
Abstract
Background:
Prolonged surgical antimicrobial prophylaxis (SAP) to prevent surgical site infection (SSI) is generally discouraged after completion of surgery. However, little is known about the pattern of peri-operative antibiotic use in resource-limited settings. We aimed to describe its use at a typical government hospital in Uganda.
Methods:
A study was originally conducted in a rural Ugandan regional referral and teaching hospital in 2014 and 2015 to improve hand hygiene practice and measure its impact on health-care–associated infections including SSI (WardGel study). This is a secondary analysis of the data from the WardGel study to assess the frequency of peri-operative antibiotic use among surgical patients.
Results:
Of 3,627 patients enrolled into the original study, 960 (26.5%) underwent surgery at the hospital and 907 patients (94.5%) received antibiotic agents during hospitalization. Of these, 880 patients (97.0%, of 907 patients) received antibiotic agents on the day of surgery. A combination of ceftriaxone and metronidazole was the most common regimen (609/907 patients, 67.1%). Thirty-six of 907 patients (4.0%) started and completed their antibiotic agents on the day of surgery. The mean length of antibiotic use during hospitalization was 3.5 days (standard deviation, 3.3). After adjusting for covariates, linear regression analysis showed an extra 1.9 days of antibiotic use post-operatively (95% confidence interval = 1.7–2.3). During the total 4,960 inpatient-days for those having surgery, there were 6,503 days of therapy (DOTs) of antibiotic agents and 1,649 antibiotic-free days (AFDs).
Conclusions:
Most patients received prolonged antibiotic therapy after surgery. Antimicrobial stewardship for SAP can play a major role in combating antimicrobial resistance in resource-limited settings.
Surgical site infection (SSI) is the most common health-care–associated infection (HAI) in low- and middle-income countries (LMICs) with the cumulative incidence ranging from 1.2 to 23.6 per 100 surgical procedures [1,2]. Although it is also one of the most common HAIs in high-income countries (HICs), the incidence of SSI is considered higher in LMICs than in HICs [1,3–5]. A recent study on surgical outcomes showed that post-operative death rates in Africa were twice the global average. Furthermore, one in 10 patients who developed an infectious complication (mostly SSIs) died after surgery in Africa [6]. Therefore, prevention of SSI would make a substantial contribution to reduction in the global burden of HAIs especially in LMICs, including Africa.
Surgical antibiotic prophylaxis (SAP) is an important strategy to prevent SSI [7–10]. In 2016, the World Health Organization (WHO) published a guideline on the prevention of SSI and made recommendations on SAP. This included the advice to avoid prolonged courses of SAP “after completion of the operation for the purpose of preventing SSI” [11]. Most other guidelines recommend discontinuing SAP within 24 hours after surgery or giving only a single dose of pre-operative SAP, except prolonged or specific surgical procedures such as cardiac surgery [8,9,12,13].
Antimicrobial resistance (AMR) has also been recognized as a public health threat at the global level [14]. In 2015, WHO published an AMR global action plan that included an objective to optimize the use of antimicrobial medicines. In the report, they noted that there was a paucity of data on human antibiotic use at the point of care, particularly from low-income countries [15].
Surgical antibiotic prophylaxis and AMR interact closely with each other: declining efficacy of SAP because of AMR could jeopardize safe surgical procedures whereas inappropriate, prolonged SAP could select for resistant micro-organisms [16,17]. A study in Sudan showed that SAP was often given inappropriately: all those who received SAP had extended antibiotic use, with an average of eight days whether they developed SSI or not [18]. However, such epidemiologic evidence of inappropriate antibiotic use related to SAP in LMICs is underreported in the literature. The aim of this study is to describe the culture and use of SAP at a typical government hospital in Uganda.
Patients and Methods
Study design and setting
The study was a quasi-experimental study conducted at Mbale Regional Referral Hospital (MRRH), a government teaching hospital in eastern Uganda between October 2014 and April 2015 (WardGel study) [19]. The details of the study have been published elsewhere [19], but in brief, the original study's aim was to assess the effect of the introduction of alcohol-based hand rub (ABHR) on the incidence of HAIs including SSI. The hospital has 12 wards with 550 beds, from which five wards were selected for the study across three departments: pediatric, obstetrics/gynecology (OB/GYN), and general surgery.
Although not all were qualified doctors, the researchers who collected the data in this study all had previous experience in the care of surgical patients and infections and had undergone training in the assessment of infection. In this study, they first checked the operation notes. If the notes recorded that the patient had undergone an operation, they examined the incision for any infection to determine its severity (class) before recording their findings on paper-based surveillance forms. The observations were conducted at least daily to capture the change in the patients' clinical status. The diagnosis of HAIs was according to the 2014 version of U.S. Centers for Disease Control and Prevention's National Healthcare Safety Network (CDC/NHSN) surveillance definitions of HAIs. Wound classes were defined according to the United States CDC definition as class 1 (clean), class 2 (clean-contaminated), class 3 (contaminated), and class 4 (dirty or infected) [20]. The efforts were made to ensure the data collected was accurate and consistent with the physicians' assessment by confirming with the hospital staff and physicians if needed.
For the purpose of this article, we focused on the patients hospitalized in the two surgical departments (OB/GYN and surgical departments) and excluded the pediatric department where no surgery was conducted. The patients' demographics, interventions, vital signs, clinical findings including wound class, antibiotic use, and outcomes were recorded in paper-based surveillance forms by research assistants.
Outcomes and statistical analysis
The main outcomes for this article were the length and type of peri-operative antibiotic use. Length of antibiotic use at patient level was calculated by counting each day any antibiotic was given to a patient as one day, regardless of antibiotic type, dose, and frequency. To measure accurately the prolonged use after surgery rather than antibiotic use before surgery, extra days of antibiotic use after surgery were calculated by counting each day that an antibiotic was given to a patient at least a day after surgery (that is, antibiotic use before or on day of surgery were not counted). Conversely, antibiotic-free days (AFDs) were also calculated by counting each day when no antibiotic agents were given to a patient during their hospitalization as one AFD [21]. To measure the extent of antibiotic exposure by antibiotic type, days of therapy (DOTs) were also calculated by counting each day an antibiotic was given to a patient as one DOT [21–23]. The difference between length of antibiotic use and DOTs is that DOTs consider multiple types of antibiotics given simultaneously, for example, if a patient receives ampicillin and gentamicin only for a day, one DOT for ampicillin and one DOT for gentamicin are counted separately. The use of urinary catheter or mechanical ventilation was counted as “yes” when they were used at any time during the hospitalization. The t-tests and χ2 were performed for continuous and categorical parameters in bivariable analyses, respectively. Linear regression analysis with backward selection and plausible causal interpretation was made to adjust length of antibiotic use for associated parameters. Statistical significance was defined as a p value of <0.05 and 95% confidence intervals (CIs) were reported when appropriate. R version 3.4.1 (The R Foundation, Vienna, Austria) was used for all statistical analysis.
Results
Of 3627 patients originally enrolled into the study, 960 patients who underwent surgical procedures during the study period were analyzed. In total, the observations from 960 patients over 4,960 inpatient days were analyzed for this article. Approximately three-quarters of the patients (714, 74.4%) were hospitalized in the OB/GYN department. Cesarean delivery was the most common surgical procedure (474 patients, 49.4%), followed by laparotomy; surgical abortion; surgery for skin-subcutaneous tissue; and orthopedic surgery involving deep tissue, bone, and joint. These top five common surgeries accounted for the majority of the surgical procedures (842, 87.7%; Table 1). The proportion of wounds that were class 2 was higher in the OB/GYN department than that in the surgical department (p < 0.01) mainly explained by cesarean delivery, and the systemic inflammatory response syndrome (SIRS) and or HAI were more common (p < 0.01). In the surgical department, the hospital mortality was higher (p < 0.01) than that in the OB/GYN department. Of the 15 patients with HAI, the most common diagnosis was SSI (14 patients).
Characteristics of Patients Who Underwent Surgical Procedures (N = 960)
OB/GYN = obstetrics/gynecology; SD = standard deviation: CDC = U.S. Centers for Disease Control and Prevention; SIRS = systemic inflammatory response syndrome; HAI = health-care–associated infections.
Length of antibiotic exposure at patient level
The mean length of antibiotic use and AFDs among all the patients were 3.5 days and 1.7 days, respectively (Table 1). The mean length of stay in the surgical department was longer than in OB/GYN (p < 0.01), as were the mean length of antibiotic use and AFDs (p < 0.01). Only 53 patients (5.5%) received no antibiotic agents during hospitalization. Two-thirds (35/53, 66.0%) of these patients were hospitalized in OBGYN, with cesarean delivery being the most common (14 patients).
Among the 907 patients who received antibiotic agents at any point during hospitalization, only 36 patients (4.0%) started and completed their antibiotic agents on the day of surgery (Table 2). Rather, the majority of the patients (766/907 patients, 84.4%) started receiving antibiotic agents on the day of surgery and continued for at least a day after. This practice was more common in the OB/GYN department than in the surgical department.
Antibiotic Use among Patients Who Underwent Surgery during Hospitalization (N = 907)
OB/GYN = obstetrics/gynecology.
Most patients (97%; 880/907) took antibiotic agents on the day of surgery (Fig. 1). Of these, the mean length of antibiotic use and extra days of antibiotic use after surgery were 3.7 days and 2.4 days, respectively (Table 3). After adjusting for SIRS/HAI occurrence and wound class, the length of antibiotic use and the extra days of antibiotic use after surgery were 2.9 days (95% CI = 2.7–3.3) and 1.9 days (95% CI = 1.7–2.3), respectively.
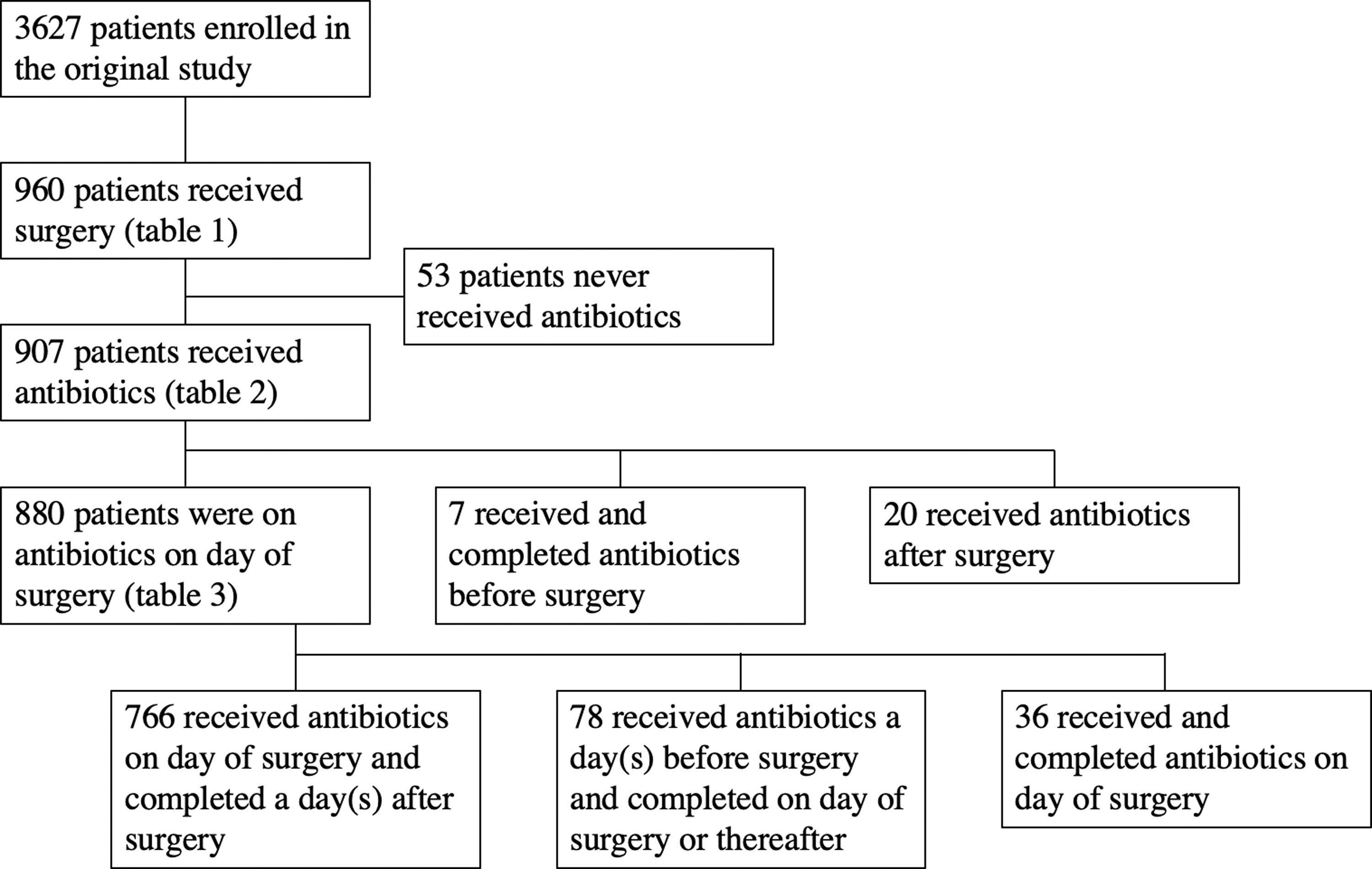
Flow chart of the patients studied.
Duration of Antibiotic Use for Patients Who Received Antibiotic Agents on the Day of Surgery (N = 880)
SD = standard deviation; CI = confidence interval; 1OBGYN: obstetrics/gynecology
SIRS: systemic inflammatory response syndrome
HAI: healthcare associated infections
CDC: United States Centers for Disease Control and Prevention
Type of antibiotic exposure, DOTs for antibiotic agents, and total AFDs
At the patient level, more than two-thirds (609, 67.1%) of patients among 907 patients who ever received antibiotic agents during hospitalization received a combination of ceftriaxone and metronidazole, followed by a single regimen of ceftriaxone (Table 2). The combination of ceftriaxone and metronidazole was more common in the OB/GYN department whereas other combination regimens were more common in the surgical department (p < 0.01). The combination of ceftriaxone and metronidazole was particularly common among those who underwent cesarean delivery (423/474 patients, 89.2%).
In total, 45 regimens of single or combination antibiotics of 11 different types were given with the total 6,503 DOTs of antibiotics. Ceftriaxone and metronidazole accounted for more than 80% of the total DOTs (2,852 DOTs, 43.9% and 2,372 DOTs, 36.5%, respectively; Fig. 2). In the total 4,960 inpatient-days of all 960 patients, the number of AFDs was 1,649 days (33.2%).
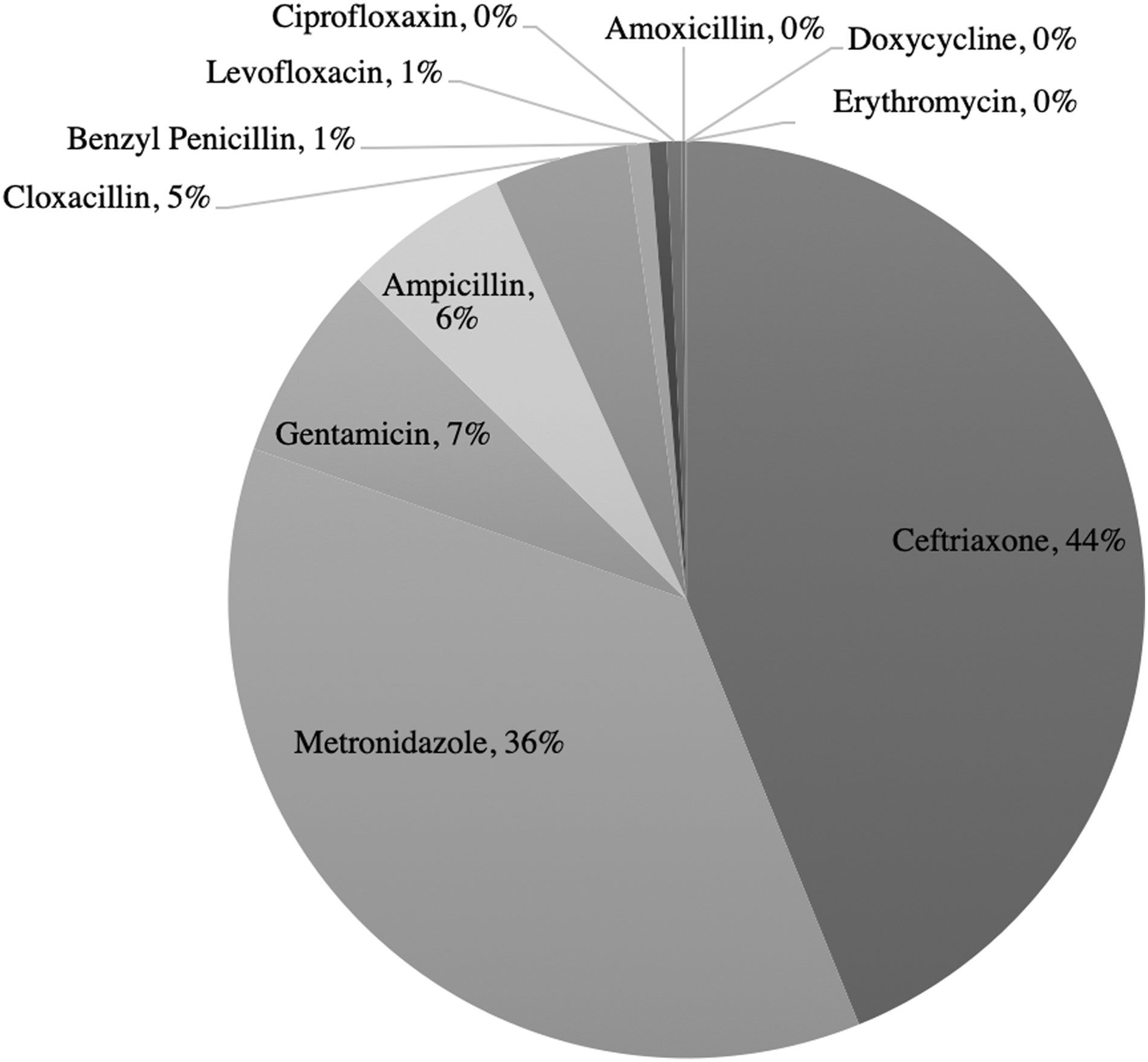
Days of therapy (DOTs) of antibiotics given.
Discussion
This study shows antibiotic use among patients who underwent surgery at a regional referral hospital in Uganda. To our knowledge, this is one of the largest studies to describe peri-operative antibiotic use in Uganda. Even after adjusting for covariates of SIRS/HAI occurrence and wound class (the important determinants of prolonged antibiotic use), antibiotic agents were given for an average of 2.9 days during hospitalization, an extra 1.9 days after surgery, and the usage was longer than usually recommended across different patient groups, including those without SIRS/HAI whose antibiotic use was likely SAP, and those with wounds that were CDC class 1.
At the study population level, AFDs account only for one-third of the total inpatient-days (1,649 AFDs of 4,960 inpatient days). The 6,503 DOTs occurred during the remaining 3,311 non-AFDs patient days, demonstrating that on average two different antibiotics were given each day among those who received antibiotic agents. Furthermore, we found more than 40 different antibiotic regimens used by clinicians. Although there is likely to be a discrepancy between the WHO recommended defined daily dose (DDD) and DOT [22], our study shows the measurement of DOTs and AFDs is more applicable and may be of clinical value in resource-limited settings.
Prolonged SAP after surgery (extended antibiotic use for the purpose of SSI prevention after surgery) is not recommended by WHO or other guidelines [8,9,11,24,25]. A single dose is generally considered sufficient and its effectiveness compared with prolonged post-operative antibiotic use has been proven in several studies in Africa [26]. However, post-operative antibiotic overuse in other African countries has been described [18,27]. The findings of this study were similar to those previously reported: antibiotic overuse was seen even among low-risk patients such as those without SIRS/HAI and those with class 1 wounds. Even after adjustment, the linear regression analysis still showed an extra 1.9 days of antibiotic use post-operatively, excluding the day of surgery. In addition, the combination regimen was extremely high among those who received antibiotic agents: more than four in five patients (737/907 patients, 81.3%) received the combination regimen. This compares with 22.5% found in a 2006 study in Tanzania [27].
The combination regimen of ceftriaxone and metronidazole most commonly given for cesarean delivery in the OB/GYN department may not be ideal. It is unnecessarily broad-coverage for SAP [8,28,29] and has weak coverage on skin flora, the common pathogens of SSI. Methicillin-resistant Staphylococcus aureus (MRSA) is reported to be increasingly common in Africa as well as multi-drug–resistant Enterobacteriaceae such as extended spectrum β-lactamase (ESBL)-producing Enterobacteriaceae [30,31]. Although no clear consensus is available on whether SAP coverage should be modified based on the local prevalence of MRSA and ESBL Enterobacteriaceae [9,11,28], AMR trends need to be monitored locally. In the meantime, antimicrobial stewardship needs to be practiced even in this surgical population who often require SAP regardless of the underlying infectious disease status. Although the risk of SSI is higher in LMICs, the CDC, for example, recommends that SAP is often unnecessary for clean procedures [20,28]. The risk-benefit balance of SAP for clean procedures in resource-limited setting may warrant further research.
There are some limitations to this study. First, because the study was conducted in a pragmatic way with limited diagnostics [19], and the study was not designed specifically to assess antibiotic use, it is difficult to differentiate between antibiotic use for prophylaxis and treatment. The timing of antibiotics given pre-operatively and the number of doses given were also not collected. However, no more than 4% (36/907) of patients received antibiotics only on the day of surgery, and this clearly suggests the overuse of antibiotics is prevalent. In the previous study, we acknowledged the lower incidence of HAI including SSI during our study than usually reported, and reasoned that underdiagnosis and lack of documentation by the hospital staff were likely the case [19]. Therefore, a composite outcome of SIRS and/or HAI was used as a possible intermediate outcome of infection. Considering the type of surgery undergone by the patients analyzed in this study, half of them underwent cesarean delivery. Although women undergoing cesarean delivery may have underlying infection, most do not and so should only require prophylactic antibiotic agents. Major operations such as laparotomy accounted for less than 20% of the patients on the surgical ward (Table 1).
These findings suggest that the number of those who required antibiotic agents for treatment was not large at the timing of surgery. In addition, in this current study, those without SIRS/HAI, who were considered not to have an active infection, received antibiotic agents for an average of 3.3 days and an extra 2.2 days after surgery, respectively. Other stratifications and linear regression analyses with adjustment by covariates still suggested post-operative antibiotic use were likely given longer than necessary even among patients with low risk of SSI such as those with class 1 wounds. Furthermore, given that the data does not contain post-discharge antibiotic use, it is possible that the true post-operative antibiotic duration would be even longer than reported.
Second, the appropriateness of the type(s) of antibiotic agents used was not evaluated at the individual level. Most antibiotic agents were prescribed without senior clinical input and there was limited documentation in the case files to determine the reason for the choice [19]. The pattern of antibiotic use may also depend on local availability, which may be driven by financial constraints rather than clinical appropriateness, and the study lacks such information at the pharmacy level. In addition, microbiologic data including sensitivity testing was lacking at the hospital level to guide decision making. However, at the study population level, broad-spectrum antibiotics such as third-generation cephalosporin, ceftriaxone, are used commonly in many different regimens, posing a risk of AMR. Although tailored therapeutic antibiotic use is not realistic in such a resource-limited setting [32], a more standardized approach may be feasible for prophylactic antibiotic use. A national-, or ideally, hospital-level guideline/guidance for SAP could promote more judicious antibiotic use with narrow-spectrum antibiotic agents as well as optimal timing, dose, and duration. Ideally, this would be supported by regular supplies of the appropriate antibiotic agents to the hospital, rather than having to rely on the patients' family attending the local pharmacy and using what is available and affordable.
Conclusions
In conclusion, our study showed widespread overuse of peri-operative antibiotics, particularly post-operatively, among surgical patients in surgical and OB/GYN departments at a regional referral hospital in Uganda. There was also evidence of inappropriate prescribing. Given the growing global AMR threat, improvements in prophylactic surgical antibiotic regimens should be promoted.
Footnotes
Acknowledgments
We acknowledge the following data clerks (Macreen Mudoola, Emily Nasiyo, Rose Wataka, and Grace Abongo), research assistants (Winfred Mutaki, Takali Sylvia, Christine Limio, Ekido Lossira, Rosemary Lunyolo, Proscovia Auma, Florence Ouchi, Bumba Ebyesali and Michael Maweda) who ensured smooth data collection.
The Wardgel study, of which this is a secondary analysis, was approved by the Mbale Regional Referral Hospital Institutional Review Committee (REIRC IN–COM 098/2014) and registered with ![]() (NCT02435719). The ethics committee considered this data collection as standard ward practice and waived individual consent. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
(NCT02435719). The ethics committee considered this data collection as standard ward practice and waived individual consent. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding Information
The study was conducted with funding provided by Saraya East Africa Co. Ltd., but the funder was not involved in the study design, data collection, data analysis, data interpretation, or manuscript writing.
Author Disclosure Statement
The authors declare that they have no competing interests. No competing financial interests exist.