
Abstract
Background:
Multiple studies have reported that gender, pre-operative stent insertion, positive pre-operative urine culture results, and diabetes mellitus are associated with infectious complication after ureteroscopy. A previous meta-analysis focused on this topic is based, however, on crude estimate. Further analysis based on adjusted estimates is needed.
Methods:
PubMed, Web of Science, Embase, and the Cochrane Library database were searched with ureteroscopy, ureteroscopies, ureteroscopic surgical procedures, ureteroscopic surgery, ureteroscopic lithotripsy, flexible ureteroscopic lithotripsy, ureteroscopy (URS), flexible ureterorenoscopy, risk factor, predictor, predicting model, and nomogram until December 15, 2019. The quality of research was evaluated by Newcastle-Ottawa Scale system. Odds ratio (OR) and 95% confidence intervals (CI) of each risk factor were extracted. Meta-analysis was performed with Stata 15.0 software. Heterogeneity was assessed by I2. Publication bias was tested by the Egger test, and funnel plot. Meta-regressions and subgroup analysis were further performed.
Results:
There were 16 studies; 12,357 patients finally were included in this meta-analysis. The association between gender (OR = 1.82, 95% CI: 1.48–2.23, I2 = 0%, p = 0.701), pre-operative ureteric stent insertion (OR = 1.91, 95% CI: 1.26–2.91, I2 = 40.4%, p = 0.109), diabetes mellitus (OR: 1.40, 95% CI: 1.07–1.85, I2 = 34.1%, p = 0.168), positive urine culture before URS (OR: 2.18, 95% CI: 1.34–3.57, I2 = 47.2%, p = 0.092), operation duration (OR: 1.03, 95% CI: 1.01–1.04, I2 = 70.6%, p = 0.001) and infectious complications was positively significant. All four pooled results were different from results of meta-analysis based on crude estimate.
Conclusion:
Female gender, pre-operative ureteric stent insertion, diabetes mellitus, positive urine culture results before URS, and operation duration are risk factors for infectious complications after URS. Meta-analysis based on adjusted estimates may be more convincing.
There is a growing number of urologists who will use ureteroscopy (URS) as their preferred choice in the management of renal and ureteral calculi. Post-operative infectious complication is one of the most important complications for patients with ureteroscopy [1]. Many risk factors such as gender, diabetes mellitus, pre-operative stent insertion, and positive pre-operative urine culture results have been identified for infectious complication.
Further, a recent meta-analysis attempted to provide a systematic review concerning infectious complication in ureteroscopy [2]. After careful reading, however, of this recent meta-analysis, the pooled results of many factors such as gender, age, operation duration, and positive urine culture results were based on uni-variable analysis or crude odds ratio (OR) results.
To our knowledge, most studies on risk factors are retrospective studies, and their conclusions are likely to be influenced by many biases. To eliminate as many bias factors as possible, meta-analysis is a feasible method. A meta-analysis based on crude OR, however, can only get a pooled crude OR that may still contain many biases. In the meta-analysis of the retrospective studies of risk factors, the pooled results based on the multi-variable regression results (adjusted OR) may be more convincing [3].
In this study, to avoid various biases as much as possible, a meta-analysis only based on the multi-variable logistic regression was conducted to obtain the best assessment of the risk factors of infectious complications in ureteroscopy.
Methods
Literature search and inclusion criteria
A published study search procedure was performed in Pubmed, Embase, and Cochrane Library. The latest search date was December 9, 2019. The searching key words included ureteroscopy, ureteroscopies, ureteroscopic surgical procedures, ureteroscopic surgery, ureteroscopic lithotripsy, flexible ureteroscopic lithotripsy, URS, fURS, risk factor, predictor, predicting model, nomogram. Further, the reference section of every candidate literature selection was screened manually to find possible data sources.
Detailed inclusion criteria were as follows: Patients were treated with URS or ureteroscopic lithotripsy, and comparisons should be conducted between patients with infectious complications and patients without infectious complications. Studies performed multi-variable logistic regressions between post-operative infectious complications and candidate risk factors. The OR with 95% confidence interval (CI) of risk factors were offered. Exclusion criteria were as follows: Reviews, meta-analysis, letters, comments, case serials, and conference abstract were excluded. Studies that did not contain regression information or enough data usable for secondary analysis were excluded.
Research quality evaluation
All included studies were evaluated by the Newcastle-Ottawa Scale (NOS) system; the evaluation procedure was performed by two independent reviewers [4]. According to the NOS, 7–9 score studies were considered high-level quality, 5–6 score studies were considered moderate-level quality, and <5 score studies were considered low-level quality. Low-level quality studies should not be involved in the meta-analysis.
Meta-analysis
In this study, based on multi-variable logistic regression results, the relationship between candidate risk factors and infectious complication was pooled in meta-analysis. All analyses were powered by Stata 15.0 software (Stata Corporation, College Station TX). Statistical significance was defined as p < 0.05 in this study. Pooled OR larger than 1 indicated that this factor would make patients more vulnerable for post-operative infectious complications.
Because there are two different end points (fever/urinary tract infection [UTI] and systemic inflammatory response system [SIRS]/urosepsis) in the involved studies, subgroup analysis between different end points was performed. Heterogeneity was evaluated by I2. When I2 was larger than 50%, heterogeneity could be significant. To get more stable results, if I2 in the primary meta-analysis was larger than 0%, random effect model would be implied for meta-analysis.
To identity the potential factors that contributed to heterogeneity, meta-regression analysis was performed. When only the median interquartile range (IQR) age information was provided in the involved studies, the mean age was estimated by methods described previously [5]. Subgroup analysis based on meta-regression was also performed to get detailed information. Further, sensitivity analysis was performed to test stability of meta-analysis results, and publication-bias was tested by the Egger test. Funnel plots were used for visual publication-bias visual identification.
Results
Study selection
After the literature screening, there were a total of 16 studies involved in this meta-analysis. The detailed screening procedure is displayed in Figure 1. A total of 727 studies were identified from databases. After duplicates were removed, 526 studies were enrolled into abstract screening. After the abstract screening and full text reading, 16 studies, 12,357 patients finally were involved in this meta-analysis.
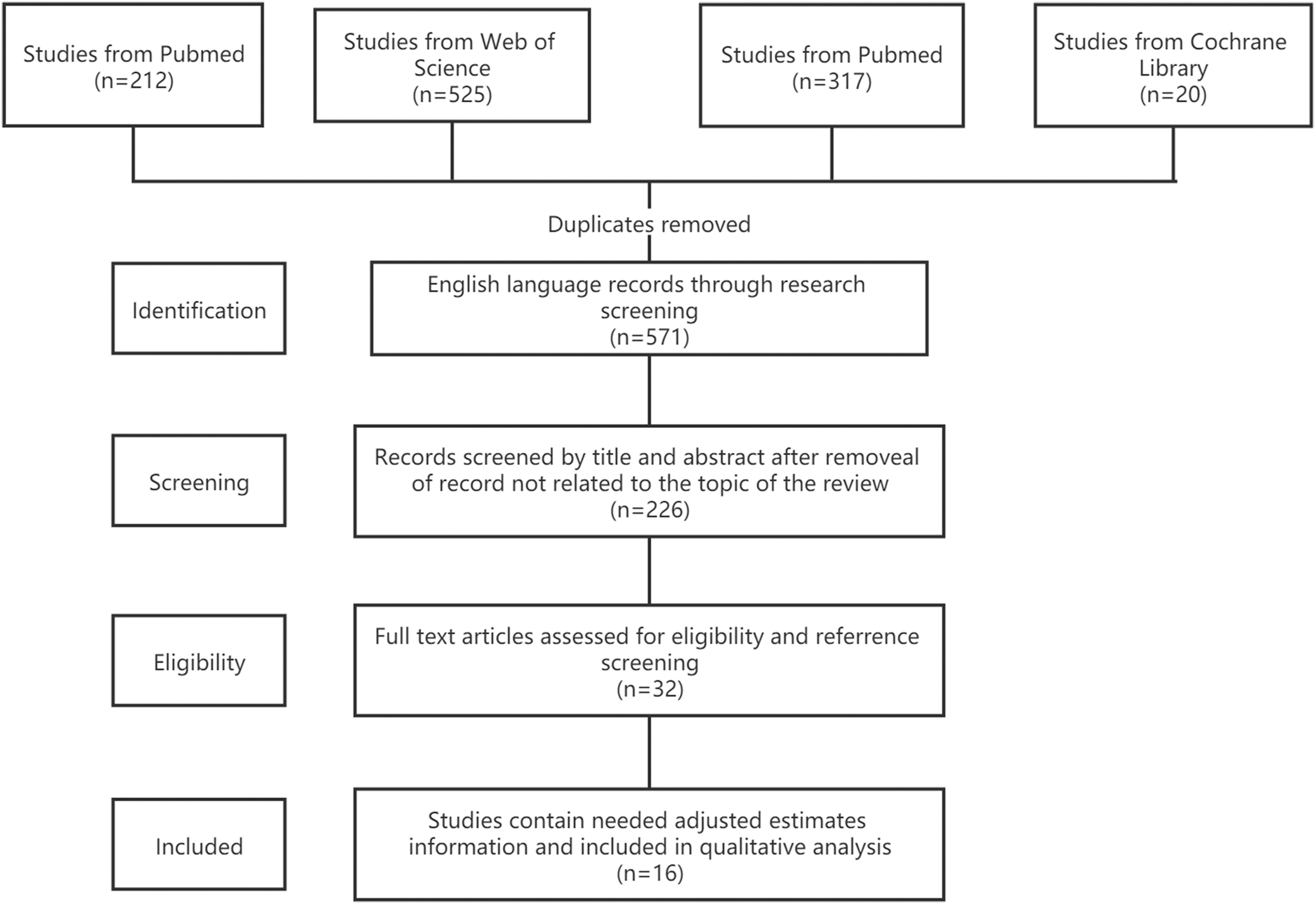
Flowchart of selection of included studies.
There were eight studies (total 8,303 patients in involved studies) containing gender anti-complication multi-variable logistic regression information [6–13], seven studies (total 5,154 patients in involved studies) containing diabetes mellitus anti-complication multi–variable analysis information [7,10,12,14–17], eight studies (total 9,446 patients in involved studies) containing pre-operative ureteric stenting anti-complication multi-variable analysis information [6–10,13,18,19], eight studies (total 7,325 patients in involved studies) containing operation time anti-complication multi-variable analysis information [7,9,12,14,16,17,19,20], six studies (total 6,478 patients in involved studies) containing pre-operative urine culture anti-complication multi-variable analysis information [8,9,11,12,15,19]. Of 16 involved studies, 14 studies are retrospective cohort studies and two are case-control studies. Detailed baseline information is listed in Table 1.
Characteristics of Studies Included in the Meta-Analysis
NOS = Newcastle-Ottawa Scale; RCS = retrospective cohort study; SIRS = systemic inflammatory response system; NR = not reported; SCCM = Society of Critical Care Medicine; ESICM = European Society of Intensive Care Medicine; ACCP = American Society of Chest Physicians; ATS = American Thoracic Society; SIS = Spine Intervention Society; WBC = white blood cell; UTI = urinary tract infection; POF = post-operative fever.
Gender
The association between gender and post-operative infectious complications was explored in eight studies containing 8,303 patients. According to the overall meta-analysis result, female patients are more vulnerable for infectious complications (OR = 1.82, 95% CI: 1.48–2.23, p < 0.0001) with no obvious heterogeneity found among the eight studies (I2 = 0%, p = 0.701). According to the subgroup analysis, female patients are more vulnerable for post-operative fever/UTI (OR = 1.92, 95% CI: 1.38–2.67, p < 0.0001, I2 = 0%, p = 0.582) and SIRS/urosepsis (OR = 2.63, 95% CI: 1.28–5.38, p = 0.008, I2 = 0%, p = 0.872), Figure 2.

Meta-analysis on the association between female gender and infectious complications. Subgroup analysis was conducted between different infectious end points. ES = estimate; CI = confidence interval; UTI = urinary tract infection.
No significant publication bias was found according to the Egger test (t = 0.97, p = 0.367), as was shown in a funnel plot (Fig. S1A). Sensitivity analysis showed that the results were not significantly changed by eliminating studies one by one (Fig. S2A).
Although there was no noticeable heterogeneity in the meta-analysis mentioned above, further meta-regression was also performed to get more information. According to the meta-regression and subgroup analysis results, in the early published studies (earlier than 2017), female gender is a more dangerous risk factor than reported in recent three-year studies (earlier than 2017 OR: 1.99, 95% CI: 1.48–2.23 vs. recent three-year OR: 1.75, 95% CI: 1.39–2.22, p = 0.018). It was indicated that compared with males of their respective population, Asian females may be more vulnerable than white females (Asian OR: 1.78, 95% CI: 1.10–2.87 vs. white OR: 1.71, 95% CI: 1.32–2.22, p = 0.01).
Prophylactic antibiotic subgroup analysis indicated that, compared with selective prophylactic antibiotic use, general prophylactic antibiotic use may protect females from overall infectious complications more effectively (general prophylactic antibiotic use OR: 1.76, 95% CI: 1.39–2.22 vs. selective prophylactic antibiotic use OR: 1.99, 95% CI: 1.29–3.08, p = 0.004). Sample size (p = 0.055), age (p = 0.47), operation duration (0.20) did not affect meta-analysis results. Detailed gender-complication meta-regression information is listed in Table 2.
Meta-Regression and Subgroup Analyses of Female Gender
OR = odds ratio; CI = confidence interval.
Pre-Operative Ureteric Stent Insertion
The association between pre-operative ureteric stenting and post-operative infectious complications was discussed in eight studies containing 9,446 patients. According to the overall meta-analysis result, patients receiving pre-operative ureteric stenting are more vulnerable for infectious complications (OR = 1.91, 95% CI: 1.26–2.91, p = 0.002] with moderate heterogeneity found among eight studies (I2 = 40.4%, p = 0.1257). According to the subgroup analysis, patients receiving pre-operative ureteric stenting are more vulnerable for post-operative SIRS/urosepsis (OR = 3.04, 95% CI: 1.67–5.54, p < 0.0001, I2 = 0%, p = 0.542) than fever/UTI (OR = 1.79, 95% CI: 1.17–2.76, p = 0.008, I2 = 0%, p = 0.407), Figure 3.
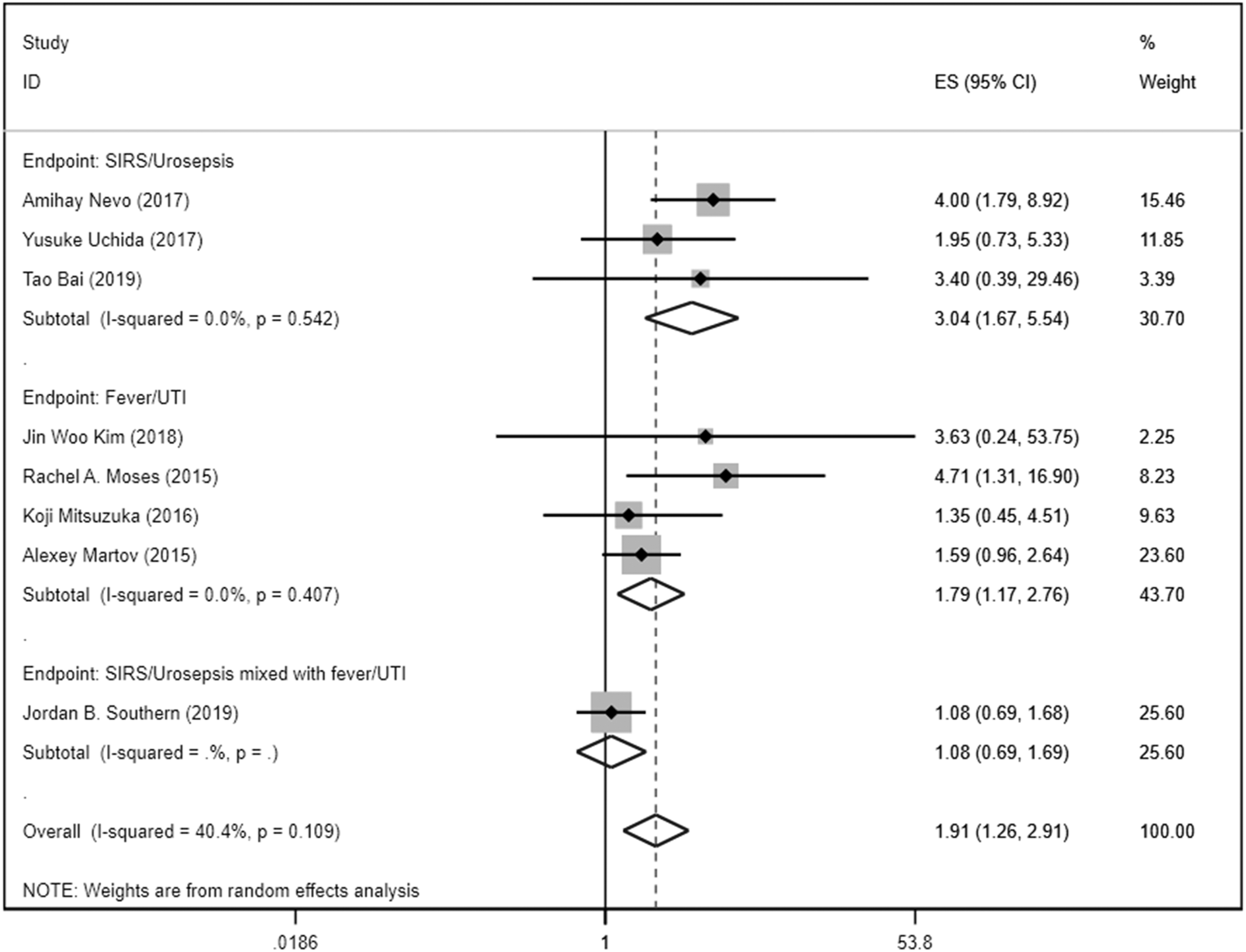
Meta-analysis on the association between pre-operative ureteric stent insertion and infectious complications. Subgroup analysis was conducted between different infectious end points. ES = estimate; CI = confidence interval; SIRS = systemic inflammatory response system; UTI = urinary tract infection.
No significant publication bias was found according to the Egger test (t = 1.95, p = 0.099), shown in A funnel plot (Fig. S1B). Sensitivity analysis showed that the results were not significantly changed by eliminating studies one by one (Fig. S2B).
Because moderate heterogeneity was found (I2 = 40.4%, p = 0.1257), further meta-regression was performed to get more information. After meta-regression, it was found that patient number of each involved studies (p = 0.045) may also contribute the heterogeneity besides a different end point. Publication year (p = 0.134), involved population (p = 0.092), prophylactic antibiotic agents (p = 0.376), mean age (0.669), mean operation duration (p = 0.578) did not affect the meta-analysis result significantly. Detailed regression information is displayed in Table 3.
Meta-Regression and Subgroup Analyses of Pre-Operative Ureteric Stent Insertion
OR = odds ratio; CI = confidence interval.
Diabetes mellitus
The association between diabetes mellitus and post-operative infectious complications was discussed in seven studies containing 5,154 patients. According to the overall meta-analysis result, patients with diabetes mellitus are more vulnerable for infectious complications (OR = 1.40, 95% CI: 1.07–1.85, p = 0.015) with moderate heterogeneity found among eight studies (I2 = 34.1%, p = 0.168). According to the subgroup analysis, patients with diabetes mellitus are more vulnerable for post-operative fever/UTI (OR = 1.58, 95% CI: 1.06–2.38, p = 0.026, I2 = 12.1%, p = 0.332), Figure 4.
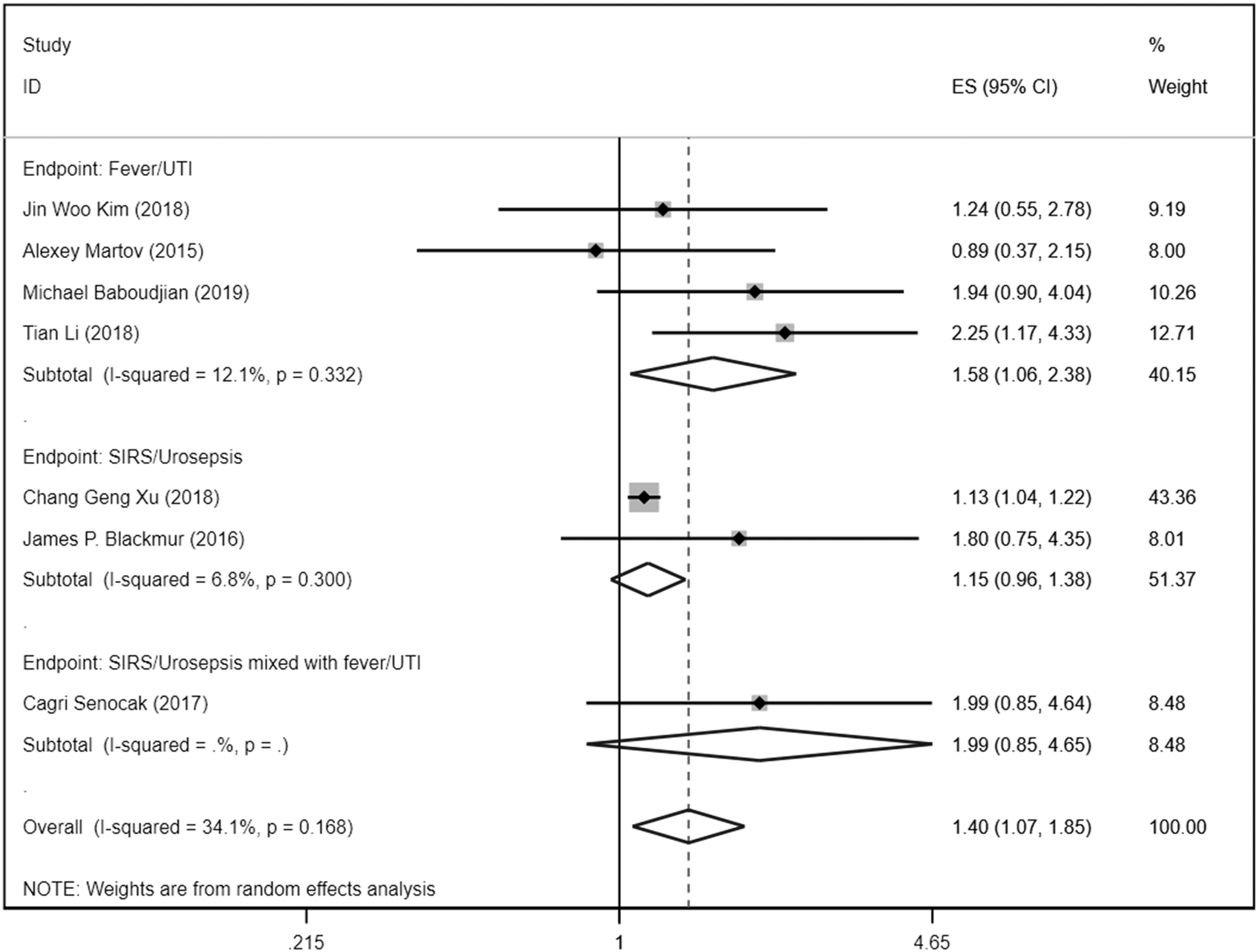
Meta-analysis on the association between diabetes mellitus and infectious complications. Subgroup analysis was conducted between different infectious end points. ES = estimate; CI = confidence interval; SIRS = systemic inflammatory response system; UTI = urinary tract infection.
No significant publication bias was found according to the Egger test (t = 2.30, p = 0.07) as shown in a funnel plot (Fig. S1C). Sensitivity analysis showed that when eliminating Baboudjian et al. [12] (OR: 1.29, 95% CI: 0.97–1.61), Blackmur et al. [15] (OR: 1.32, 95% CI: 0.98–1.66), and Senocak et al. [16] (OR: 1.29, 95% CI: 0.97–1.62), meta-analysis results became unstable; this situation indicated that more related studies were required to get a stable conclusion (Fig. S2C).
Further meta-regression was conducted to explore potential heterogeneity resource besides different end points. Publication year (p = 0.548), population (0.823), mean age (0.974), mean operation duration (p = 0.295), prophylactic antibiotic agents (p = 0.808), patient number (p = 0.069) did not affect meta-analysis results significantly. Detailed information is in Table 4.
Meta-Regression and Subgroup Analyses of Diabetes Mellitus
Pre-operative urine culture
The association between positive pre-operative urine culture and post-operative infectious complications was discussed in six studies containing 6,478 patients. According to the overall meta-analysis result, patients with positive pre-operative urine culture results are more vulnerable for infectious complications (OR = 2.18, 95% CI: 1.34–3.57, p = 0.002); moderate heterogeneity was found among eight studies (I2 = 47.2%, p = 0.168).
According to the subgroup analysis, patients with positive pre- operative urine culture results are more vulnerable for post-operative SIRS/urosepsis (OR = 1.58, 95% CI: 1.06–2.38, p = 0.026, I2 = 12.1%, p = 0.092) than overall infectious complications (Fig. 5). No significant publication bias was found according to the Egger test (t = 0.94, p = 0.40 and Begg test (z = -0.19, p = 0.851), as shown in a funnel plot (Fig. S1D). Sensitivity analysis showed that the results were not significantly changed by eliminating studies one by one (Fig. S2D).
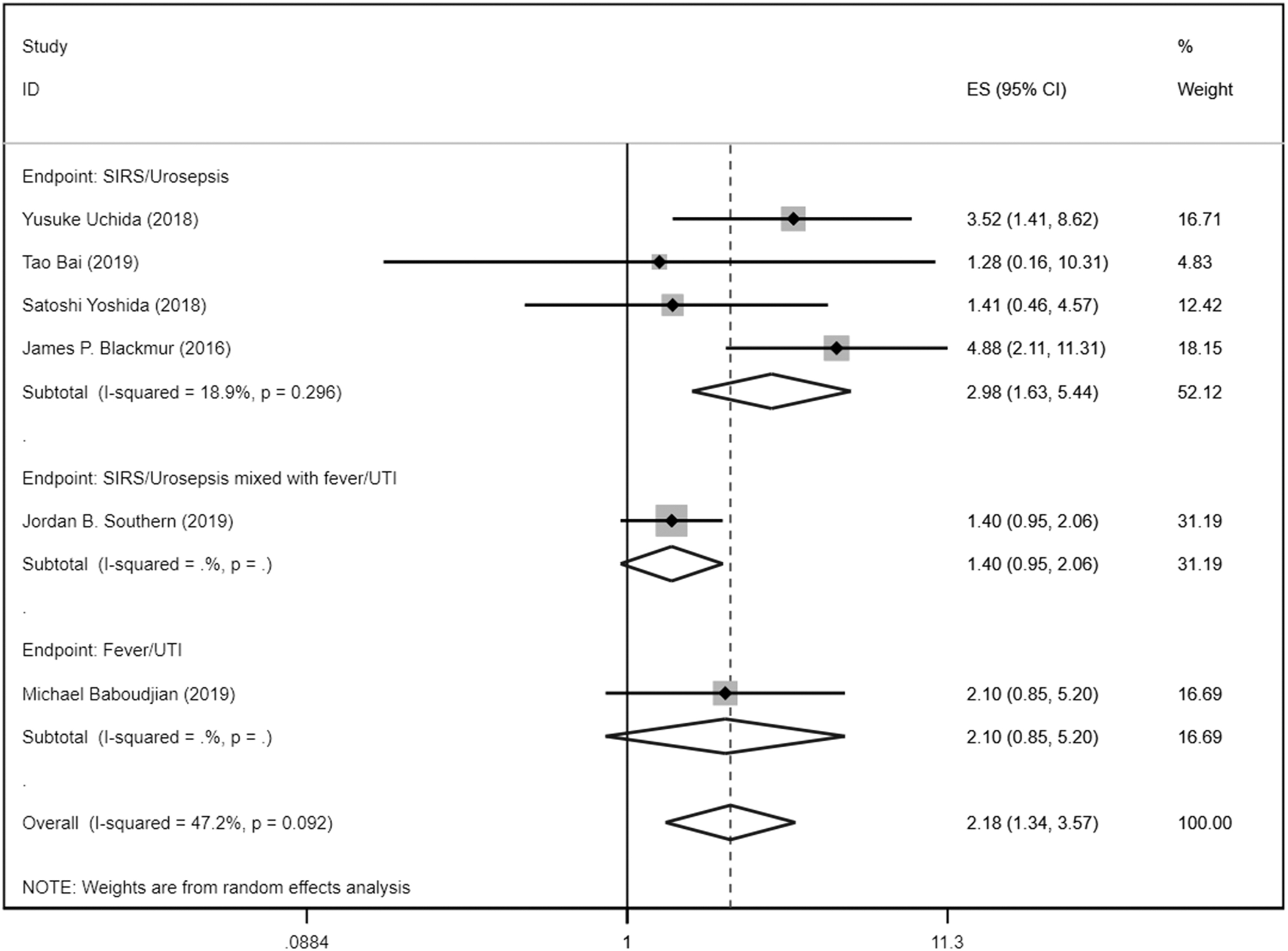
Meta-analysis on the association between pre-operative urine culture and infectious complications. Subgroup analysis was conducted between different infectious end points. ES = estimate; CI = confidence interval; SIRS = systemic inflammatory response system; UTI = urinary tract infection.
In the meta-regression, publication year of studies can affect the results of meta-analysis (p = 0.028) and may be one of resources of heterogeneity. Patient number in involved studies was another significant factor that can affect meta-analysis result (p = 0.013), and subgroup analysis indicated that in small size studies (patients <500), the effect of pre-operative urine culture results on infectious complications might be overestimated (>500 patients OR: 1.48, 95% CI: 1.05–2.1 vs. <500 patients OR: 3.17, 95% CI: 1.63–6.18). Population (p = 0.082), mean age (p = 0.22), mean operation duration (p = 0.109), prophylactic use (p = 0.054) did not affect meta-analysis results. Detailed meta-regression between positive pre-operative urine culture results and infectious complication information is displayed in Table 5.
Meta-Regression and Subgroup Analyses of Pre-Operative Urine Culture
OR = odds ratio; CI = confidence interval.
Operation duration
The association between operation duration and post-operative infectious complications was discussed in eight studies containing 7,325 patients. According to the primary overall meta-analysis result, patients with longer operation time (min) are more vulnerable for infectious complication (OR = 1.03, 95% CI: 1.01–1.04, p = 0.001]; noticeable heterogeneity was found among eight studies (I2 = 70.6%, p = 0.001), Figure 6.
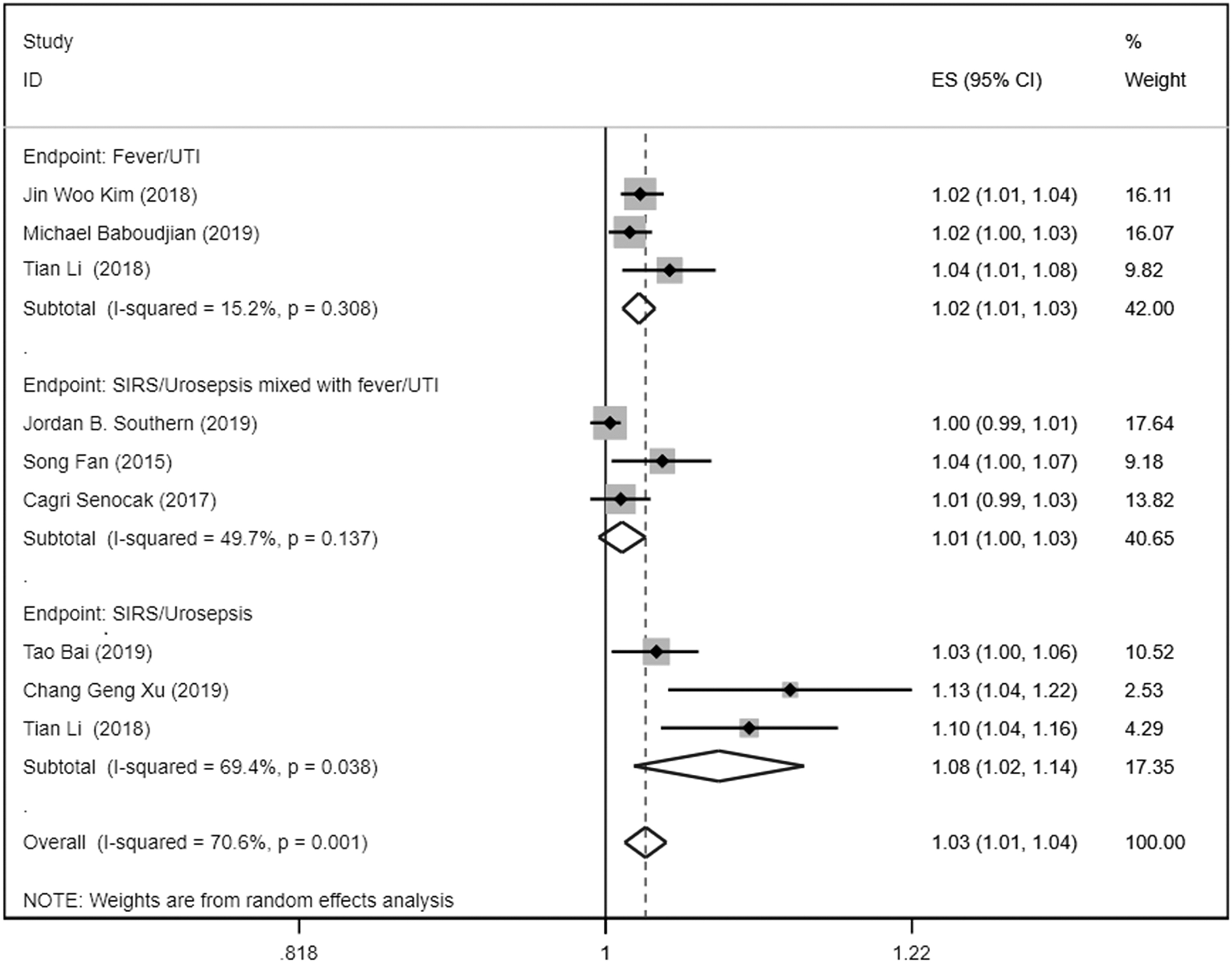
Meta-analysis on the association between operation duration and infectious complications. Subgroup analysis was conducted between different infectious end points. ES = estimate; CI = confidence interval; UTI = urinary tract infection; SIRS = systemic inflammatory response system.
According to the subgroup analysis, patients with longer operation time (min) are vulnerable for post-operative fever/UTI (OR = 1.02, 95% CI: 1.01–1.03, p < 0.001, I2 = 15.2%, p = 0.308) and also vulnerable for post-operative SIRS/urosepsis (OR: 1.08, 95% CI: 1.02–1.14, p = 0.009, I2 = 69.4%, p = 0.0017), Figure 6 (study conducted by Tian Li offered both two endpoint data).
After the Egger test (t = 4.19, p = 0.004), Begg test (z = 2.50, p = 0.012] and funnel plot (Fig. S1), however, significant publication bias was detected. Therefore, further trim-and-fill analysis was conducted to have a proper publication-bias corrected overall meta-analysis result for association between operation duration and post-operative infectious complications (OR: 1.02 95% CI: 1.001–1.03, p = 0.034).
Discussion
In this systematic review and meta-analysis, a total of 12,357 patients were included from 16 studies. It was found that gender, pre-operative ureteric stent insertion, diabetes mellitus, pre-operative urine culture results, and operation duration are significant risk factors for post-operative infectious complication in URS.
On the basis of meta-analysis results mentioned in this study, a positive pre-operative urine culture result is the most important risk factor (OR: 2.18, 95% CI: 1.34–3.57) with no significant heterogeneity among six included studies (I2 = 47.2%). According to the European Association of Urology guideline, urine culture is still the most important laboratory test for the diagnosis of UTI [21]. Obviously, if there is bacterial infection in the urinary tract, along with the insertion of an ureteroscope and normal saline washing, a large number of bacteria may enter the collecting system or enter the blood through the damaged mucosa, which may significantly increase the risk of post-operative infectious complications such as fever/SIRS urosepsis
When the pre-operative urine culture results are positive, usually sensitive antibiotic agents will be used for treatment. Most urologists will only perform URS after the UTI is controlled. In this context, the history of positive urine culture results will still significantly increase the risk of post-operative infectious complications. This suggests that controlling the existing infection symptoms cannot completely avoid the risk of post-operative infectious complications, and the etiology/inducement control of the existing UTI is the recommendation for patients with positive urine culture results.
Pre-operative ureteric stent insertion is another risk factor for infectious complications (OR: 1.91, 95% CI: 1.26–2.91; no significant heterogeneity was found (I2 = 40.4%. p = 0.109). A pre-operative ureteric stent is usually used to drain hydronephrosis or to expand the ureter to facilitate the insertion of the flexible ureteroscope sheath [22]. The possible cause is that during and after the ureteric stent insertion, ureteral implants provide a fixed route for bacteria to spread upward from the lower urinary tract [23]. Although hydronephrosis is not a significant risk factor for post-operative infectious complications according to the results of the included study, if stent placement before URS is strictly controlled, it may lead to renal function impairment and increased risk of upper UTI. Therefore, it is still necessary for urologists to make a comprehensive decision on whether to place a ureteric stent before operation.
A third significant risk factor for infectious complication for patients undergoing URS is female gender (OR: 1.82 95% CI: 1.48–2.23). For most urologists, female patients are more likely to have a UTI; this experience is supported by many published studies [24–26]. Because the female urethra is shorter and straighter than the male urethra, bacterial invasion is more likely to occur in females than in males [27].
Ureteric stent placement before operation, insertion of the ureteroscope, and washing with physiologic saline during URS may bring bacteria in the lower urinary tract into the upper urinary tract, increasing the risk of infectious complications. Further, the flora in the vagina and the effect of sex hormones on the urinary tract will affect the susceptibility of female patients to UTI [28, 29].
This meta-analysis also indicates that patients with diabetes mellitus are more vulnerable for infectious complications after URS (OR: 1.40, 95% CI: 1.07–1.85, I2 = 34.1%) with no significant heterogeneity (I2 = 34.1% p = 0.168). For patients with diabetes mellitus, increased urine sugar and blood sugar levels, as well as impaired immune systems, increase their risk of urinary infections, and it is also generally accepted that for a diabetic patient, peri-operative infection management should be usually more cautious [30–32].
Although the vast majority of medical institutions will be cautious about post-operative infection in patients with diabetes mellitus, a history of diabetes still leaves patients with a higher risk of post-operative infectious complications. Therefore, for URS of diabetic patients, more strict and cautious infection precaution management should be taken.
For a long time, surgical duration of ureteroscopic lithotripsy has been considered a risk factor for post-operative infectious complications, which is supported by this meta-analysis (operation duration/min OR: 1.03, 95 CI% 1.01–1.04). Because significant publication bias was detected, an estimated OR (OR: 1.02 95% CI: 1.001–1.03, p = 0.034) of operation duration was obtained through Trim-and-Fill analysis [33]. For all ureteroscopic procedures, longer operation duration means longer irrigation time, which may lead to more bacteria carrying saline into the kidney collecting system or urinary tract mucosa damage and cause infectious complications.
For ureteroscopic lithotripsy, many factors such as stone size and stone location can affect the operation duration. As a “comprehensive factor,” operation duration actually integrates much basic information concerning stones. Although there is no high-level evidence on the threshold of ureteral operation duration published, according to the existing research, when the operation duration is greater than 120 min, it may bring greater risk of post-operative infection for patients [18].
This meta-analysis only included the multi-variable regression adjusted OR value of risk factors. Compared with the previous meta-analysis based on uni-variable analysis (crude OR), the pooled OR value of all risk factors is different. For female gender, the OR value decreases from 1.95, 95% CI: 1.48–2.57 to 1.82, 95% CI: 1.48–2.23. For pre-operative stent insertion, the OR value increases from 1.53, 95% CI: 1.11–2.11 to 1.91, 95% CI: 1.26–2.91]. For diabetes mellitus, the OR value deceases from 1.55 95% CI: 1.13–2.13 to 1.40, 95% CI: 1.07–1.85.
To include more studies, many researchers tend to use uni-variable analysis results to conduct meta-analysis. A meta-analysis based on crude OR will also bring a lot of bias into the conclusion. It may be better to conduct meta-analysis based on uni-variable analysis (crude OR/HR/RR) as a rough estimate and supplement if there is no multi-variable analysis data result offered by primary studies.
There are some limitations to this study. First, all the studies included in this analysis were retrospective studies. Second, heterogeneity and publication bias were found in some risk factors. Third, although we tried to differentiate the types of ureteroscopes used in different studies, most studies only mentioned that semi-rigid and flexible ureteroscopes were used. No detailed information was offered; this may bring some heterogeneity. Fourth, because this study only included multi-variable regression results, many risk factors such as age, post-operative stent, stone diameter, and renal function were not involved. Last, to get more robust risk factor analysis results, more clinical research studies are required.
Conclusion
On the basis of the multi-variable analysis results, this meta-analysis found that gender, pre-operative ureteric stent insertion, diabetes mellitus, pre-operative urine culture results, and operation duration are risk factors for infectious s in URS management.
Footnotes
Authors' Contributions
Yu-cheng Ma: project development, data collection, data analysis, manuscript writing; Zhong-Yu Jing: project development, data collection, data analysis, manuscript writing; Chi Yuan: project development, data collection, data analysis, manuscript writing; Hong Li: project development, critical revision of the article; Kun-Jie Wang: project development, critical revision of the article.
Funding Information
This article is supported by grants from 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD18011 and ZYJC18015), Chengdu Science and Technology Bureau (2016-HM02-00020-SF), Project of Science and Technology Department of Sichuan Province (2018SZ0118).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.