
Abstract
Background:
Methicillin-resistant Staphylococcus aureus (MRSA) infection remains a challenging threat because of limited treatment options. Ceftaroline was identified as having potent anti-MRSA activity.
Aim:
To evaluate the susceptibility of MRSA to gentamicin, macrolides, ciprofloxacin, vancomycin, and ceftaroline and to perform molecular characterization of different resistance genes as aminoglycoside modifying enzyme genes, ermA and ermC, and vanA and vanB genes.
Patients and Methods:
One hundred non-duplicate MRSA strains were isolated from different samples of hospitalized patients in Cairo University teaching hospitals from November 2015 to August 2016. Determination of antibiotic susceptibility was done using disk diffusion test and minimum inhibitory concentration followed by detection of resistance genes by multiplex polymerase chain reaction (PCR).
Results:
Of 100 MRSA isolates, 63 (63%) were resistant to gentamicin, erythromycin, clindamycin, and ciprofloxacin, however, all were sensitive to ceftaroline. Fifteen isolates (15%) were vancomycin intermediate resistant and were sensitive to ceftaroline as well.
Conclusion:
Ceftaroline was potent against MRSA, which was found to be non-susceptible to vancomycin, ciprofloxacin, erythromycin, clindamycin, and gentamicin and it may represent a successful treatment for MRSA infections.
Staphylococcus aureus, in particular methicillin-resistant Staphylococcus aureus (MRSA), infections are of great concern in hospital and community settings throughout the world. Nosocomial infections caused by MRSA include surgical site infections, ventilator-associated pneumonia, catheter-associated urinary tract infections, and central line blood stream infections [1,2]. Methicillin resistance is mediated through alternation of Staphylococcus aureus penicillin-binding protein (PBP) to a low-affinity PBP2a rendering it resistant to β-lactam antibiotic agents. This altered protein is encoded predominantly by the mecA gene. Commonly, health-care–associated MRSA strains are resistant to antibiotic agents other than β-lactam [3,4]. There are limited therapeutic options for emerging MRSA infections. Clindamycin is considered one of the alternatives for treating MRSA infections [2]. However, Staphylococcus aureus strains may show resistance to it [5]. The main mechanism of resistance to macrolide-lincosamide streptogramin B (MLSB) antibiotics is expression of erm genes either constitutively (cMLSB phenotype) or inducibly (iMLSB phenotype) leading to target site modification [6].
Aminoglycosides have potent bactericidal activity by irreversibly inhibiting bacterial protein synthesis. They have been administered commonly with glycopeptides for treatment of infections caused by multi-drug–resistant (MDR) Staphylococcus aureus. However, presence of aminoglycoside resistance in MRSA has been reported through drug inactivation by aminoglycoside-modifying enzymes (AMEs) encoded by aac(6′)- Ie+aph(2′′), aph(3′)-IIIa, and ant(4′)-Ia [7].
Vancomycin is a glycopeptide antibiotic agent used for treatment of severe MRSA infections. There are two types of glycopeptide-resistance in Staphylococcus aureus: vancomycin-intermediate Staphylococcus aureus (VISA), which is associated with cell wall thickening and vancomycin-resistant Staphylococcus aureus (VRSA) through acquisition of vanA or vanB genes [8]. Vancomycin resistance is associated with persistent infections and poor clinical outcomes [9,10].
New treatment options for MRSA including ceftaroline, daptomycin, linezolid, telavancin, tedizolid, oritavancin, and dalbavancin have been increasing [11–13]. Ceftaroline is a fifth-generation cephalosporin that is mostly active against MRSA [14]. It has both in vitro and in vivo activities against MRSA [15]. This antimicrobial agent has a high affinity to PBP2a associated with methicillin resistance that leads to inhibition of cell wall synthesis [16]. Ceftaroline is used for treatment of MRSA skin and skin structure infections for pediatric and adult patients, as well as MRSA bacteremia and endocarditis [14]. This new drug could be used as a salvage therapy for complicated MRSA infections [15]. However, inappropriate use of other β-lactam antibiotic agents may lead to cross-resistance to ceftaroline [14]. This study was conducted to detect the antibiotic susceptibility of MRSA strains isolated from various samples of patients with hospital-acquired infections and the presence of related antibiotic resistance genes. It also aimed to evaluate the in vitro activity of ceftaroline against MRSA strains.
Patients and Methods
Bacterial isolates
A cross-sectional study was conducted in Cairo University, Kasr Alainy Faculty of Medicine, Department of Medical Microbiology and Immunology. It included 100 non-duplicate strains of MRSA isolated from clinical samples of hospitalized patients with different infections from November 2015 to August 2016. Identification of Staphylococcus aureus was done by conventional biochemical methods including gram stain, catalase test, mannitol fermentation, DNase, and coagulase test. Screening for methicillin resistance was done by cefoxitin (30 μ) disk diffusion method. The strains included were resistant to cefoxitin (Table 1). Multiplex polymerase chain reaction (PCR) was used for amplification of nuc and mecA genes as a confirmatory method for Staphylococcus aureus species and methicillin resistance, respectively (17).
Antibiotic Zone Diameter and MIC Interpretative Criteria (CLSI, 2016)
I = intermediate; S = sensitive; R = resistant; MIC = minimum inhibitory concentration; μ = micron.
Antibiotic susceptibility testing
Susceptibility of the isolates to different antibiotic agents was assessed including gentamicin (10 mcg), erythromycin (15 mcg), clindamycin (2 mcg), and ciprofloxacin (5 mcg) (Table 1). D-test was performed to detect inducible clindamycin resistance in Staphylococcus aureus [18]. A clindamycin disk was placed 15 mm from an erythromycin disk on a Mueller-Hinton agar and inoculated with standard bacterial suspension of 0.5 McFarland. After overnight incubation at 37°C, flattening of the zone around clindamycin (D-shaped) in the area between the two disks indicated a positive D-test. Four types of phenotypes are identified by the D-test:
Sensitive phenotype: Staphylococcus aureus sensitive to erythromycin and clindamycin. Moderate sensitive phenotype (MS) (negative): Staphylococcus aureus resistant to erythromycin and sensitive to clindamycin (no D-zone). Inducible resistance phenotypes (iMLSB): Staphylococcus aureus showed resistance to erythromycin with D-zone around the clindamycin. Constitutive resistance phenotypes (cMLSB): Staphylococcus aureus was resistant to both erythromycin and clindamycin.
Vancomycin minimum inhibitory concentration (MIC) was detected by the Mueller-Hinton broth (HiMedia Laboratories, Kennett Square, PA) microdilution method [18]. Ceftaroline E-test (bioMérieux, Marcy l'Etoile, France) was done for MRSA strains. Interpretation of vancomycin and ceftaroline MIC were applied as illustrated in Table 1.
Detection of antibiotic resistance genes
All MRSA isolates were sub-cultured on blood agar plates followed by overnight incubation at 37°C. Total DNA extraction from the bacterial isolates was done using Biospin Bacteria Genomic DNA extraction kit (BioFlux Corporation, Tokyo, Japan) according to the manufacturer's instructions. In two multiplex PCR assays performed in PCR Biometra T-Personal thermal cycler (48 wells, Ver 09/10, Göttingen, Germany), amplification of the target genes was done using PCR master mix (Dream TaqTM Green PCR Master, Thermo- Fischer, San Jose, CA). Cycling conditions for multiplex amplification of nuc, vanB, ermA, and ermC genes, and multiplex amplification of mecA, vanA, aac(6′)/aph(2′′), aph(3′)-IIIa, and ant(4′)-Ia are illustrated in Table 2. A 10-mL aliquot of the product was analyzed in 1.5% agarose gel, and the amplified DNA products were observed under an ultraviolet (UV) transilluminator after staining with 0.5 mg/mL ethidium bromide. Target genes, primers' sequences, and size for each gene product are shown in Table 2 [19–23].
Target Genes, Primer Sequences, Product Size, and Multiplex PCR Cycling Conditions
PCR = polymerase chain reaction.
Statistical methods
Quantitative data were expressed as numbers and percentages. Analysis was done using IBM SPSS 21.0 Statistics (IBM, Armonk, NY). The Fisher exact test was used to analyze differences between groups. P value <0.05 was significant.
Results
In our study, 100 MRSA strains isolated from various samples of hospitalized patients were positive for nuc and mecA genes by PCR. Of 100 MRSA isolates, 89 (89%) were resistant to gentamicin, whereas 11 (11%) were sensitive. The 89 resistant and 10 of 11 sensitive isolates contained at least one of the genes encoding gentamicin resistance. The ant(4′)-Ia, aac(6′)/aph(2′′), and aph (3’)-IIIa genes were detected in 54%, 43%, and 40%, respectively. The presence and association of different genes with gentamicin susceptibility pattern is shown in Table 3.
Presence and Association of the Different Genes Encoding Gentamicin Resistance
AME = aminoglycoside modifying enzymes.
Of 100 isolates, 18 (18%) were resistant to erythromycin only, whereas 68 (68%) showed resistance to erythromycin and clindamycin. Eighty-six percent of isolates were resistant whereas 14% were sensitive to erythromycin. All isolates showing resistance to clindamycin were also resistant to erythromycin. The distribution pattern for the MLSB resistance phenotypes and ermA and ermC genes among MRSA isolates is shown in Table 4. Both ermA and ermC were detected in most strains with inducible clindamycin resistance (12/15) and constitutional clindamycin resistance (42/68). A total of 93 (93%) of the MRSA isolates contained ermA, ermC, or both. Seventy-nine percent of the isolates were resistant to ciprofloxacin, 4% were intermediate resistant, and 17% were sensitive. Among the studied isolates, 15% showed intermediate resistance to vancomycin (VISA) by broth microdilution method whereas 85% were sensitive. No vancomycin resistance was detected among MRSA isolates. The agreement between vancomycin susceptibility patterns and associated vanA and vanB genes is shown in Table 5.
Distribution of ermA and ermC in Relation to MLSB Resistance Phenotypes
MRSA = methicillin-resistant Staphylococcus aureus; ERY = erythromycin; CL = clindamycin; S = sensitive; R = resistant; MS = moderate sensitive phenotype; MLSB = macrolide-lincosamide-streptogramin B; MLSB = macrolide-lincosamide-streptogramin B antibiotic; cMLSB = constitutive MLSB-resistant phenotype; iMLSB = inducible MLSB-resistant phenotype; MSB = negative; S = sensitive phenotype.
The Agreement between the Results of Phenotypic (MIC) and Genotypic (Multiplex PCR) Susceptibility to Vancomycin
MIC = minimum inhibitory concentration; PCR = polymerase chain reaction.
The majority of the studied MRSA isolates (96%) were susceptible to ceftaroline. Only one isolate (1%) was resistant, whereas three (3%) were intermediate resistant to ceftaroline. Among the MRSA isolates, 63 of 100 (63%) were found to be resistant to all tested antibiotic agents by disk diffusion method (gentamicin, erythromycin, clindamycin, and ciprofloxacin), however, all were sensitive to ceftaroline. This was also applicable for all VISA strains (15 isolates) that were sensitive to ceftaroline as well. The phenotypic susceptibility pattern of ceftaroline-sensitive MRSA is illustrated in Table 6. Table 7 summarizes MRSA antibiotic susceptibility patterns. Seventy-two isolates (72%) of MDR Staphylococcus aureus were resistant to at least one antibiotic of each category except vancomycin. It was found that 71 were sensitive to ceftaroline whereas nine isolates (9%) of MDR Staphylococcus aureus were sensitive to at least one antibiotic of each category including VISA. The nine isolates were also sensitive to ceftaroline (Fig. 1).
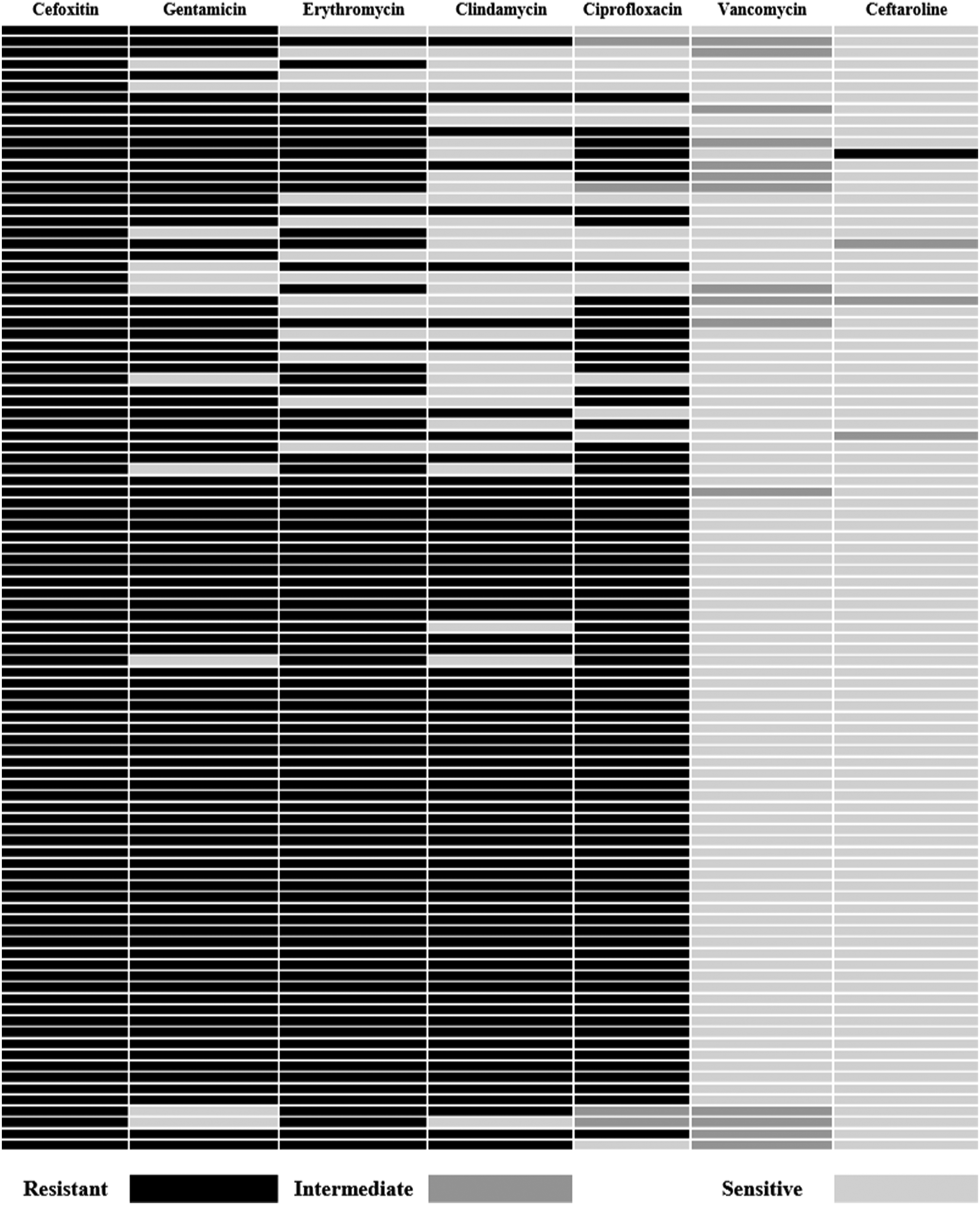
Heat map showing antibiotic resistance profile of all multi-drug– resistant methicillin-resistant Staphylococcus aureus (MRSA) isolates.
Phenotypic Patterns for the MRSA Isolates in Comparison with Ceftaroline
MRSA = methicillin resistant Staphylococcus aureus; S = sensitive; R = resistant;
The Susceptibility Data for the Tested Antibiotics
Discussion
Emergence of MDR Staphylococcus aureus is associated with high morbidity and mortality. Accurate reporting of resistant isolates is crucial for appropriate therapy decisions. The aim of the work was to evaluate the susceptibility pattern of 100 MRSA isolates from various clinical samples and assess the in vitro activity of ceftaroline against Staphylococcus aureus as an alternative to vancomycin. Resistance to gentamicin was observed in 89% of the isolates. A lower rate of gentamicin resistance (68%) was reported by Ardic et al. [24], whereas a recent study by Khosravi et al. [25] showed a similarly high rate (84.5%) indicating that gentamicin is no longer effective against MRSA infections. The high gentamicin resistance rate could be attributed to its use to treat serious staphylococcal and enterococcal infections (25).
Determination of AMEs genes was done using multiplex PCR. In this study, the ant(4′)-Ia was the highest gene detected (54%), followed by aac(6′)/aph(2′′) (43%) and aph(3′)-IIIa (40%). The same finding was reported in a study from Iran that revealed that ant(4′)-Ia was the most frequent gene (58%) followed by aac(6′)-Ie/aph(2″) (46%) and aph(3′)-IIIa (6%) (26). Similar results were also obtained in a study done in Japan by Ida et al. [27] who reported that the ant(4’)-Ia gene was the highest gene (84.5%) encoding gentamicin resistance. One of the reasons that the ant(4)-Ia gene is the most frequent is that it adjoins the mecA gene (27). Ardic et al. [24] reported that the aac(6′)/aph(2′′) gene was the most frequent AME gene (66%), followed by ant(4′)-Ia (24%) and aph(3′)-IIIa genes (8%). Vanhoof et al. (28) reported that the most prevalent gene detected among MRSA isolates in Europe was aac(6')/aph(2'') and Choi et al. [22] obtained similar results in South Korea. This could be attributed to the fact that aac(6′)/aph(2′′) is encoded by transposon Tn4001 or Tn4001-like elements that have been detected in Staphylococcus aureus.
Although aph(3′)-IIIa gene in this study was the lowest (40%), it was higher than reported in another study performed by Schmitz et al. [29] (14%). In contrast, a study done in Greece reported that aph(3')-IIIa was the predominant gene (73.3%) [30]. The aph(3′)-IIIa genes are transposon (Tn3854)-mediated on the staphylococcal chromosome and plasmid. The gentamicin-resistant plasmids in Staphylococcus aureus vary among different geographic areas [27]. The changes in prevalence of AMEs among the isolates can be explained by changes in antibiotic policies in different geographical regions combined with a possible inter-hospital spread of resistant strains by horizontal AME gene transfer (28). Many studies reported coexistence of methicillin and aminoglycoside resistance [29,31]. In this study, at least one of the genes encoding gentamicin resistance was detected in 10 of 11 gentamicin- sensitive isolates. This finding is in agreement with other studies and could be the result of the amplification of repressed resistance gene [32,33].
In this study, resistance of MRSA isolates to erythromycin (86%) and clindamycin (68%) was in partial agreement with a study done by Adhikari et al. [5] on 68 MRSA isolates who reported similar resistance rates of erythromycin (88.2%) although a higher rate for clindamycin (79.4%). Among the 86 erythromycin-resistant isolates, cMLSB, iMLSB, and MSB phenotypes were 68%, 15%, and 3%, respectively. Maina et al. [34] reported 60%, 38%, and 2%, respectively. Banik et al. [35] reported 30%, 15.38%, and 8.47%, respectively, whereas Adhikari et al. [5] reported 54.4%, 27.9%, and 10.3%, respectively. Variations in different MLSB-resistant phenotypes can be explained by geographical variations of circulatory clones and even between hospitals. Erythromycin resistance in staphylococci is predominantly mediated by erm genes encoding methylase. In this study, ermA, ermC, and coexistance of both were 22%, 12%, and 59%, respectively. Lina et al. [21] reported 57.6%, 4.9%, and 0%, respectively, whereas Saderi et al. [36] reported 81.4%, 74.4%, and 67.4%, respectively. A recent study done by Sedaghat et al. [37] reported 9%, 16.4%, and 11%, respectively. The ermA genes are borne by Tn554 transposons and spread to MRSA [21].
In our study, 15% of MRSA isolates were VISA. In Egypt, two recent studies done by Abdel-Maksoud et al. [38] and Mashaly et al. [39] reported VISA among MRSA isolates with rates of 1.2% and 10.9%, respectively. Another study done in Nepal by Pahadi et al. [40] reported 9.5% whereas a recent study done in Iran by Asadpour et al. [41] reported a rate of 17%. In this study, vanA was detected in 12% and vanB was detected in 6% of MRSA isolates. A study done by Fasihi et al. [42] reported that 1.2% (1/86) of MRSA were vanA positive, whereas vanB was not detected. Jahanshahi et al. [43] reported 4.3% (2/46) of MRSA were vanB positive, while no vanA was detected. Asadpour et al. [41] reported that 2% of the MRSA isolates were vanA positive (1/47). In a study conducted by Saadat et al. [44], vanA and vanB were detected in 34% and 37% of Staphylococcus aureus isolates, respectively. Neither vanA nor vanB was detected in a study done by Bamigboye et al. (45).
In the current study, a considerable number of vancomycin-sensitive isolates (15/85) contain either vanA or vanB without being expressed, which highlights the potential of these isolates to express the vancomycin resistance under selective antibiotic pressure. Saadat et al. [44] reported 19 of 100 Staphylococcus aureus isolates with detected vancomycin resistance gene but that were phenotypically sensitive to vancomycin. In our study, 96% of MRSA including the 14 VISA isolates were sensitive to ceftaroline. Abbott et al. [46] tested 421 MRSA strains, 350 (83%) of which were susceptible to ceftaroline. However, Kelley et al. [47] reported results of a study detecting 40 of 60 (66%) MRSA isolates that were resistant to ceftaroline. A study conducted by Bakthavatchalam et al. [48] revealed that 85% (73/86) of MRSA isolates were sensitive to ceftaroline. Andrey et al. [49] reported that 73 of 96 MRSA strains (76%) were susceptible to ceftaroline. Another study done by Isnard et al. [50] reported that all Staphylococcus aureus including methicillin-resistant isolates (100%) were susceptible to ceftaroline.
Conclusions
Health-care–associated MRSA isolates in our setting appear to be multi-drug–resistant, which challenges the therapeutic options. Rates of resistance to gentamicin, erythromycin, clindamycin, and even quinolones were high in this study, which necessitate searching for new therapeutic options. Intermediate resistance to vancomycin appears to be increasing in our setting, whereas ceftaroline appears to be a good therapeutic option for MDR MRSA strains.
Recommendations
Antibiotic stewardship programs should monitor the appropriate use of antibiotic agents to avoid the increasing antibiotic resistance. Selective reporting of antibiotic agents from the clinical microbiology laboratory might help in this issue. Ceftaroline might be great concern for treating MDR MRSA strains. Further studies including larger number of isolates might be needed to assess the susceptibility testing of the MRSA isolates to ceftaroline properly.
Footnotes
Funding Information
No grant was received to conduct this study. No financial interests exist.
Author Disclosure Statement
No competing interests were declared by the authors.