
Abstract
Background:
The relation between deresuscitative fluid management after the resuscitation phase and clinical outcome in patients with abdominal sepsis is not completely clear. The aim of this study was to assess the contribution of deresuscitative management to death and organ dysfunction in abdominal sepsis.
Methods:
Consecutive patients with abdominal sepsis requiring fluid resuscitation were included in this study. According to the fluid management given in the later stage of resuscitation, a conservative group and a deresuscitative fluid management group were compared. The primary outcome was in-hospital death, whereas secondary outcomes were categorized as organ dysfunction and other adverse events.
Results:
A total of 138 patients were enrolled in this study. Conservative fluid management was given to 47.8% of patients, whereas deresuscitative fluid management occurred in 52.2%. The deresuscitative strategy was associated with a markedly lower prevalence of new-onset acute kidney injury and a decrease in the duration of continuous renal replacement therapy (CRRT). There was a greater risk of needing new-onset intubation and the mechanical ventilation duration in the conservative group than in the deresuscitative group. However, the deresuscitative group did not differ from the conservative group with respect to open abdomen and intra-abdominal hypertension or new-onset abdominal compartment syndrome. The conservative treatment was associated with prolonged stays as well as a higher in-hospital mortality rate. A multivariable logistic regression model showed that deresuscitative fluid management imparts a protective effect against in-hospital death (odds ratio 4.343; 95% confidence interva1 1.466–12.866; p = 0.008), whereas septic shock, source control failure, and CRRT duration were associated with a higher mortality rate.
Conclusions:
Fluid balance achieved using deresuscitative treatment is correlated with better outcomes in patients with abdominal sepsis, indicating that this treatment may be useful as a therapeutic strategy.
Intra-abdominal infection (IAI) is one of the most important forms of sepsis [1]. It is a significant cause of death, with a mortality rate as high as 35%. Multiple factors influence the prognosis, including organ damage, antibiotic use, nutritional support, uncontrollable infections, and fluid accumulation [2–4]. Fluid therapy is employed extensively to optimize tissue perfusion in various critical states such as sepsis and is supported by international guidelines. Other than resuscitation fluid boluses, large volumes of fluid also are administered for nutrition, fluid maintenance, and as a drug diluent [5]. Given endocrine influences and acute kidney injury (AKI) that predispose to fluid retention, patients often accumulate a positive fluid balance (FB). The correlation between a positive FB and death in various critical illnesses has been well established [6,7].
Abdominal sepsis aggravates water–electrolyte imbalance; the fluid accumulates in the third gap and leads to abdominal cavity syndrome [8]. The current goal-directed fluid resuscitation strategy has been studied extensively, and the sepsis guidelines emphasize that resuscitation should be completed within one hour, and the fluid input is 50 mL per kilogram per hour. Rapid administration of a bolus of this size is associated with an increased risk of pulmonary edema and need for mechanical ventilation (MV). Fluid overload (FO) is a well-recognized adverse effect of fluid resuscitation [9]. After stabilization of shock, restricting maintenance and targeted deresuscitation using diuretics and renal replacement therapies improves clinical outcomes [10]. Moreover, the practice of deresuscitation after fluid-based hemodynamic stabilization should be investigated further.
Goal-directed resuscitation has emerged as the standard of care; however, this procedure brings us only halfway through the course [11]. Although vasoactive medications may be a useful component of resuscitation, they also generate various adverse physiological consequences. When a patient attains hemodynamic stability, “deresuscitation” must be performed; i.e., weaning of pharmacologic and mechanical support [12]. However, the most appropriate technique for deresuscitation has not yet been established. A conservative or deresuscitative method (application of diuretics or renal replacement regimen to remove accumulated fluid) for fluid management in critical states perhaps is beneficial, but the supporting evidence is insufficient.
Our previous studies have shown that excessive fluid is associated with a poorer prognosis for patients with IAIs [13]. A recent study showed that restrictive fluid resuscitation improves the timely recovery of homeostasis balance after resuscitation, maintains water–electrolyte balance, and restores the pathophysiological environment of the body [14]. However, the effect of this strategy is unclear. There are a few studies that require further in-depth investigation, particularly in patients with IAIs.
Deresuscitation is targeted fluid removal after stabilization of shock [15]. Restricting maintenance fluids and targeted fluid removal decrease the duration of MV and length of stay (LOS) in the intensive care unit (ICU). Diuretics and renal replacement therapies targeting negative FB are the main strategies for deresuscitation. The triggers to initiate these therapies after shock stabilization are an FO percentage >10% and the absence of fluid responsiveness using various dynamic measures [16].
The goal of this study was to assess the impact of deresuscitation on patient outcome after fluid resuscitation in abdominal sepsis, especially the occurrence of adverse events such as organ dysfunction and damage. Although there is some evidence of the importance of FO, whether this damage alone is sufficient to cause death is unclear. When insufficient fluid input is considered deleterious because of worsening cardiac output, excessive fluid input may generate tissue edema, which results in further complications. A growing number of studies have revealed the positive effects of a personalized, goal-directed hemodynamic scheme based on cardiac output monitoring. Herein, we postulate that deresuscitative management improves survival and reduces organ injury in patients with abdominal sepsis.
Patients and Methods
Study population and design
Patients who were found to have abdominal sepsis at the Research Institute of General Surgery of the Jinling Hospital, Nanjing Medical University in China from January 2016 to January 2018 were identified prospectively in the Abdominal Sepsis Center database. This research was approved by the Ethics Committee of Jinling Hospital. Eligible patients were selected, and they provided their written informed consent for participation prior to the start of the study.
The enrolled patients fulfilled the following inclusion criteria: (1) Age 18–60 years; (2) having abdominal sepsis diagnosed on the basis of clinical features, radiologic and microbiology assessment, or intra-operative findings; (3) underwent fluid therapy for resuscitation during the acute phase of the critical illness; and (4) were not treated with any concomitant medications (e.g., prednisone, methylprednisolone, dexamethasone, hydrocortisone, indomethacin, phenylbutazone, rofecoxib, or broad immune modulators). We excluded findings centered on the resuscitation phase of critical illness, as well as patients who died within 48 hours. We also excluded patients with primary cardiac insufficiency.
All patients underwent standard care following the Surviving Sepsis Campaign guidelines [17] as well as the Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infections [18,19]. The standard protocol comprised an expeditious diagnosis, initial patient resuscitation, source control, then antimicrobial therapy. We collected patient data such as primary diagnosis, sex, age, Body Mass Index (BMI), Acute Physiology, Age, and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores, extra-corporeal life support use, change of fluid volume, LOS, and in-hospital death.
Definition
In our hospital, patients assigned to the deresuscitation group underwent fluid removal using diuretics or continuous renal replacement therapy (CRRT), as well as restricted liquid management to achieve a negative FB after stabilization of shock. Source control failure was defined as progressive organ dysfunction within the first 24–48 hours after source control if there was no clinical improvement in organ dysfunction 48 hours or more after source control or if there were persistent signs of inflammation five to seven days after source control [19]. Daily fluid accumulation was defined as the daily total input (i.e., intravenous fluids, nutrition, medications) minus total output (e.g., urine, ultrafiltrate, and fluid from surgical drains) as recorded using nursing care and computer software. Cumulative fluid accumulation over a specific period of time was computed as the total fluid input minus the total output during that period. Acute kidney injury was defined according to the risk, injury, failure, loss, and classification of end-stage renal failure (RIFLE) in renal dysfunction [20]. Abdominal compartment syndrome (ACS) and intra-abdominal hypertension (IAH) were designated as defined previously [21].
Outcome measures
The primary outcome was in-hospital death. The secondary outcomes were ICU LOS, incidence of new-onset organ dysfunction, MV and CRRT use and duration, and new-onset intubation. We also focused on the special complications in abdominal sepsis similar to that in open abdomen and ACS or IAH.
Statistical analysis
All analyses were conducted using SPSS 22.0 (IBM Corp, Armonk, NY, USA). We compared proportions using the means of the χ2 test or Fisher exact test, whereas continuous variables were compared using means of unpaired t-tests. We examined the in-hospital survival with Kaplan-Meier curves and compared survival in patients with and without deresuscitative fluid management with the log-rank test.
Multivariable logistic regression models were constructed for in-hospital death. A two-sided p value of <0.05 was deemed statistically significant. Univariable and multivariable associations were expressed as odds ratios (ORs) with 95% confidence intervals (CIs).
Results
Study population
This study assessed 138 eligible patients with baseline characteristics presented in Table 1. Deresuscitative treatment was used in 72 patients (52.2%). The majority of patients (79.0%; n = 109) were male. Trauma was the main primary disease (42.0%; n = 58). Source control failure was present in the overwhelming majority of cases. Patients had an average of 4.9 days of FO. The two groups showed similarities in sex, age, baseline BMI, APACHE scores, SOFA scores, co-morbidities, and types of primary disease. Similarly, septic shock, source control failure, AKI diagnosis, and support of MV showed no differences between the groups. In contrast, the duration of FO showed an increasing trend in the deresuscitative group compared with the conservative group (5.2 versus 4.5 days), but the difference was not statistically significant.
Clinical Variables by Fluid Management Status
AKI = acute kidney injury; APACHE II = Acute Physiology and Chronic Health Evaluation II; CRRT = continuous renal replacement therapy; FO = fluid overload; MV, mechanical ventilation; SAP, severe acute pancreatitis; SD = standard deviation; SOFA = Sequential Organ Failure Assessment.
Clinical outcomes between different types of fluid management status
In-hospital death occurred in 31 patients (22.5%). A significant difference was observed in the in-hospital mortality rate in the deresuscitative and conservative treatment groups (8.3% versus 37.9%; p < 0.001). The deresuscitative strategy was correlated with a significantly lower incidence of new-onset AKI and a decrease in CRRT duration (Table 2). There was a greater risk of new-onset intubation in the conservative treatment group compared with the deresuscitative group. However, the deresuscitative group did not differ with respect to open abdomen (achieved fascia closure, new-onset fistulae) or in new-onset ACS or IAH.
Clinical Outcomes According to Fluid Management
ACS = abdominal compartment syndrome; AKI = acute kidney injury; CRRT = continuous renal replacement therapy; IAH = intra-abdominal hypertension; ICU = intensive care unit; LOS = length of stay; MV = mechanical ventilation.
Comparison between the deresuscitative and conservative groups revealed a mean ICU LOS of 27.2 days versus 42.4 days, respectively (p = 0.013), and the mean hospital LOS was 57.8 days versus 82.2 days, respectively (p = 0.001). Kaplan–Meier survival analysis showed a significant difference in the in-hospital survival between patients with deresuscitative and conservative therapy (log rank 11.035; p = 0.001) (Fig. 1).

Kaplan-Meier cumulative survival curves for patients with abdominal sepsis according to fluid management strategy. There was a significant difference in the survival rate in patients having deresuscitative vs. conservative therapy (log-rank test 11.035; p = 0.001).
Association between fluid management strategy and fluid volume
The mean daily FB and mean cumulative FB from days 1 to 7 are presented in Figure 2. The mean daily fluid input was significantly higher for the conservative than the deresuscitative group from days four to seven. However, the mean daily fluid output was significantly higher in the deresuscitative than conservative group from days 2 to 7. Daily fluid accumulation decreased rapidly from days two to seven with deresuscitative treatment. Mean cumulative fluid accumulation in the 72 patients in the deresuscitative group on day 3 was significantly lower than for those in the conservative treatment group (Fig. 2). This suggests that the deresuscitative group achieved early positive FB without increasing fluid input.
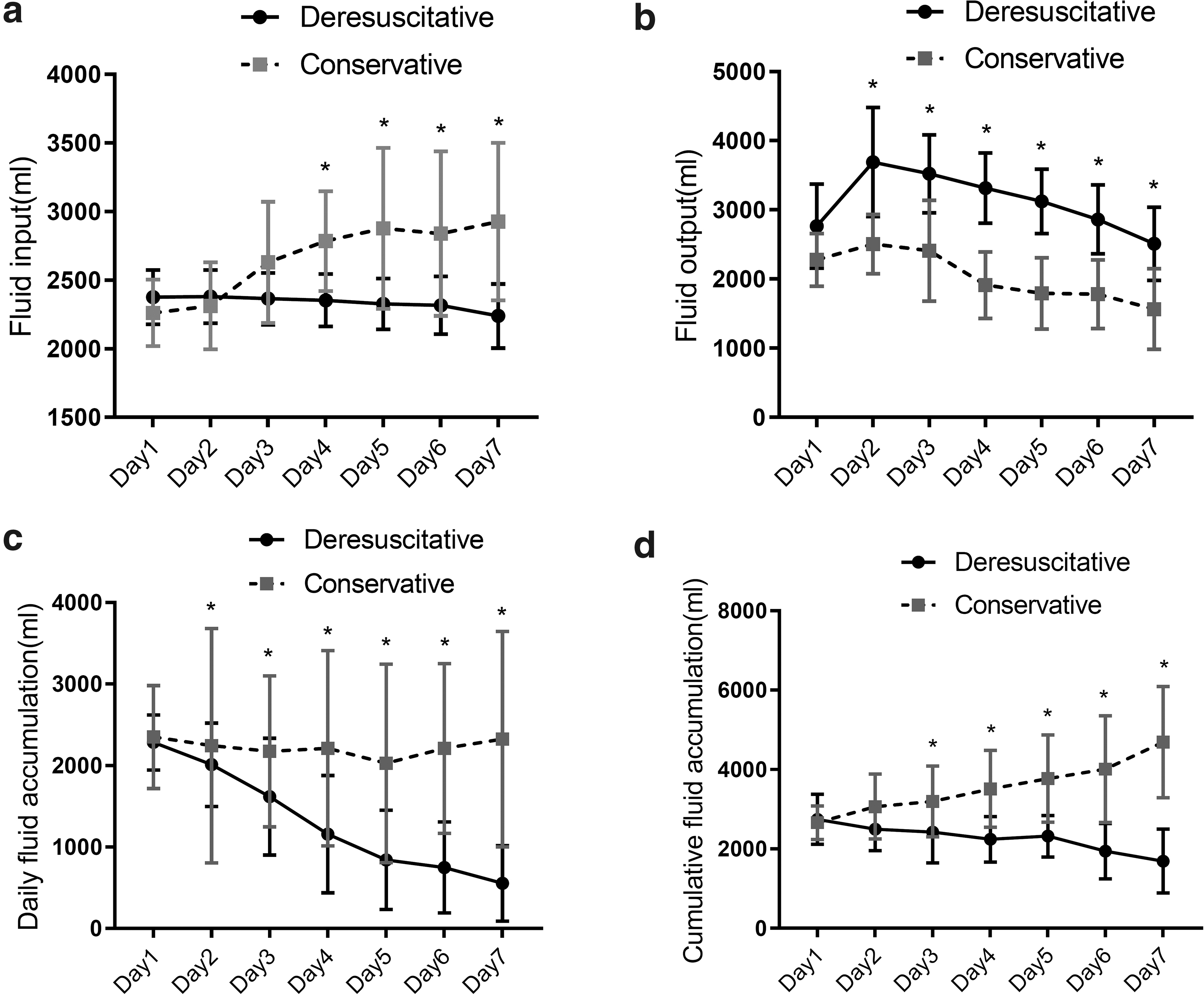
Fluid accumulation during first 7 days (Days 1–7) of intensive care unit admission in deresuscitative vs. conservative therapy. *Statistically significant difference at p < 0.05 between fluid management strategies.
Fluid strategy and in-hospital death
Univariable analysis showed that the nonsurvivors had a higher ratio of septic shock and source control failure on admission, and the nonsurvivors also received less deresuscitative fluid therapy (Table 3). Nonsurvivors required longer-term CRRT treatment (OR 1.087; 95% CI 1.039–1.137).
Univariable and Multivariable Analyses with In-Hospital Death as Outcome
APACHE = Acute Physiology, Age, and Chronic Health Evaluation; CI = confidence interval; CRRT = continuous renal replacement therapy; FO = fluid overload; MV = mechanical ventilation; OR = odds ratio; SOFA = Sequential Organ Failure Assessment.
Our multivariable logistic regression model revealed that deresuscitative fluid management imparted protection against in-hospital death (OR 4.343; 95% CI 1.466–12.866), whereas septic shock on admission (OR 5.390; 95% CI 1.986–14.629), source control failure (OR 12.791; 95% CI 1.484–110.262), and CRRT duration (OR 1.064; 95% CI 1.013–1.116) were independent risk factors for in-hospital death (Table 3).
Discussion
A deresuscitative fluid strategy resulted in a lower in-hospital mortality rate, which most likely influences subsequent fluid therapy. Furthermore, deresuscitative treatment was correlated independently with a lower mortality rate despite its occurrence during the later stage of resuscitation. No significant association was observed between deresuscitative fluid strategy and abdominal conditions, including open abdomen and ACS or IAH, although this association was observed irrespective of deresuscitative treatment. Finally, a deresuscitative fluid strategies may help change some of the underlying practical factors, particularly AKI, which may show how to treat specific organs better.
Fluid management strategies in critically ill patients consist of four phases, namely, salvage, optimization, stabilization, and de-escalation (or deresuscitation) [22]. Aggressive fluid management is essential to infuse enough fluid volume during hemodynamic instability in the early phase of a critical illness. The deresuscitative fluid strategy comprises a series of clinical measures, and water may be removed during the later hemodynamically stable phase when sufficient fluid volumes have been achieved.
Patients with source control failure because of ineffective treatment of the infected lesions still suffer from repeated inflammatory reactions and organ dysfunction, and fluid input cannot be reduced or even stopped, which affects the administration of subsequent fluid deresuscitation measures; and these patients might have more opportunity to receive deresuscitation therapy. Therefore, successful source control is the premise of effective deresuscitation. In turn, inadequate or improper timing of deresuscitation may affect the healing of a gastrointestinal anastomosis or abdominal incision, possibly resulting in gastrointestinal fistula formation or abdominal fascia rupture. Eventually, source control failure or new sources of infection emerge, creating a vicious cycle. This may explain in part why the proportion of patients with source control failure in the deresuscitation group in this study was higher than that in the conservative treatment group, although there was no statistical difference.
Patients receiving deresuscitative treatment had a significantly lower rate of new-onset AKI and a CRRT or MV duration shorter than those receiving conservative treatment. There were no differences in open abdomen, new-onset ACS, or IAH; however, the positive correlation between FO and AKI has been well established [23]. We also observed an increase in the incidence of AKI after conservative fluid therapy, which was accompanied by a higher volume of fluid input and lower fluid output. A gradual increase in fluid accumulation also was observed in the conservative treatment group, which is similar to the findings of earlier studies [24].
Patients who received conservative fluid treatment showed a higher risk for in-hospital death, had a longer hospital LOS, and were more likely to have renal dysfunction. Our previous study found that excessive fluid is associated with a poorer prognosis in patients with IAIs [25], and fluid volume overload correlates negatively with delayed primary fascial closure in open abdomen [26]. In contrast, in the current study, no significant relation between deresuscitation management and open abdomen, including achieved fascia closure or new-onset fistula, was observed. This may be secondary to our inclusion of sepsis patients who had completed early fluid resuscitation, and most patients presented with FO on ICU admission. Further work is necessary to establish the optimal fluid strategy and fluid type in this specific situation.
Fluid overload was correlated independently with the outcomes of critically ill patients. Damage control resuscitation may result in IAH or ACS [27]. These conditions could lead to self-perpetuating cycles that cause severe physiologic derangements and multiorgan failure unless intervention is performed using abdominal decompression [28]. Other alterations in capillary fluid dynamics were attributable to factors such as massive fluid resuscitation and generalized inflammation. Renal and gastrointestinal effects were observed during the early stage of IAH and are associated with poor patient outcomes when they go undetected [29]. Intestinal microcirculation significantly decreased, as much as 50%, with intra-abdominal pressures as low as 15 mm Hg [30]. Hypoperfusion of gut mucosal and submucosal tissues induces considerable damage to intestinal epithelial cells, which in turn may result in bacterial translocation, endotoxin release, and sepsis, as well as multiple organ failure [31,32]. However, clinical signs and symptoms of acute gastrointestinal injury may go undetected or be considered mistakenly to be symptoms of other critical illnesses.
The practice of the sepsis guidelines and the extent of intensive care has improved, and timely and sufficient fluid resuscitation has been implemented in most sepsis scenarios. However, most of the cited studies have focused on the early stages of fluid resuscitation in sepsis [33]. Recently, four stages of fluid management strategies for critically ill patients have been used as a new scheme, and fluid administration should be adapted along with the time course of sepsis. Once a patient has been stabilized, removal of excess fluid should be prioritized. Fluid administration should be prescribed as a therapeutic approach, with the type and dosage based on every patient's particular requirements and tolerance [34].
This study has a number of limitations. First, the sample size is modest, and practice variability was assessed in only a single center; and thus the results may not represent the entire population of interest fully, and practice variability may be underestimated. Second, the retrospective nature of our study might not allow the determination of indications or clinician intent for practice variables. Third, without prospective screening, our data on pre-ICU FB were insufficient. Finally, despite adjustment for illness severity, we were unable to exclude the possibility that the correlation between positive FB and poor outcomes reflects residual confounding according to indication.
Conclusion
This study demonstrated that deresuscitative fluid treatment correlated with a lower in-hospital mortality rate and less likelihood of AKI. The deresuscitative approach using limited maintenance fluid intake, as well as removal of FO to minimize FB, may be useful as a therapeutic strategy. Randomized controlled trials are warranted to confirm these findings.
Footnotes
Acknowledgments
Jianan Ren and Zhizhao Jiang designed the study. Zhizhao Jiang, Huajian Ren, and Zhiwu Hong performed data collection. Zhizhao Jiang wrote the manuscript. All authors contributed substantially to this study. All authors have read and approved the final version of the manuscript. We thank LetPub (![]() ) for its linguistic assistance during the preparation of this manuscript.
) for its linguistic assistance during the preparation of this manuscript.
Funding Information
No funding was received for this work.
Author Disclosure Statement
The authors declare that they have no proprietary or commercial interest in any component mentioned or concept discussed in this report.