
Abstract
Objective:
To explore the value of the difference in procalcitonin (PCT) levels in serum and cerebrospinal fluid (CSF) for diagnosing intracranial infection in post-neurosurgical patients.
Methods:
Patients who were treated at our hospital after craniotomy from January 2015 to January 2019 were enrolled in this study. Twenty patients eventually diagnosed with intracranial infection were included in a study group and 22 patients with no intracranial infection were included in a control group. A t-test was used to compare the differences between serum and CSF PCT levels of PCT, and the diagnostic value of PCT was evaluated by receiver operating characteristic (ROC) curve analysis.
Results:
The serum PCT levels in the study and control groups were 0. 10 ± 0. 03 ng/mL and 0. 09 ± 0. 03 ng/mL, respectively, and they were not substantially different between the groups. The CSF PCT level in the study group was substantially higher than that in the control group, with values of 0. 13 ± 0. 03 ng/mL and 0. 07 ± 0. 02 ng/mL, respectively. The CSF/serum PCT ratio in the study group was substantially higher than that in the control group, with values of 1. 31 ± 0. 19 and 0. 79 ± 0. 23, respectively. The areas under the ROC curve for serum PCT, CSF PCT and the CSF/serum PCT ratio were 0. 56, 0. 92, and 0. 95, respectively, resulting in a substantial difference among the three groups.
Conclusion:
CSF PCT may be a valuable marker for diagnosing intracranial infection in patients after neurosurgery; in particular, the specificity of CSF PCT is higher if the CSF PCT level is higher than the serum PCT level.
Secondary intracranial infection after craniotomy is a common complication, with an incidence ranging from 1% to 10% [1,2], and it is an important reason for increases in hospital costs and hospitalization time. The diagnostic criteria for intracranial infection include elevated body temperature, clinical symptoms, and laboratory examination findings, but these findings lack specificity. In addition, it is difficult to distinguish post-neurosurgical bacterial meningitis (PNBM) from aseptic meningitis, which is caused by an aseptic inflammatory response to the products of sloughing tissue, tumor antigen hemolysis, bone dust, and hemolysis. If the diagnosis is delayed, intracranial infection is likely to cause complications in the central nervous system and seriously affect the prognosis. Therefore, rapidly distinguishable and accurate biomarkers can improve the prognosis of patients with PNBM. Recent studies have found that procalcitonin (PCT) is an indicator of systemic bacterial infection that can be used to diagnose intracranial infections [3–6]. However, other scholars believe that cerebrospinal fluid (CSF) PCT is derived from the serum as a result of the destruction of the blood-brain barrier; it is affected by surgical trauma, anesthesia, and other factors and it cannot be used to differentiate infectious fever from noninfectious fever [7]. In summary, the usefulness of CSF PCT in the diagnosis of intracranial infection has not been demonstrated fully. Whether PCT is locally produced in the central nervous system is a matter of debate. The purpose of this study was to compare serum and CSF PCT levels to investigate the value of PCT for diagnosing intracranial infection in patients with PNBM.
Patients and Methods
Patients
This prospective observational cohort study was conducted from January 2015 to January 2019 in the intensive care unit (ICU) of Ningbo Yinzhou People's Hospital. All patients (>18 years) who had undergone surgery 48–72 hours previously were recruited to participate in this study. The study group was diagnosed with intracranial infection, and the control group included patients in whom intracranial infections had been excluded. Twelve males and eight females were included in the study group, with an age range from 38 to 83 years (average: 67.20 ± 12.22 years). Twelve males and 10 females were included in the control group, with an age range from 42 to 86 years (average: 66.89 ± 11.83 years). All patients had cerebral hemorrhage, including 29 cases of hypertension-associated hemorrhage, six cases of a ruptured aneurysm, and seven cases of a ruptured vascular malformation.
Methods
For patients who were suspected of having an intracranial infection after neurosurgery, informed consent was obtained, a lumbar puncture was performed, and a CSF sample was taken to the laboratory for routine CSF analysis, biochemical analysis, culturing, and the measurement of CSF PCT levels. Serum PCT levels were measured simultaneously. All procedures were based on the assumption of an absence of bacterial infection.
Diagnostic criteria for intracranial infection
The diagnostic standards in this study included the following: the presence of clinical symptoms of intracranial infection; a positive CSF culture; a CSF white blood cell (WBC) count ≥1,000 cells per microliter and a polykaryocyte percentage ≥75%; and a CSF glucose level <2.5 mmol/L or a CSF/serum glucose ratio <0.4 [8]. The diagnosis of intracranial infection was made individually in patients meeting the second criterion. Intracranial infection was also diagnosed in patients with negative CSF culture results but who met the other three diagnostic criteria. Those who had one or more of the criteria but did not meet the second criterion or all three other diagnostic criteria were considered as the control group. Patients with none of the inclusion criteria were excluded from our study.
Detection methods
All patients who underwent craniotomy also underwent a lumbar puncture for the collection of CSF specimens. Fifteen milliliters of CSF were collected in a sterile test tube, 5 mL of which was centrifuged for five minutes (3,000 r/rain), after which PCT was detected. The residual CSF samples were immediately sent to the clinical laboratory, and a VITROS 5. 1 FS automatic chemistry analyzer (Diamond Diagnostics, Citrus Heights, CA) was used to detect the CSF components (protein, chloride, and glucose levels). Procalcitonin was detected using an enzyme-linked fluorescence method (bioMérieux Marcy L'Etoile, France); the lower limit of positivity was 0. 05 ng/mL, as determined by the manufacturer. Blood samples were obtained by peripheral venipuncture under sterile conditions, and the time interval between CSF and blood sample collection in the same patient was <30 minutes.
Statistical analysis
The statistical analysis was performed using SPSS 20.0 software (IBM Corp., Armonk, NY). Normally distributed data and count data were compared by t-tests and χ2 tests, respectively. Receiver operating characteristic (ROC) curve analysis was used to analyze the diagnostic efficacy of PCT. A value of P < 0. 05 was considered statistically significant.
Results
Comparison of general data between the two groups of patients
No differences were observed in age, body temperature, gender, APACHE II score, serum C-reactive protein (CRP) levels or CSF protein levels, leukocyte counts, and chloride levels between the two groups, but an important difference was found in CSF glucose levels between the two groups (p > 0. 05, Table 1).
General Data from the Two Groups at Admission
CRP = C reactive protein; CSF = cerebrospinal fluid.
Distribution of cerebrospinal fluid pathogens in the study group
Pathogenic bacteria were cultured from the cerebrospinal fluid of seven patients in the study group, with a positivity rate of 35%. A total of nine strains of pathogenic bacteria were detected, including Staphylococcus aureus, Enterococcus faecium, epidermis Staphylococcus aureus, Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Escherichia coli, among which gram-positive bacteria accounted for 44%, and gram-negative bacteria accounted for 56%. Samples from two of the patients were positive for the presence of two strains of pathogenic bacteria (Table 2).
Structure of Pathogens Isolated from Patients with Intracranial Infection
Measurement of PCT levels
The PCT positivity rates in the CSF in the study and control groups were 100% and 73%, respectively, when the positive reference value was 0. 05 ng/mL or higher, which resulted in a statistically significant difference between the two groups (p < 0. 05, Table 3). A statistically significant difference in CSF PCT levels was observed between the two groups (p < 0. 05, Table 4). No significant difference in serum PCT levels was found between the two groups (p > 0. 05, Table 4).
Positive Rate of CSF for PCT in the Two Groups
CSF = cerebrospinal fluid; PCT = procalcitonin.
Serum and CSF PCT Data of the Two Groups
CSF = cerebrospinal fluid; PCT = procalcitonin.
Analysis of the efficacy of PCT in the diagnosis of intracranial infection by ROC curve
The areas under the ROC curves of serum PCT, CSF PCT, and the CSF/serum PCT ratio were 0.56, 0.92 and 0.95, respectively (Fig. 1), resulting in a substantial difference among these factors (Table 5). When the cutoff value of PCT for a diagnosis of intracranial infection was >0.05 ng/mL, the diagnostic sensitivity of CSF PCT was 100% and the specificity was <27%; furthermore, the diagnostic sensitivity of serum PCT was 90%, and the specificity was 5%. When the cutoff value was increased to 0. 09 ng/mL, the sensitivity of CSF PCT for diagnosing intracranial infection was 80% and the specificity increased to 82%. The specificity and sensitivity of serum PCT were 27% and 60%, respectively. When a CSF/serum PCT ratio >1 was used to diagnose intracranial infection, the specificity and sensitivity were 86% and 95%, respectively.
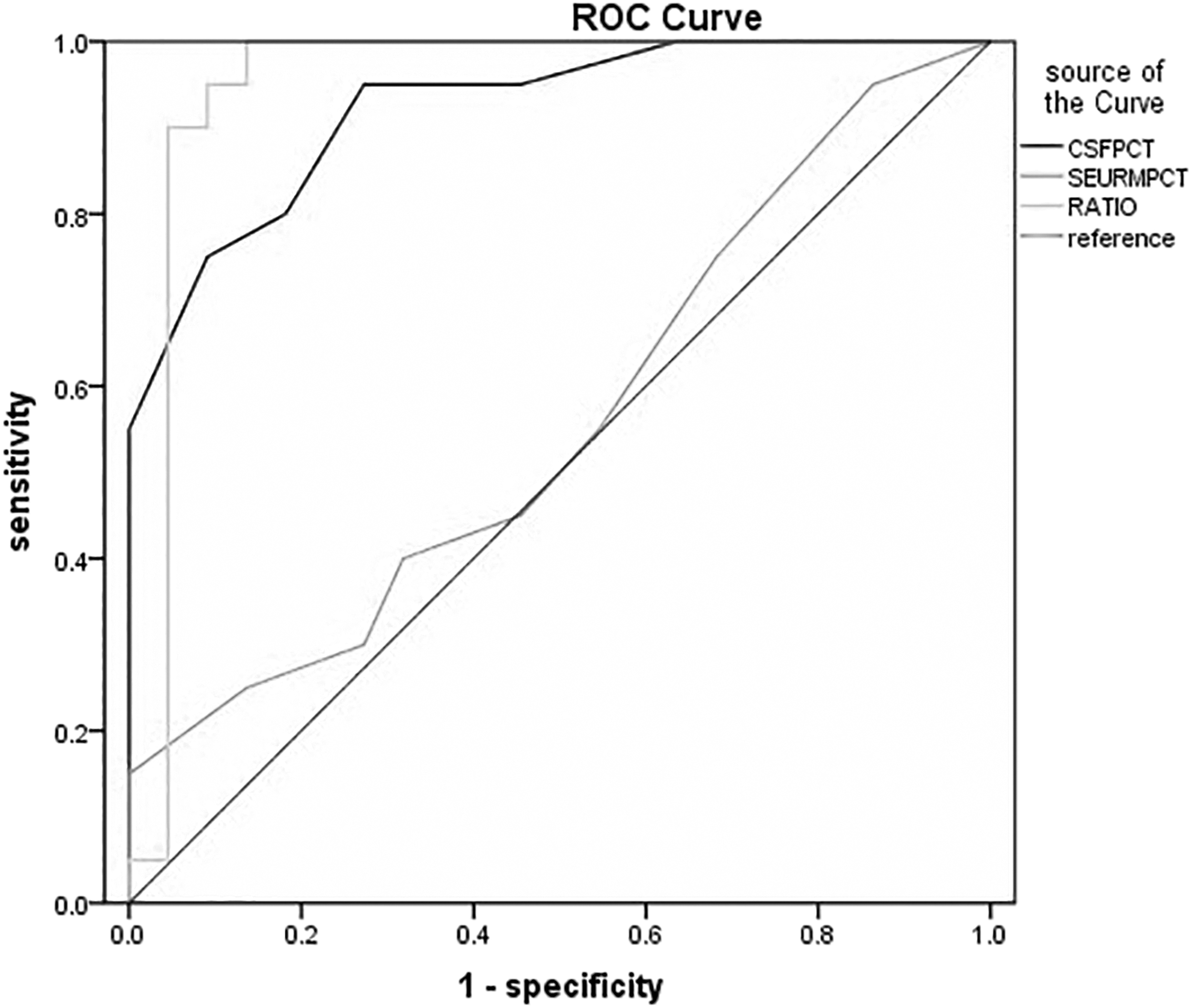
Receiver operating characteristic (ROC) analysis illustrating that the cerebrospinal fluid (CSF) procalcitonin (PCT) and CSF/serum PCT ratio are significant predictors of the post-neurosurgical bacterial meningitis (PNBM) (area under the curve [AUC] = 0. 92, p < 0. 005, and AUC = 0. 95, p < 0. 005, respectively).
Area under the ROC Curve
Indicates a comparison with serum PCT.
ROC = receiver operating characteristic; CSF = cerebrospinal fluid; PCT = procalcitonin.
Difference in the CSF/serum PCT ratio between the two groups
The CSF/serum PCT ratio was (1.31 ± 0.19) in the study group and (0.79 ± 0.23) in the control group, resulting in a statistically significant difference between the two groups (p = 0. 01, Table 6).
CSF/Serum PCT Ratio of Two Groups
CSF = cerebrospinal fluid; PCT = procalcitonin.
Discussion
Intracranial infection is a common complication of postoperative cerebral hemorrhage, but the diagnosis of intracranial infection lacks specific indicators or examinations and mainly relies on CSF examinations [9]. The sensitivity of routine and biochemical CSF examinations is high, but the specificity is low, which is consistent with the results of this study. The bacterial culture of CSF remains the gold standard for the diagnosis of intracranial infection, but the positivity rate in our study was only 35%, and the culturing requires a long time, which is not conducive to the early diagnosis of intracranial infection. Therefore, it is important to identify sensitive, specific, simple, and easily detectable indicators for the clinical diagnosis and treatment of intracranial infections. Procalcitonin is a prepeptide of calcitonin. When the body becomes infected with bacteria, the concentration of PCT in the blood increases within a short time and the PCT concentration is positively correlated with the severity of the infection. Therefore, PCT is a key indicator for the diagnosis of bacterial infection and has been used widely in clinical practice [10,11]. Recent studies have also shown that elevated PCT levels in the serum and CSF may be used for the diagnosis of intracranial infection. Other studies have shown that CSF PCT has better sensitivity and specificity than serum PCT [12–15]. Additionally, studies have suggested that increased CSF PCT is a non-specific finding, even though the brain tissue itself does not produce synthetic secretions [16,17]. However, the role of CSF PCT in the diagnosis of intracranial infection and whether the brain tissue itself secretes PCT remain unclear.
This study found that the CSF PCT levels in the infected group were substantially higher than those in the non-intracranial infection group. However, no difference was observed in serum PCT levels between the two groups. Furthermore, we found that the area under the ROC curve for CSF PCT was 0.92, which was substantially different from the area under the ROC curve for serum PCT (by 0.56). These findings suggest that increases in CSF PCT levels can be used for the diagnosis of intracranial infection, which is similar to the conclusions of many other studies [13,14,18]. However, in this study, serum PCT did not show good diagnostic value for intracranial infection, which is consistent with the results of Choi et al.'s study [19]. We hypothesized that because intracranial infection is a localized rather than a systemic infection, the difference in serum PCT levels would not be significant. Although many studies (including a meta-analysis) have suggested that CSF PCT is a good potential indicator for the diagnosis of intracranial infection, reference values have not been determined [20]. At present, most studies use the reference value for serum PCT (0. 05 ng/mL). However, this study found that the positivity rate of CSF PCT in the control group was 73%, the sensitivity of CSF PCT in the diagnosis of intracranial infection was 100%, and the specificity was less than 27%; obviously, these results do not meet clinical requirements. The Guidelines for Healthcare-Associated Ventriculitis and Meningitis have advised that increased CSF PCT levels may indicate intracranial infection [21]. However, the optimal cutoff value for PCT using the Youden index was 0. 09 ng/mL, which yielded a sensitivity for diagnosing intracranial infection of 80% and a specificity of 82%, which meet clinical needs. This threshold is similar to those in several other studies [22–24].
When CSF and serum PCT levels were compared simultaneously, we found that most patients with intracranial infections had higher CSF PCT levels than serum PCT levels, and the CSF/serum PCT ratio was different between the two groups. When intracranial infection was diagnosed using a CSF/serum PCT ratio >1, the area under the ROC curve was 95%, the specificity was 95%, and the sensitivity was 86%. These sensitivity and specificity values meet clinical needs. To the best of our knowledge, this is the first study to diagnose intracranial infection in patients with PNBM using the CSF/serum PCT ratio. Clearly, the nerve tissue itself also stimulates the secretion of PCT because of inflammation, and the CSF PCT is not derived from serum PCT. Therefore, the presence of higher CSF PCT levels than serum PCT levels can be used for the diagnosis and differential diagnosis of intracranial infection, and the specificity of this method is better than that of the use of the CSF PCT level alone.
In conclusion, we suggest that CSF PCT is highly sensitive for the diagnosis of intracranial infections, but it lacks specificity, which is consistent with the Guidelines for Healthcare-Associated Intracranial Infections developed by the American Society of Infectious Diseases in 2017. However, the specificity of CSF PCT increases with increasing cutoff values or when CSF PCT levels are higher than serum PCT levels.
This is an exploratory study and has several limitations. First, the clinical status of patients in the intensive care unit is complex, and they can have various infections. The sample size of the enrolled group was small, and the positivity rate of CSF culture was too low. We did not have enough samples to compare the differences in CSF PCT among different pathogen types. We will try to collect more samples from multiple centers. At the same time, the detection rate of pathogenicity can be increased by the second generation sequencing method of the CSF; we will dynamically observe the changes in serum PCT and CSF PCT before and after anti-infection therapy and explore the guiding effect of CSF on anti-infective efficacy. We plan to explore whether the increase in PCT in CSF is related to bacterial endotoxin, tumor necrosis factor, interleukin-1, interleukin-6, and other inflammatory factors. Further research is needed to verify the usefulness of measuring PCT for the early diagnosis of intracranial infections in patients undergoing craniotomy.
Footnotes
Acknowledgments
I thank all of the patients, doctors, and staff involved in the study. I also thank my family for their support.
Funding Information
This work did not require any funding.
Author Disclosure Statement
No competing financial interests exist.