
Abstract
Background:
A skin-sparing approach for the treatment of necrotizing soft-tissue infections (NSTIs) removes necrotic tissue planes while leaving viable overlying skin. Subsequent closure of the spared skin may decrease the need for graft-based reconstruction, which is associated with contracture, pain, and deformity. This study compared the outcomes of a traditional approach (excision of overlying skin with diseased fascia) with that of a skin-sparing approach for patients with NSTI treated at a major metropolitan medical center.
Methods:
Demographic, clinical, and operative details for patients treated for NSTI between July 2012 and December 2016 at a single institution were reviewed retrospectively. Pre-operative and post-operative photographs were evaluated independently by three surgeons to determine reconstructive outcomes. Cohen's κ was used to assess inter-rater reliability. Multiple regression and Poisson regression models were used to assess the association between outcomes and the surgical approach.
Results:
A total of 487 patients were divided into two cohorts: Traditional approach (TA), treated between July 2012 and December 2014 (n = 230), and skin-sparing approach (SS), treated after January 2015 (n = 257). The mortality rate in the two groups was equal at approximately 10%. The median percentage of each wound closed by skin graft was significantly lower for the SS group than for the TA group (20% versus 90%; p < 0.0001) with a correspondingly higher median percentage of primary skin closure for the SS group (50% versus 0; p < 0.0001).
Conclusions:
Relative to traditional debridement, skin-sparing debridement for source control of NSTI results in significantly more wounds closed completely by delayed primary suture of existing skin flaps and a significantly lower overall wound percentage closed by skin graft, while demonstrating equivalent efficacy of source control and a similar low mortality rate.
Necrotizing soft-tissue infections (NSTIs) are rapidly progressing bacterial infections that require prompt and complete surgical source control. Although the incidence of these infections is difficult to measure, it appears that approximately 500–1,500 cases per year are captured, although with a recent increase thought to be related to persistent antibiotic resistance. Greater awareness, advances in critical care, and appropriate surgical intervention have contributed to the overall decrease in the NSTI mortality rate from 34% in the 1990s [1] to 4.9 [2]–25% in the 2000s [3]. With increasing survival, the focus must expand now from purely preserving life to preserving quality of life.
The traditional approach (TA) for NSTI treatment is wide debridement of all overlying skin, fat, and fascia, and, in some circumstances, muscle and even bone. This technique leaves patients with large surface-area wounds associated with substantial functional, cosmetic, and psychological morbidity post-operatively. Given the decreasing mortality rate in recent decades, we proposed a skin-sparing (SS) approach that focuses on debridement only of tissue directly involved in necrosis, leaving viable overlying skin and subcutaneous tissue intact [4]. The evolution of the surgical management of breast cancer parallels this approach. The radical mastectomy described by Dr. William Halsted in the 19th Century decreased deaths [5] while producing substantial morbidity. With improved patient survival, the focus shifted toward preserving quality of life; thus, the modified radical mastectomy [6] and subsequent skin-sparing [7,8] and nipple-sparing mastectomies were described [9]. These adapted surgical techniques improved post-operative aesthetic results and quality of life without compromising oncologic outcomes [10,11].
The evolution of the management of NSTI must also adopt a quality of life preservation approach by following an SS strategy. We have described incision diagrams for each body region and documented a case series in our original publication [4]. Key concepts highlighted in the SS approach include maintaining unaffected skin, preserving skin perforators, covering vital structures, and limiting incisions over flexor surfaces (Fig. 1). In this article, we compare reconstructive and clinical outcomes between patients with NSTI who underwent a TA versus an SS approach.
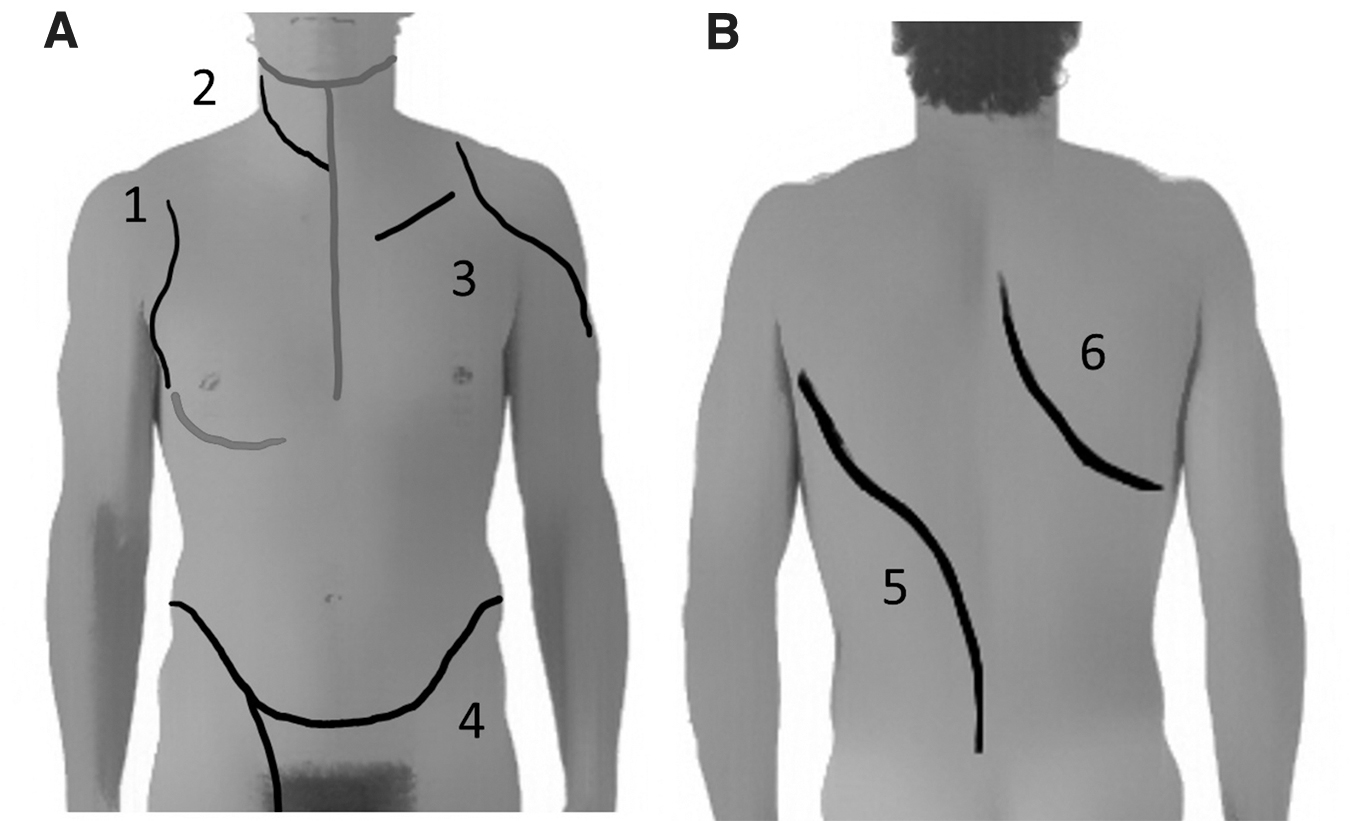
Skin-sparing incision diagrams: Torso. (
Patients and Methods
This was a retrospective cohort study to evaluate the outcomes of patients treated for NSTI with a traditional approach (TA) or with an SS approach at an academic tertiary referral center (Harborview Medical Center, Seattle, WA) from July 2012 through December 2016. The TA cohort data were collected retrospectively for patients admitted between July 2012 and December 2014 by using admission and discharge International Classifications of Disease 9 diagnosis codes and manual chart review to confirm the NSTI diagnosis. Patients without NSTI on review of the operative report and inpatient progress notes were excluded from the analysis.
In November 2014, attending surgeons who treated NSTIs at our institution underwent training and received an online curriculum about the SS approach [4]. After the introduction of the SS approach, for three consecutive months, attending surgeons were queried for each patient whether they attempted SS surgery; and 95% answered affirmatively. Beginning January 1, 2015, all patients admitted with NSTI were identified prospectively and captured in our NSTI registry. All these patients were included in the SS cohort, as this approach was implemented as the surgical approach for all NSTI patients at that time. Before January 1, 2015, five patients are classified as pilot patients on which the SS approach was developed and initiated. These patients were included as part of the SS cohort.
The University of Washington Institutional Review Board approved all study procedures.
Outcomes
Primary
The primary operative outcomes of interest were the percentage of wound closure achieved via primary closure versus skin grafting. Methods of closure included delayed primary closure, grafting, or skin flaps including local advancement and free flaps.
In a subgroup of patients who were treated between July 2012 and July 2016, photographs were available to analyze the percentage of wound closed by either primary, grafting, or secondary intention. Two plastic surgeons (LT and KK) and one general surgeon (BP) assessed pre-reconstruction and post-reconstruction photographs independently to calculate the percentage of wound closure achieved after reconstruction. Of note, one evaluator (BP) had not participated in any SS approach operations, did not have experience with the SS incisions prior to photograph review, and was blinded to the clinical histories of the subjects. The average of these three independent estimates was computed and used as the final value for the percentage closure in each subject. For patients for whom photographs were not available, operative reports were reviewed to determine the percentage of wound closed by delayed primary closure or by a skin graft.
Secondary
Secondary wound-related outcomes also were assessed, including the total area of the first debridement (cm2), amputation, and secondary revision operations such as for dehiscence or scar contracture. Other clinical outcomes included in-hospital death, ventilator-free days, hospital length of stay, acute renal failure (requiring new dialysis), acute respiratory distress syndrome (ARDS), and in-hospital cardiac arrest.
Sensitivity analysis
Only surgeons at Harborview Medical Center, and not the surrounding communities, were trained in the SS technique for this study. Thus, patients in the SS cohort who had debridement prior to transfer may have had larger initial debridements and worse clinical outcomes. Therefore, a sensitivity analysis of the primary and secondary outcomes was performed excluding all patients in both cohorts who were debrided prior to arrival at Harborview Medical Center.
Data presentation and statistical analysis
Categorical data are represented as counts and percentages, whereas continuous data are represented as medians with interquartile ranges (IQRs) or means as appropriate. Baseline characteristics according to the debridement technique (TA versus SS) were compared using the Student t-test, the Pearson χ2 test, or the Kruskal Wallis test, as appropriate.
The relations between debridement technique (TA or SS) and post-operative outcomes were examined. For continuous outcomes, estimated mean differences and 95% confidence intervals (CIs) were calculated using multiple linear regression with robust standard errors. For categorical outcomes, relative risk (RR) and 95% CI were calculated using Poisson regression with robust standard errors. The exposure of interest in all models was treatment with the SS approach, and outcomes were as detailed in the above paragraphs. Age, diabetes mellitus status, debridement prior to transfer, Laboratory Risk Index for Necrotizing Fasciitis (LRINEC) score, and smoking status were co-factors to be included in the model. Smoking status was not available for 65% of the cohort and so was removed from the model.
Cohen's κ was used to assess inter-rater agreement on photograph-based wound closure estimates. Statistical significance was set at alpha <0.05. All statistical analyses were performed using Stata 15 (StataCorp., College Station, TX).
Results
From January 2012 through December 2016, 487 patients were treated for NSTI at Harborview Medical Center. The SS approach was introduced in late 2014 and had become standard practice by 2015. In total, 257 patients (52.8%) were in the SS cohort. The mean age of all NSTI patients was 51.7 years (±13.9 years), with no difference between the SS and TA cohorts (Table 1). Women comprised 37% (n = 179) of the overall and individual cohorts. The co-morbidities were similar in the two groups, except for smoking, diabetes mellitus, and chronic kidney failure, which were more common in the SS group. The underlying cause of infection also was similar for the two surgical approaches, with the majority of individuals having infections arising without preceding trauma or intravenous drug use (Table 1).
Baseline Characteristics and Co-Morbidities for Patients Admitted with Necrotizing Soft-Tissue Infection at a Level One Trauma Center between July 2012–December 2016
Continuous variables are presented as median (interquartile range) and categorical variables as n (percent). Percentages may not add to 100 because of missing values.
Percentages of the total number of TA or SS patients.
Intravenous or intramuscular injections.
Includes bites, pre-existing skin lesions, intra-abdominal infection, and peri-rectal abscesses.
COPD = chronic obstructive pulmonary disease; IQR = interquartile range; LNRINEC = Laboratory Risk Index Score for Necrotizing Soft Tissue Infections; SD = standard deviation.
Most patients (84.8%, n = 412) transferred from other hospitals. Transfers were more frequent in the SS cohort (89.1% versus 79.1%; p = 0.005). Similar numbers of patients underwent initial debridement at the referring hospitals (SS: n = 71/183; 38.8% versus TA: n = 86/240; 35.8%). Patients in both the SS and TA groups underwent a median of three debridements prior to reconstruction (p = 0.03).
Wound closure by skin grafting versus primary closure was analyzed via photographs or operative reports for 277 of the patients (56.9%). Of these, 200 patients (72.2%) had photographs available for analysis, whereas the rest were assessed from the operative reports alone. These patients were included in the primary analysis. Wound closure percentages estimated from pre-operative and post-operative photographs, which were evaluated by three independent surgeons, showed excellent inter-rater agreement.
Wound outcomes are improved by the SS debridement technique
The percentage of the wound closed by delayed primary surgery was available for 277 patients (TA 150; SS 127). In the SS group, local tissue rearrangement achieved a median of 50% (IQR 0–100%) wound closure compared with a median of 0 (IQR 0–26.7%) in the TA group (estimated mean difference +27.4%; 95% CI +19–+41; p < 0.0001) (Table 2). In contrast, skin grafting was used to achieve a median of 90% wound closure in the TA group compared with 20% in the SS group (IQR 0–100% in both groups; estimated mean difference -26.1%; 95% CI -10–-42; p = 0.002). The initial size of the debridement was documented for 247 patients in the operative reports. As expected, in the SS group, with 195 patients, the median initial debridement size (200 cm2; IQR 50–500 cm2) was smaller than in the TA group, with 52 patients (537.5 cm2; IQR 220–105 cm2) (p = 0.0001) (estimated mean difference -386 cm2; 95% CI -42–-729 cm2; p = 0.028). More TA patients than SS patients required secondary procedures after initial reconstruction, 31.3% (72/230) versus 21.4% (55/257). However, on adjusted analysis, the SS did not reduce the risk of needing a second reconstruction (RR 0.77; 95% CI 0.54–1.1; p = 0.15 (Table 3).
Primary Operative and Clinical Outcomes for Patients Admitted with Necrotizing Soft-Tissue Infection at a Level One Trauma Center between July 2012–November 2015d
Statistical significance was determined using multiple linear regression with robust standard errors, with models structured as follows: 1) exposure of interest: skin-sparing technique; 2) outcomes as listed above, 3) covariates included categorical variables for age, diabetes, debridement at outside facility, laboratory risk index score for necrotizing fasciitis (LRINEC) and smoking status. Data are presented as medians (inter-quartile ranges).
Average of estimated percentages from three independent surgeons assessing operative reports, pre-operative photographs, and post-operative photographs.
Autograft, xenograft, dermal template, or free flap.
CI = confidence interval; DPC = delayed primary closure; IQR = interquartile range.
Secondary Operative and Clinical Outcomes by Operative Approach (Traditional vs. Skin Sparing)
Statistical significance was determined using Poisson regression with robust standard errors, with models structured as follows: 1) exposure of interest: skin-sparing technique, 2) outcomes as listed above, 3) covariates included categorical variables for age, diabetes, debridement at outside facility, and Laboratory Risk Index Score for Necrotizing Fasciitis (LRINEC). Data are presented as number (percent).
Because of failed skin graft, flap loss, dehiscence of primary closure, or impaired function.
Autograft, xenograft, dermal template, or free flap.
Grade 1, 2, or 3.
ARDS = acute respiratory distress syndrome CI = confidence interval.
Skin-sparing debridement does not appear to increase the risk of complications
Mortality rates did not differ for the two approaches, SS 10.9% (n = 28) versus TA 12.6% (n = 29) (p = 0.4). Amputation data were available for 467 patients (95.9%). There was no difference in the rate for the SS (7.8%; 20/257) and TA (9.1%; 19/210) groups (p = 0.62). Ventilator-free days and hospital length of stay were similar in the SS and TA groups (Table 2). The incidence of new-onset acute renal failure was lower in the SS group, while ARDS and cardiac arrest data were similar in the two groups (Table 3).
Sensitivity analysis excluding patients having initial debridement at another institution
A sensitivity analysis including only the patients whose initial debridement(s) occurred at Harborview Medical Center was done, as physicians at other institutions were not trained in the SS method during the study period. This analysis included 69% of TA patients (159/230), and 70.8% of SS patients (182/257). In this group, a significantly larger portion of the SS patients' wounds were closed by delayed primary surgery, the estimated mean difference being +27.9% (95% CI 13.6–42.2; p < 0.001). The percent closed by grafting was similarly reduced, -26.7% (95% CI -42.9, 10.6; p = 0.001) for the SS approach when adjusted. Again, excluding patients with an initial debridement at another institution, the crude mortality rates did not differ in the TA (14.5%; 23/159) and SS patients (11.5%; 21/182) (p = 0.42), with the adjusted RR of in-hospital death for the SS group being 0.68 (95% CI 0.33–1.4; p = 0.29. In this subgroup, SS did not increase the risk of other complications, including need for reconstruction, length of stay, need for amputation, ventilator days, cardiac arrest, ARDS, or renal failure.
Discussion
Treatment of NSTI traditionally has included large, disfiguring debridements with complex and lengthy reconstructive courses. This large study is the first to demonstrate that using an SS technique for initial debridement, as described in our previous work [4], has a reconstructive advantage over the TA. The SS technique was associated with significantly smaller areas of grafting and higher rates of primary closure. The SS technique did not increase the mortality rate or risks of other post-operative complications compared with the TA.
The SS technique has several post-operative advantages over the TA. Overall skin grafting was significantly less extensive. A primary principle in reconstruction is to replace “like with like.” Although skin grafting does achieve ultimate closure of a wound, it does not have the same sensitivity, durability, or aesthetic appearance as native skin and subcutaneous tissue [12–14]. The SS approach allows preservation of native tissue whose quality simply cannot be entirely replaced. This can result in better overall reconstruction through delayed primary closure, local soft-tissue flap rearrangements, and smaller skin-grafted areas. Although there was not a statistical difference in the number of patients who required revision after reconstruction, we hypothesize that re-operation because of functional limitation was less in the SS group. Studies to determine the patient's motivating factors for re-operation are recommended to understand better the effect of NSTI course on the quality of life.
Although our current study did not evaluate post-operative quality of life directly, we hypothesize that the SS approach will lead to better social and physical functioning relative to the TA. Only a few studies have described the long-term followup and quality of life outcomes among patients with NSTI. One study evaluated functional limitation at the time of discharge, which demonstrated 30% of patients suffered from some degree of functional limitation; and involvement of the extremity was associated with a higher functional limitation [15]. Another study found that survivors were at continued risk of premature death after discharge compared with a control population [16]. A qualitative study used a patient-first method to understand better the patient recovery experience and found that reported quality of life was significantly affected by physical function-related reconstruction and by continuing pain [17]. To our knowledge, there are no published studies that identify the correlation between the extent of skin grafting and quality of life in the NSTI population.
The burn surgery literature provides some rationale for the SS technique for NSTI. A Norwegian group demonstrated that the presence of a full-thickness burn increases the risk of a negative impact on quality of life [18]. The same group completed a long-term study to 16 years after a burn and found, again, an association between the extent of full-thickness burn and domains of burn-specific and general quality of life [19]. Another study demonstrated that mobility and self-care was affected negatively in patients with >20% total body-surface area full-thickness burns [20]. The SS technique allows smaller areas of skin grafting, which, based on burn literature precedent, may have a positive impact on patients' long-term quality of life and function.
A key strength of this study is the large cohort of patients managed with modern critical care and its associated improved mortality rate. Despite this, there are several limitations of the study. First, this technique was not adopted uniformly by all surgeons at the same time, which may have attenuated the stated results in the early transition period. Second, when evaluating the percentage of closure, only one of the surgeons was blinded completely to outcomes, one surgeon was involved clinically with 10 patients, and the primary investigator cared for the majority of these patients. This may have led to bias in the estimated percentage of closure. However, strong inter-rater agreement among both blinded and unblinded surgeons suggests this effect was small. Despite the large cohort, the study was not powered to determine non-inferiority of the SS compared with TA on death or other complications. Our cohort indicates no differences, but adequately powered studies are needed to detect risk differences for these uncommon outcomes. Finally. we included all patients in the SS approach group if they presented in 2015 or 2016, including those whose initial debridement occurred prior to transfer to our hospital because management at out institution followed SS principles. Although these patients may have had initial debridements that affected their overall results, a sensitivity analysis done without these patients showed similar trends and significance for all primary and secondary outcomes. Furthermore, larger initial debridements would tend only to decrease the likelihood of a difference in each approach.
Conclusions
Using an SS approach, which minimizes initial resection of skin and subcutaneous tissue, decreases the need for skin grafting in patients with NSTI without increasing deaths or other post-operative complications. Future research on the surgical treatment and care model is needed to optimize patient treatment and recovery. This work must focus on patient-reported outcomes that can assess how to optimize long-term function and improve quality of life. The effect on hospital utilization and fiscal impact also can help guide initiation and adjustment of standards of care for these patients. Data collection on these points is continuing, and future publications on the topic are anticipated.
Acknowledgment
This material was presented at the 10th Annual Meeting of the Washington/Oregon State Chapter of the American College of Surgeons Meeting, Cle Elum, WA, June 2015, and the 60th Annual Plastic Surgery Research Council, Seattle, WA, May 2015.
Author Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors have no financial or commercial conflicts of interest to report.