
Abstract
Background:
Peri-prosthetic joint infection (PJI) is a major complication of knee arthroplasty that can cause long-term disability. In addition to its physical impact, there is a clear psychological burden that has not been measured yet. We hypothesized that the psychosocial burden of PJI can be assessed quantitatively using standardized questionnaires and may be correlated with treatment stage.
Methods:
Thirty-one patients were enrolled in this longitudinal prospective cohort study from August 2015 to November 2016. Participants had clinically established knee PJI after primary total knee replacement in osteoarthritis according to the Musculoskeletal Infection Society criteria and underwent a standardized two-stage protocol. After explantation of the prosthesis and implantation of a polymethylmethacrylate knee spacer, patients were treated with organism-specific intravenous antibiotics for two weeks, followed by oral antibiotics for four weeks; and then reimplantation was performed in all cases. Psychometrically validated standardized questionnaires were used to measure psychosocial stress via self-assessment at four time points: (1) Before explantation of the prosthesis; (2) after explantation; (3) after the antibiotic treatment before reimplantation; and (4) three months after reimplantation (follow-up). The Patient Health Questionnaire (PHQ)-4, Short Form (SF)-12 (including PSK and KSK), Questions about Life Satisfaction (FLZM) and Fear of Progression (PA-F-KF) (titles and abbreviations in German) scores were interpreted according to cut-off values for depression, fear of progression, anxiety, and quality of life.
Results:
Eighteen patients (58.1%) showed a PHQ-4 score above the cut-off value for depression at least once, with the highest score before reimplantation (time point 3). On the SF-12, the mean subtest mental scale (PSK) score was 42.6 (± 14.5), and the mean subtest physical scale (KSK) score was 26.9 (± 7.5) over the four time points, which was significantly lower than that of the general German population (PSK 53.1, KSK 44.0; p < 0.05). The SF-12 scores did not change significantly over time. On the FLZ, health was least satisfactory, followed by recreational activities and work. On the PA-F-KF, patients had the greatest fear of being dependent on outside help, drastic medical interventions, and infection progression. The mean PA-F-KF value was 31.24 (± 9.60; values ≥34 are regarded as critical).
Conclusion:
Peri-prosthetic joint infection is a measurable, relevant psychosocial stressor for patients. Their quality of life and fear of the disease progressing are comparable to those of oncology patients. Routine screening should be conducted to identify affected patients early for appropriate treatment, improving long-term outcomes. Orthopaedic surgeons who treat patients with PJI should initiate by psychologists as well in order to maintain the patient's long-term quality of life.
Osteoarthritis of the knee is a disease with a significant and rising incidence, especially because of the aging populations in modern industrialized countries. Currently, total knee arthroplasty (TKA) remains the only curative therapy. Therefore, the total number of TKAs performed is rising in the United States and Europe. Recent studies predicted a 600% increase in the number of TKAs being performed by 2030 [1].
The number of revision arthroplasties also is projected to increase in proportion to the number of primary TKAs. One common reason for revision arthroplasty is peri-prosthetic joint infection (PJI). In North America and Europe, a two-stage revision protocol is considered the gold standard for chronic infection eradication [2–5]. This protocol involves the explantation of the prosthesis and the implantation of an antibiotic-loaded cement spacer for an interval of two–six weeks before implantation of a new prosthesis. This process causes a period of poor joint function and disability for the patient that is accompanied by high doses of intravenous or oral antibiotics, possibly with adverse effects. Despite its drawbacks, this protocol enables control of the infection in 80%–100% of patients [6,7].
Less is known about the impact of PJI and the two-stage treatment protocol on the patients and their social environment. In this context, Zmistowski et al. demonstrated a higher mortality rate for patients undergoing surgical intervention because of PJI compared with those having aseptic revision surgery. Furthermore, the five-year mortality rate of patients suffering from PJI is 26% [8]. Thus, PJI has a higher mortality rate than thyroid, prostate, and breast cancer [9].
Because of the relatively high mortality rate, approximately 30%–60% of all cancer patients suffer from psychosocial distress during the course of their disease, which poses a relevant clinical and economic problem [10–12]. Many studies have addressed psychosocial parameters such as health-related quality of life, depression and anxiety, or aspects of satisfaction with life experienced by patients suffering from malignant diseases.
According to a register study from Damkjaer et al., breast cancer causes considerable unemployment for patients, with a higher rate of early retirement causing economic losses for the families and from an overall societal standpoint [13]. Even if returning to work is possible, a sum of problems such as physical and mental fatigue, depression, and reduction of quality of life cause a significant reduction of productivity and increase of psychosomatic/ mental health issues [14,15]. An intervention aimed at individual physical, mental, and social functioning in the initial phase of the disease improves these issues significantly [13].
Surgical site infections (SSI) such as PJI are assumed to cause similar situations. Gelhorn et al. postulated that patients have low awareness of the consequences of SSIs. Apart from the impact on everyday life, psychological and social functioning and a significant economic burden are underestimated problems of PJI [16–18].
In contrast to patients suffering from PJI, adjuvant psychological treatment options are offered on a regular basis to patients during cancer therapy to support recovery and successful coping with related social problems such as unemployment or family difficulties [19–25]. The treatment of PJI, however, is still focused mainly on the biomedical aspects, although high psychosocial distress levels should be expected in these patients. This is an important issue because psychosocial distress occurs during PJI therapy, and thus the authors hypothesized that adding psychological treatment may produce better clinical results in the long run. So far, there have been no prospective studies on this problem. We therefore asked the following study questions:
Is there a relevant psychosocial burden on patients suffering from PJI that indicates a need for psychological treatment during and after therapy? Is the psychosocial burden comparable to that experienced by patients suffering from malignant disease? Is the satisfaction with life of patients with PJI reduced compared with that of the general population and of those with malignant disease?
Patients and Methods
The approval of the Institutional Review Board was obtained before initiation of the study (Ethics Committee of the Faculty of Medicine, Technical University Munich, Number 407/15F). All patients undergoing a two-stage surgical treatment for PJI of the knee joint in our institution from August 2015 to November 2016 were enrolled prospectively, and written consent was obtained from each subject prior to enrollment. Patients were included irrespective of age (> 18 years), gender, and co-morbidities. All patients had a PJI according to the Musculoskeletal Infection Society (MSIS) criteria [26]. Patients with a neuropsychiatric disease were excluded. All patients were treated using a two-stage protocol, which means that after explantation of the prosthesis and implantation of a multi-part articulating polymethylmethacrylate knee spacer, patients were treated with organism-specific intravenous antibiotics for two weeks, followed by oral antibiotics for four weeks. Reimplantation was performed in all cases after six weeks, there being no evidence of persistent infection at the time of reimplantation (normal clinical and laboratory findings). All patients had a medial parapatellar approach.
Established and psychometrically validated self-assessment questionnaires were used to screen for psychosocial stress (Table 1). We used the PHQ-4, the SF-12 (short version of the SF-36 as a measurement instrument for the assessment of health-related quality of life [27]), the FLZ Herschbach & Henrich, and the PA-F-KF [28,29]. The patients received the four self-assessment questionnaires at four time points during their therapy. In detail, the PHQ-4 Questionnaire is a combination of the short version of the PHQ-2, one of the best-validated screening tools for depression, and the Generalized Anxiety Disorder (GAD)-2, which has good validity for the detection of the four most common anxiety disorders according to Kroenke et al. (2009 [30].)
Time Points of Treatment and Questionnaire Completion by Patient
The SF-12 is the short form of the SF-36 Health Questionnaire and is a measurement tool used to assess health-related quality of life. It consists of twelve questions on physical and role functioning, pain, general health perception, vitality, and social functioning in terms of emotional and psychological well-being. These items can be calculated by weighting the physical (KSK) and psychological (PSK) sum scales (the titles and abbreviations are in German). The SF-12 can be used for patients with diverse diseases or those with a specific disease. Increasing values over time indicate improving health. A score of 50 is the average in a population-based sample (possible range 20–80).
The FLZ test aims to capture the relevant aspects of satisfaction in eight areas of life (friends/leisure, hobbies/health/income, financial security/work, occupation/housing/family life, children/partnership, and sexuality [31]. The module on health-related quality of life examines the relevant areas of physical and mental health (performance, ability to relax, energy/joy in life, ability to move, sight and hearing, freedom from fear, absence of pain and suffering, and independence from help and care). First, the participant is asked for her or his subjective view of the importance of each item and rates it on a five-level response scale from “not important” to “extremely important.” Afterward, the levels of satisfaction in these individual areas of life are rated from “dissatisfied” to “very satisfied.” For the evaluation, the mean value of the eight unweighted items is calculated, and an individually adjusted value for the weighted satisfaction is calculated according to the subjective importance perceived by the individual. The content values of the items are linked to the importance values. The sum value for each module is added (range −96 to 160 per module, worst weighted to best weighted quality of life).
The PA-F-KF is the short form of the progressive anxiety questionnaire, a self-assessment tool used to screen for stress in patients with progressive anxiety (affective responses, partnership, job, loss of autonomy, and anxiety management; Mehnert et al. [32]). This questionnaire consists of 12 items of the original 43 on the long form, which are answered on a five-point scale from “never” to “very often.” The short form has been validated in large samples of patients with cancer. For evaluation, the individual values are added, resulting in a range of 12–60, with values ≥34 regarded as critical. An infected prosthesis may result in limitations being imposed on patients similar to those experienced by patients with cancer (prolonged hospitalization, intravenous antibiotic therapy, and loss of physical integrity and self-reliance); therefore, this study first used a questionnaire designed primarily for patients with cancer.
The questionnaire data were analysed descriptively and are reported as the means, standard deviations (SDs), minimums, maximums, and 95% confidence intervals (CIs) for the metric scaled variables. The absolute and relative frequencies and 95% CIs were calculated for the nominally scaled variables. A p value of 0.05 was assumed to be statistically significant. In addition, the frequency distributions of the different values at each time point were calculated and compared. Statistical analysis was performed using IBM SPSS Statistics 25 (IBM, Armonk, NY USA) and Microsoft Excel 2016 (Microsoft, Redmond, WA USA).
Results
Thirty one patients (male/female = 16/15) with a median age of 69 years (range 42–85 years) at the time of diagnosis of PJI were included.
PHQ-4 Questionnaire
The published cut-off value for the PHQ-4 as a screening tool for depression (PHQ-2) and anxiety disorders (GAD-2) is ≥6. In this study, 18 patients (58.1%) reached this cut-off value at least once. Four patients (12.9%) had the maximum value of 12 at least once, and 14 (77.8% of all patients, who reached the cut-off value at least once and 45.2% of all participants) achieved a value ≥6 at one time point. Five patients achieved scores of ≥6 at two points. The mean value and SD of the 55 questionnaires distributed over all four time points was 5.27 ± 3.77, with slightly better values for males (4.72 ± 3.59) than females (5.88 ± 3.93). The mean values for each of the four time points showed that the highest value occurred at time point 3 (Fig. 1).
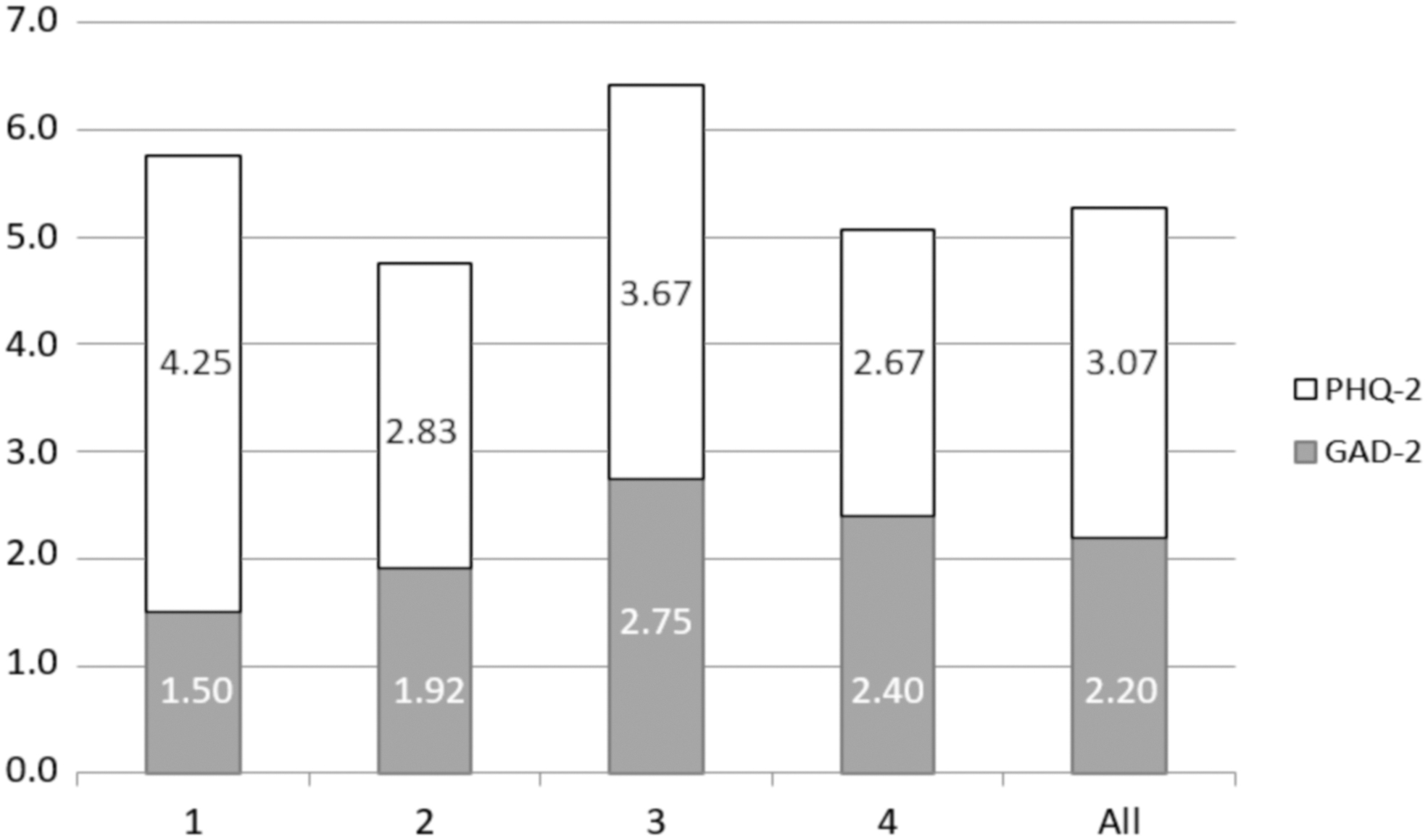
Mean value of PHQ 4 scores over all four time points (x axis = time points as detailed in Table 1 and as the mean of all four time points; y axis = patient values; cut-off value 6).
SF-12 Questionnaire
The mean scores of the SF-12 Questionnaire were 26.88 ± 7.47 for the KSK and 42.60 ± 14.54 for the PSK. Male and female participants achieved similar scores, although females had slightly worse scores on the KSK (28.54 ± 8.12 versus 25.22 ± 6.50) and the PSK (43.99 ± 14.52 versus 41.20 ± 14.70). The mean values did not change significantly over the four time points (Fig. 2). The SF-12 was significantly lower than that of the German population (p < 0.05; Table 2).
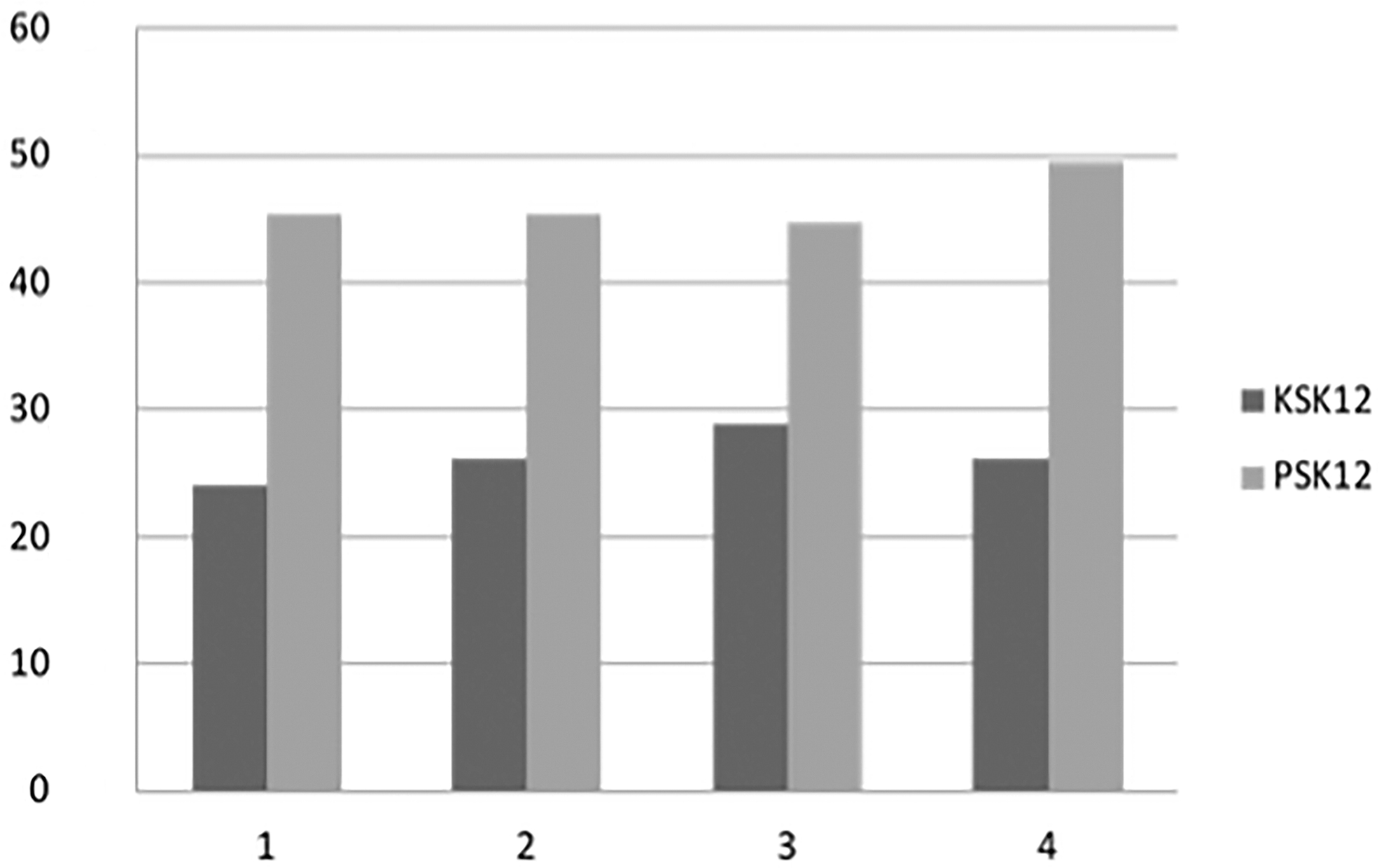
Mean value of SF-12 (KSK+PSK) over all four time points (x axis = time points as detailed in Table 1; y axis = patient values; KSK: physical sum scale; PSK: psychological sum scale).
P Value Results of SF-12, PHQ-4, and FLZ Questionnaires
Values are mean over four time points correlated with German norm determined by authors from respective questionnaires on basis of a different number of patients as published by authors [28–32].
CI = confidence interval; GLS = General Life Satisfaction; HLS = Health Life Satisfaction; PJI = peri-prosthetic joint infection.
FLZM Questionnaire
The values of the patients were almost identical over the four time points. For this reason, the mean values at all four times are shown in Figures 3–5. For both the unweighted and weighted scores, participants had the lowest level of satisfaction regarding health, followed by recreational activities and work. Participants were most satisfied with their family life/children and housing situations (Fig. 3). Within the category of health, the participants had low unweighted and weighted satisfaction scores for their ability to move, physical performance, and independence from help and care (Figs. 4 and 5). The question “How satisfied are you overall with your life when you put all aspects together?” showed that 70% of the participants were dissatisfied (Fig. 6).
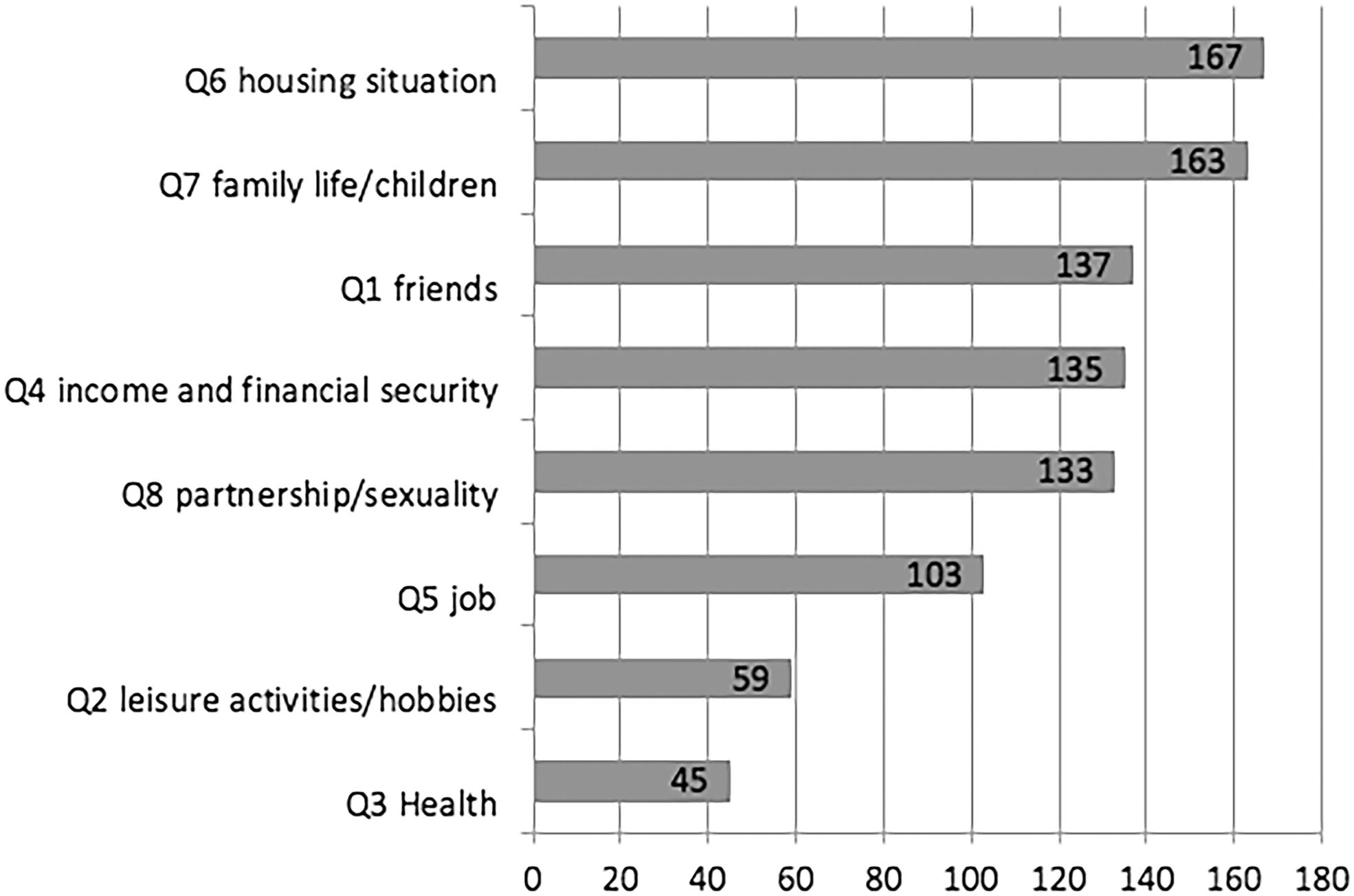
Cumulative score of all patients: General life satisfaction-unweighted (FLZM) questionnaire (x axis = patient values, y axis = items of the questionnaire).
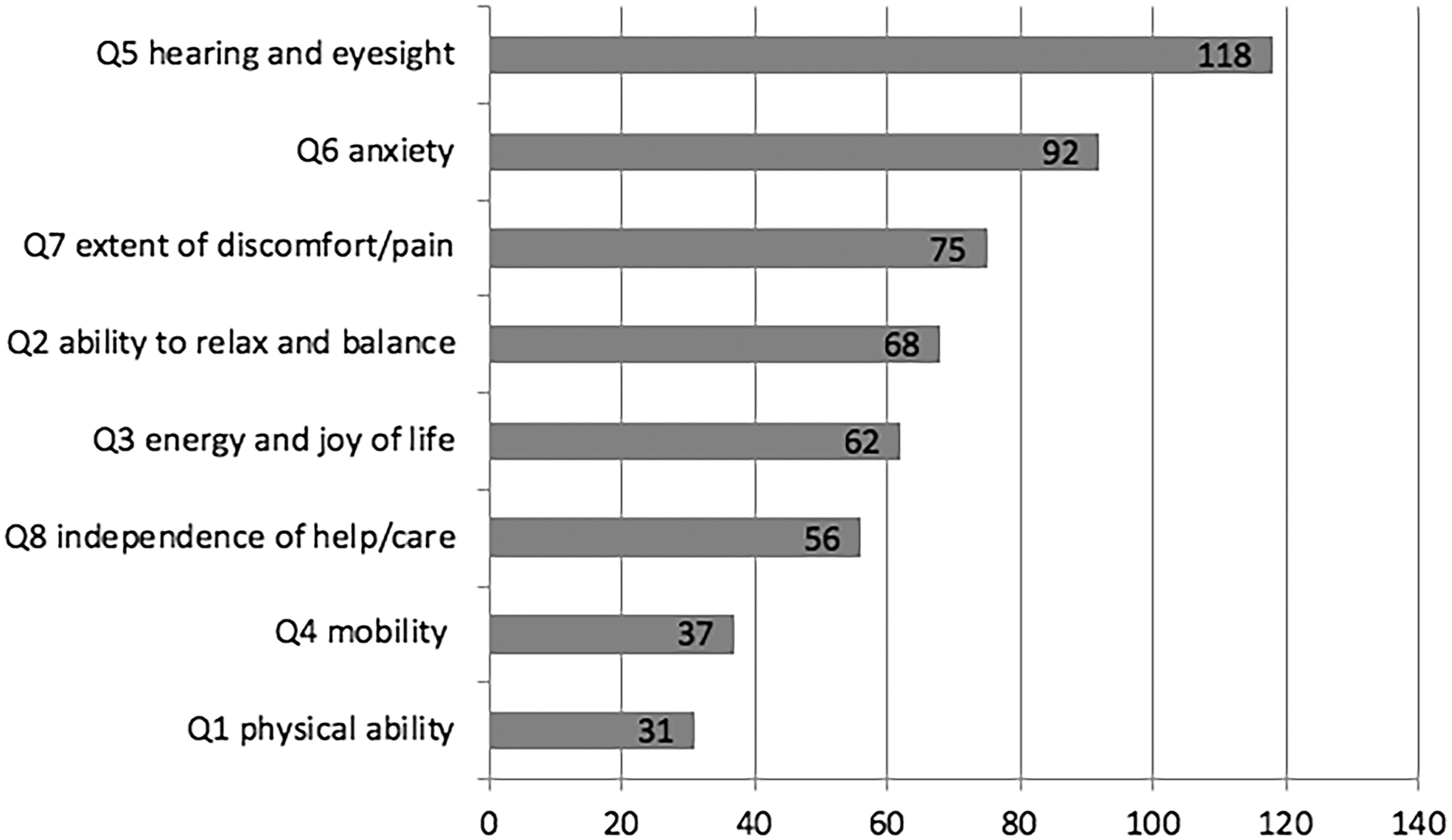
Cumulative score of all patients: satisfaction with health-unweighted (FLZM) questionnaire (x axis = patient values unweighted, y axis = items of questionnaire).
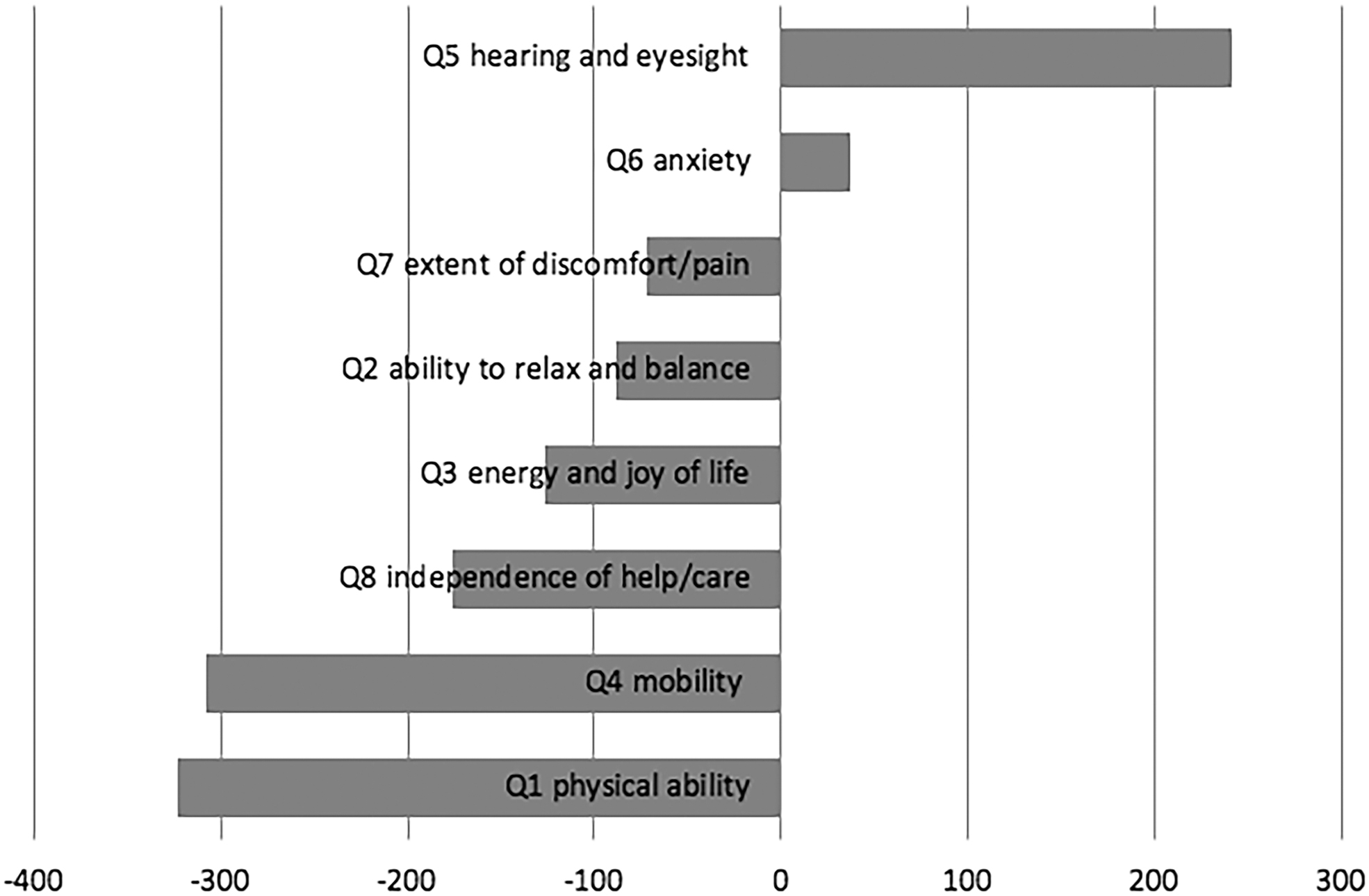
Cumulative score of all patients: Satisfaction with health-weighted (FLZM) questionnaire (x axis = patient values weighted, y axis = items of questionnaire).
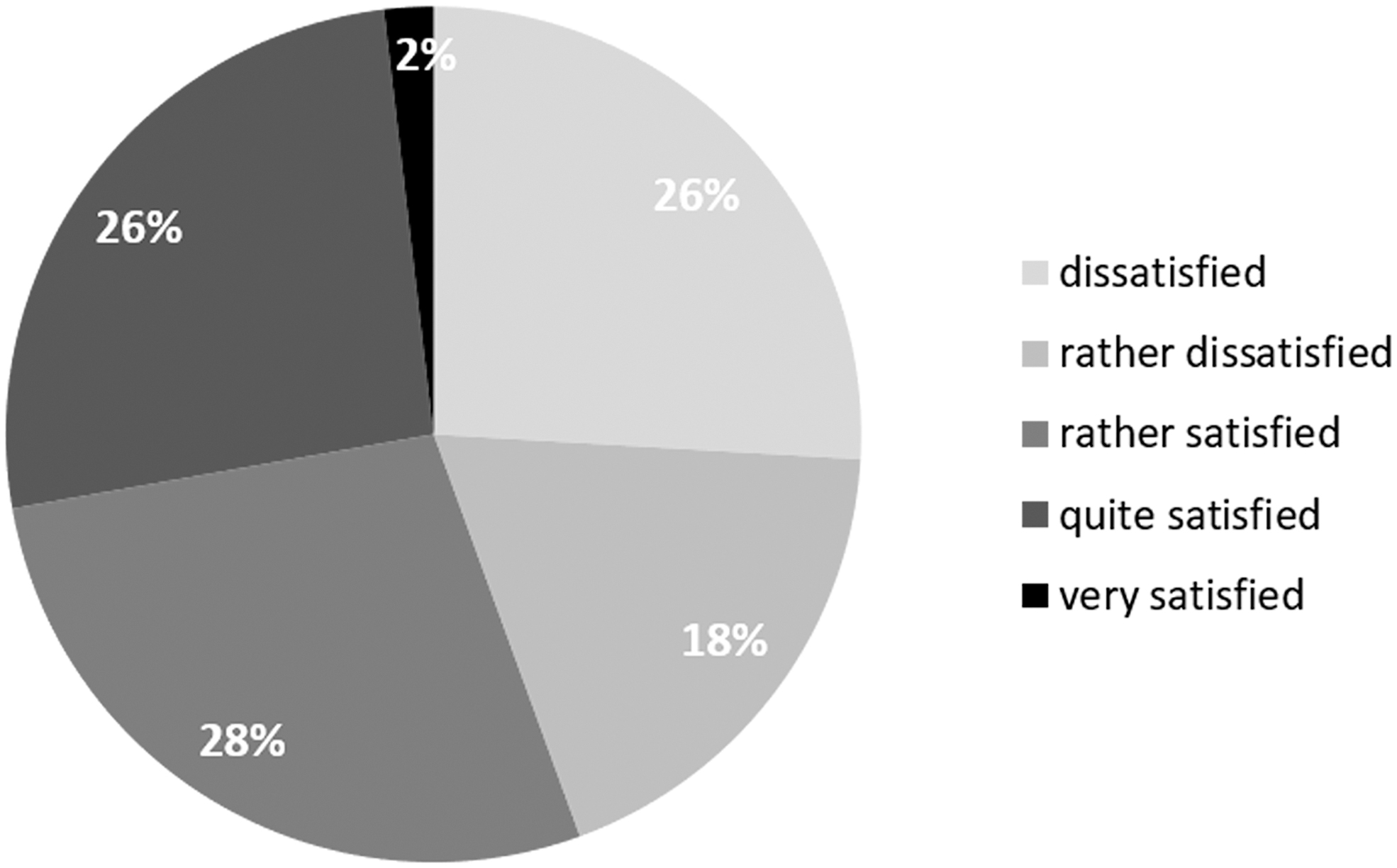
General satisfaction (percentage of patients).
PA-F-KF Questionnaire
As with the FLZM questionnaire, the values reported by the patients over the four time points were almost identical. For this reason, the mean values over time are shown in Figure 7. The mean score of the PA-F-KF questionnaire was 31.24 ± 9.60. Male and female participants achieved similar scores (31.90 ± 9.32 versus 30.50 ± 10.02). Patients are most afraid of being dependent on outside help, of drastic medical interventions (leg amputation), of drugs, and of the further course of the infection.
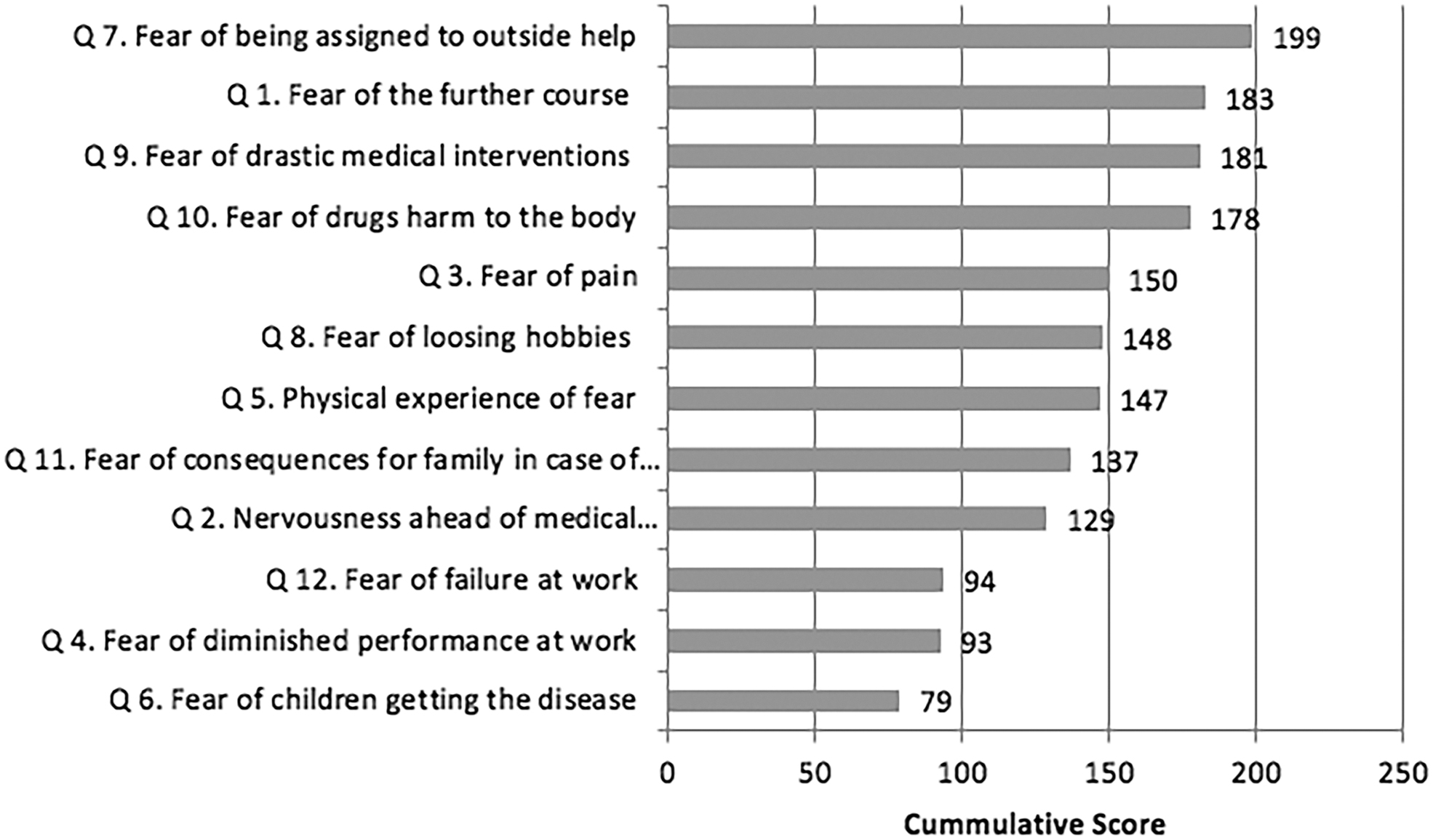
Cumulative score of all patients on PA-F-KF: Fear of progression (x axis = patient values, y axis = items of questionnaire).
Discussion
The two-stage protocol commonly is regarded as the gold standard for the treatment of chronic PJIs, being considered the most effective strategy for infection eradication and preservation of joint function [4]. Its success rate differs in the literature [33,34], but a meta-analysis reported successful treatment was achieved in 89% of patients. However, studies concerning the psychosocial burden of patients with PJIs are rare and difficult to compare. To the best of our knowledge, this is the only prospective study that reports on psychosocial distress in patients with PJI with a defined timeline during a two-stage protocol. This is an important issue because psychosocial distress occurs during PJI therapy, and thus the authors hypothesized that addition of psychological treatment may facilitate better clinical results in the long run. A previous study by Helwig et al. used a retrospective telephone survey to screen patients using the SF-12 Questionnaire to determine their long-term life quality. However, some patients were evaluated years after they underwent a two-stage PJI protocol [35]. Two independent working groups led by Cahill et al. and Kappler et al. also reported on the quality of life of patients after PJI; their surveys were similar to the study by Helwig et al., performed between one and three years after the disease, leading to underestimation of the extent of psychosocial distress during PJI treatment [28,29,36]. Although still being underrated in orthopaedic surgery, in oncologic treatment, an interdisciplinary approach is considered to be standard in the United States and Europe, involving surgeons, oncologists, and psychologists in the therapeutic process [11]. Our study showed that patients with PJI experience psychosocial distress during the important weeks of therapy, which are characterized by poor physical functioning and sometimes confinement to bed, accompanied by the administration of strong antibiotic medication. Answering our first question, the PHQ-4 Questionnaire, which focuses on depression and anxiety disorders, indicated a high level of distress in our cohort. Although the PHQ-4 is an ultra-brief measure, the results are reliable and valid for diagnosing depression and anxiety [37]. Half our cohort scored above the cut-off level at least once during therapy, indicating the considerable relevance of the problem. Comparing our results with those of cancer patients, Renovanz et al. reported in a cohort of patients with intra-cranial tumors just 23% with a relevant cut-off >6. Pompe et al. postulate an even lower percentage of 8%> 6 in a cohort of 5,862 patients after radical prostatectomy [38,39].
Several evidence-based treatment guidelines provide recommendations regarding treatment options for these patients [33]. In addition, the stepped care principle for depression and anxiety disorders could be applied to these patients [37]. Our working group is the first to articulate the need for depression and anxiety distress treatment and, ideally, prophylaxis during PJI treatment.
Our patient cohort's physical score (26 points) was significantly lower than those of the general population and patients undergoing aseptic revision arthroplasty [34]. The mental score of our cohort (46 points) was reduced, although not significantly, compared with that of the general population. We confirmed the findings of the groups of Helwig et al. and Romano et al., who reported a lower physical score than mental score with the SF-12 tool. Our cohort showed significantly lower physical scores than in other cohorts at all times. This can be explained by the different study designs. As mentioned above, all other studies had retrospective designs and performed the screening a long time after the hospital stay. One can assume there were similarly low scores in their cohort at our points of time [29,33]. Our findings also confirm those of Wang et al., who compared the SF-12 scores of patients with septic and aseptic revisions and detected both lower physical scores and lower mental scores in patients undergoing septic revisions [4]. Another working group compared the quality of life of patients undergoing uncomplicated primary arthroplasty with that of patients undergoing revision arthroplasty because of infection and demonstrated poor quality of life scores in the latter group [40].
One main problem in the treatment of PJI is the cut-off period after which patients are presumed to be cured. Even after 20 months without signs of infection, recurrence of the infection is possible. In the literature, a period of 24 months is accepted for long-term infection control [5]. In this context especially, the fear of recurrence causes psychological distress in patients. Therefore, progression anxiety was an important subject in our investigation. With a mean score of 31.24 on the PA-F-KF, our cohort had slightly lower scores than those of patients after mastectomy for breast cancer. A study by Jendrian et al. addresses the quality of life after mastectomy versus breast-conserving treatment. Using the PA-F-KF, the authors report a fear of progression of 31.54 ± 10.6 in the mastectomy group and 28.54 ± 8.64 in the breast-conserving group [41].
According to Dinkel et al., fear of progression is one of the most frequent causes of distress in patients with cancer and other chronic diseases [42]. This fear can become overwhelming, affecting well-being, quality of life, and social functioning.
A standardized tool to measure quality of life in terms of life satisfaction is the FLZ Questionnaire. This questionnaire examines many aspects of daily life such as housing, friends, and family; recreational activities/hobbies; and work. For both the unweighted and weighted scores, participants in our study had the lowest level of satisfaction regarding health, followed by recreational activities and work. Large studies have shown that life satisfaction is a multi-factorial issue that cannot be reduced to health and physical well-being alone. In addition, other psychological factors play an important role. In particular, impaired mobility and physical ability as well as the fear of needing help from others seems to correlate with a significant decrease in life satisfaction. Interestingly, our cohort had no fear of loss of income or financial security, which might be a result of the German health insurance system and the age of the mostly retired patients.
The limitations of our study are the lack of follow-up data and of a cohort that included patients undergoing aseptic revision arthroplasty. Thus, a second study is planned to analyze the quality of life and the psychological burden on our cohort in the future. Further limitations of the study result from the individual assessment and course of PJI and different progressions of the infection in each person in the long-term course. Several studies have addressed quality of life with the SF-12 screening tool in patients undergoing aseptic revisions; these data can be used as a control group even if they are not perfectly matched and lack data from the PHQ-4, FLZ, and PAF-Q Questionnaires.
In conclusion, in a relevant number of patients, PJI causes depression and anxiety that needs to be addressed with psychological treatment. Furthermore, the quality of life, life satisfaction, and progression anxiety of patients with PJI are comparable to those of patients with malignant diseases. There is an urgent need for routine screening of patients with PJIs so that psychological treatment, if necessary, can be initiated as early as possible in order to facilitate better long-term results. Orthopaedic surgeons who treat patients with PJI should initiate care by psychologists in order to maintain the patient's quality of life in the long term.
Footnotes
Funding Information
This study was not supported by outside funding.
Author Disclosure Statement
All authors declare that they have no competing financial interests.