse antibiotic-related events; this is attributable primarily to scant reporting in the surveyed studies, and the true risk to patients is unclear. We recommend that all future studies on this topic include adverse event reporting in their analyses. Additionally, PAP in the most common group of facial fracture patients—mandibular fractures undergoing ORIF—paradoxically may result in more post-operative SSIs when patients receive prolonged (>72 hours) antibiotic courses. It is possible that PAP selects resistant or more virulent organisms or that mandibular fractures in particular carry a higher bacterial burden if they are associated with an intra-oral laceration.
The duration of prophylaxis reported in the literature is heterogeneous. This led us to separate the treatment regimens into three groups that seemed to be employed most commonly: peri-operative only (<24 hours), post-operative (24–72 hours), and extended post-operative (>72 hours). This last group included a large range of antibiotic durations (five days to three weeks), which could affect the generalizability of the observations for this particular group. Regardless, we found no difference in SSIs after ORIFfx regardless of the strategy employed, with the possible exception of mandibular fractures.
Another limitation of the available data is the lack of consistent reporting on the type or class of antibiotic employed. Malanchuk et al. reported that for mandibular fractures, patients given a lincosamide antibiotic had a lower rate of SSI than those treated with beta-lactam drugs, cephalosporins specifically, or aminoglycosides [54]. Those investigators hypothesized that this difference was related to oral flora, in particular anaerobic species, which are not always susceptible to agents used typically for skin/soft tissue prophylaxis, where activity against aerobic gram-positive cocci is paramount. Additionally, there is a known attrition rate in follow-up studies with the often young male patients who engage in behavior that predisposes them to facial trauma [55]. Whereas well-designed RCTs, such as that of Miles et al. [33], make a point to address the large population of facial fracture patients who are “lost to follow-up,” the quality of post-operative follow-up is not well documented in most of the available literature. It is possible that this inadequacy skews the SSI incidence toward either over- or under-reporting, as patients who develop an SSI may be more likely to follow up or may choose to follow up at another institution.
Finally, there are many patient-specific parameters that we were unable to address because of inconsistent reporting across the literature. Factors such as tobacco use, diabetes mellitus, poor oral hygiene (especially dentition), substance abuse, and age have been linked to a higher risk of SSI after facial fractures [56,57]. Whereas these factors could confound the association between SSI and PAP, three prospective studies included in this analysis did control for patient factors and came to the same conclusion—PAP does not prevent SSI [12–14].
In conclusion, this systematic review found that antibiotic prophylaxis beyond 24 hours post-operatively was not associated with a lower incidence of SSIs, regardless of the location of the facial fracture. Extended antibiotic prophylaxis of patients with mandibular fractures undergoing ORIF actually was associated with a higher risk of SSI. We suggest that post-operative antibiotics in patients with facial fractures should be limited to 24 hours or less. Unfortunately, the data are too heterogenous to offer a definitive statement on antibiotic selection. The development and implementation of practice guidelines regarding antibiotic stewardship in surgical facial fracture management is needed.
Author Disclosure Statement
None of the authors of this manuscript has significant financial disclosures to make related to this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.