Response to Tom et al.,Comparison of Traditional and Skin-Sparing Approaches for Surgical Treatment of Necrotizing Soft-Tissue Infections (DOI: 10.1089/sur.2019.263)
Available accessLetterFirst published online June, 2020
Response to Tom et al.,Comparison of Traditional and Skin-Sparing Approaches for Surgical Treatment of Necrotizing Soft-Tissue Infections (DOI: 10.1089/sur.2019.263)
We commend the Harborview team on the successful implementation of a skin-sparing (SS) approach to necrotizing soft-tissue infections (NSTI) [1]. We agree about the monumental importance of sparing viable skin and soft tissue during source-control surgery in anticipation of closure, as the fascial-level infection often outpaces the superficial devitalization (Fig. 1A, B). It has been our experience that SS achieves reduced length of stay, faster healing, and good cosmesis without increased complications [2]. Skin sparing deviates from the traditional approach at the time of the first debridement, but many patients with NSTI (38.8%) undergo initial debridement at a referring hospital. We assert that in addition to SS during the first phase, the magnitude of success is attributable to the utilization of spared skin in subsequent operations; specifically, we employ the term “progressive tensioning” to describe this second complementary phase. Although their article refers to a median of three debridement procedures prior to reconstruction, it is the Harborview team's 2016 work that details use of Silastic vessel loops in a “criss-cross” or Roman sandal design to promote mechanical and biologic creep for ultimate site closure [3]. We hypothesize that the authors achieved a median of 50% closure in the SS group compared with 0 in the traditional approach group by using progressive tensioning. There are several commercially available systems for progressive tensioning of skin, including TopClosure (IVT Medical Ltd., Ra'anana, Israel) and DermaClose (SYNOVIS Micro Alliance Companies, Inc., Birmingham, AL). Other systems work on deeper tissue, such as trans-abdominal wall traction (TAWT) for the open abdomen (Starsurgical, Inc., Burlington, WI) [4]. Not to be overlooked is the nearly ubiquitous use of negative-pressure wound therapy (NPWT) to achieve highly customizable deep and superficial tissue approximation for the purpose of gradual closure.
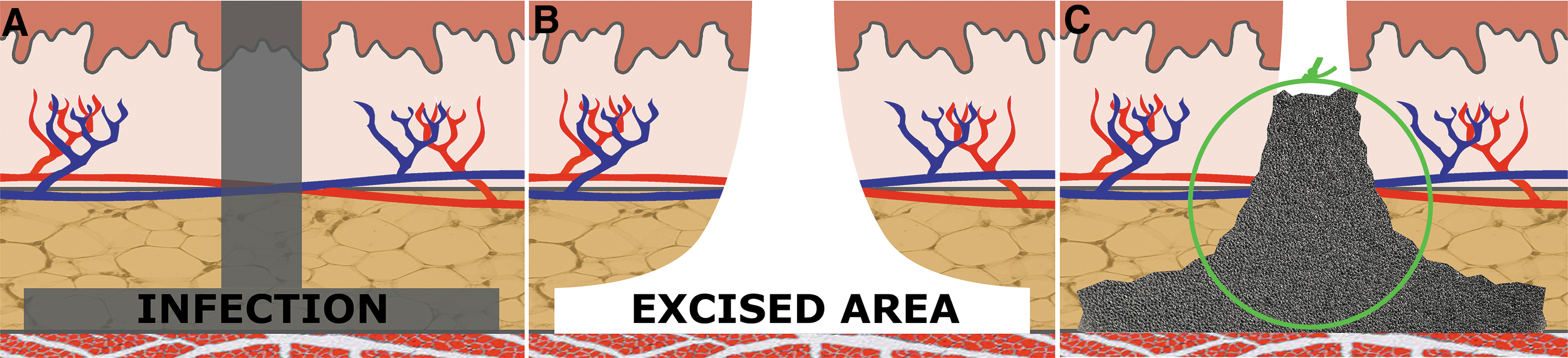
Repair of necrotizing soft tissue infection site. (A) These infections spread rapidly along the facial layer. Sentinel area of transmission has greatest vertical transmission, affecting overlying skin and soft tissue, whereas more peripheral areas have salvageable intact dermal and subdermal collateral microvasculature. (B) First phase of surgery includes source control and debridement of sentinel area and deep fascia, sparing unaffected skin and soft tissue. (C) Second phase of surgery includes using negative-pressure wound therapy with bolstering sutures (green) to narrow potential space and cause superficial and deep tissue mechanical creep, what we have termed “progressive tensioning NPWT.”
In our process at Miami Valley Hospital Regional Adult Burn and Wound Center (Dayton, OH), the initial debridement often is performed by a variety of surgeons, but with wide adoption of the SS approach, followed by a quick referral to the burn/wound surgeon (TP). Once the wound bed is clean of gross contamination, an NPWT dressing is placed within the remaining defect utilizing the V.A.C. GranuFoam dressing (KCI, an Acelity Company, San Antonio, TX). Prior to sealing the NPWT dressing, the soft tissue is approximated toward the wound center using interrupted sutures (Fig. 1C). We repeat this progressive tensioning NPWT at 4–7-day intervals, combined selectively with irrigation. Once the wound edges can be approximated directly, we perform a delayed primary closure. Although a tensioning system applied on top of the epidermis can be sufficient in superficial wounds, we have found simple sutures placed through the subcutaneous soft tissue and a black GranuFoam dressing are needed to achieve progressive tensioning at a deeper level.
In our opinion, future evolution of the SS approach to NSTI will involve multi-institutional technique sharing on progressive tensioning NPWT. The ideal techniques would allow progressive tensioning of both superficial and deep wounds in a manner that is well tolerated, fiscally responsible, cosmetically acceptable, and rapidly effective.
References
1.
TomLK, MaineRG, WangCS, et al.Comparison of traditional and skin-sparing approaches for surgical treatment of necrotizing soft-tissue infections. Surg Infect, 2019; Dec 3 doi 10/1089/sur.2019.263
2.
PerryTL, KrankerLM, MobleyEE, et al.Outcomes in Fournier's gangrene using skin and soft tissue sparing flap preservation surgery for wound closure: An alternative approach to wide radical debridement. Wounds Compend Clin Res Pract, 2018; 30:290–299.
3.
TomLK, WrightTJ, HornDL, et al.A skin-sparing approach to the treatment of necrotizing soft-tissue infections: Thinking reconstruction at initial debridement. J Am Coll Surg, 2016; 222:e47–e60.
4.
DennisA, VizinasTA, JosephK, et al.Not so fast to skin graft: Transabdominal wall traction closes most “domain loss” abdomens in the acute setting. J Trauma Acute Care Surg, 2013; 74:1486–1492.