
Abstract
Background:
Gallstones and cholecystitis are common clinical problems. There is a wide spectrum of disease severity, from rare symptoms of biliary colic to severe cholecystitis with marked gallbladder infection and inflammation that can cause life-threatening sepsis. The care of such patients is similarly varied and multi-disciplinary. Despite the prevalence of cholecystitis, there remain questions about how to manage patients appropriately.
Methods:
A multi-disciplinary team created institutional cholecystitis guidelines, and supporting evidence was compiled for review.
Results:
Even in “routine” cholecystitis, patient triage and work-up can be variable, resulting in unnecessary tests and delay to cholecystectomy. Beyond this, there are new treatment options available that may serve special populations particularly well, although the appropriate pattern of emerging endoscopic and percutaneous treatment modalities is not well defined.
Conclusions:
This review outlines evidence-based management of cholecystitis from diagnosis to treatment with a focused discussion of special populations and emerging therapies.
As many as 7%–16% of adults have gallstones [1,2], and their risk of developing a gallstone-related complication is around 7%–20% [2-6]. This incidence increases with age and is likely greater with a higher prevalence of obesity, which contributes to gallstone formation. Some estimate that there are more than 1.5 million office and emergency department visits annually in the United States for cholelithiasis, with many more visits for diagnoses that may be attributable to gallstones such as pancreatitis [7]. Cholelithiasis and cholecystitis visits and hospital admissions have been on the rise over the last decade and now are likely between 600,000 and 700,000 annually [7,8]. In a single year in the United States, there are nearly 600,000 index hospital stays and a nearly 15% re-admission rate, with a surprisingly high length of stay of 3.9 days for cholecystitis [7,8]. Cholecystitis hospitalizations alone cost > $9 billion annually [8]. Acute pancreatitis is the third leading cause of gastrointestinal admissions behind cholelithiasis [7], and gallstones are the leading cause of pancreatitis [9]. Choledocholithiasis also is encountered frequently, accounting for >125,000 hospital admissions and a similar number of cholecystectomies and endoscopic retrograde cholangiopancreatography (ERCP) procedures [10]. Clearly, gallstone disease is common, yet there is significant room for progress in the care of these patients. Because of this, high-quality guidelines are needed to inform care pathways at local institutions so outcomes for these patients may be improved [11]. This review offers an outline of common gallstone-related diseases encountered by acute care surgeons and discusses available evidence for the care of special populations and options for emerging therapies that warrant special consideration outside of traditional treatment algorithms.
Methods
A search was performed for gallstone-related diseases and divided into topics of diagnosis (history and physical examination, laboratory tests, imaging), treatment (percutaneous cholecystostomy tube, ERCP and biliary stenting, cholecystectomy, other measures), consultation, and other reviews. Supporting evidence was evaluated for relevance by a multi-disciplinary team from surgery, medicine, emergency medicine, radiology, interventional radiology, and gastroenterology. This non-systematic review focuses on the appraisal of the literature performed by this team. The strength of the recommendations was categorized as: I = generally should be performed; II = may be reasonable to perform; or III = generally should not be performed. Supporting levels of evidence were categorized as: A = systematic review of randomized controlled trials with or without meta-analysis; B = randomized controlled trials; C = systematic review of non-randomized controlled trials or observational studies, non-randomized controlled trials, group observation studies (cohort, cross-sectional, case-control); D = individual observation studies (case study/case series); or E = expert opinion regarding benefits and harm.
Diagnosis
The diagnosis of cholecystitis starts with a thorough history and physical examination. Patients typically present with abdominal pain, and the broad differential diagnosis for this problem will not be discussed in detail here. Specific to biliary pathology, right upper quadrant (RUQ) abdominal pain could be secondary to biliary-related diseases such as cholelithiasis, calculous cholecystitis, choledocholithiasis, cholangitis, gallstone pancreatitis, or non-gallstone causes of biliopancreatic obstruction. Fever should raise concern for cholecystitis, cholangitis, or pancreatitis. Jaundice should alert to the possibility of obstruction of the common bile duct (CBD) and may be confirmed with a laboratory finding of elevated bilirubin concentration and enlarged common bile duct diameter.
Laboratory evaluation should include a complete blood count (CBC) and a comprehensive metabolic panel (CMP) with particular attention paid to the white blood cell count (WBC) and bilirubin concentration. Diagnostic evaluation also will include RUQ ultrasonography (US) as the standard for initial imaging for patients with suspected cholelithiasis and cholecystitis [I-C] (Table 1). The RUQ US is sensitive for detection of cholethiasis. There are classic sonographic findings associated with acute cholecystitis (Table 2). However, US is not sensitive to these other findings of cholecystitis such as gallbladder wall edema and pericholecystic fluid, and cholecystitis should not be ruled out if these findings are absent. One large series of patients with cholecystitis confirmed by pathology examination found that just 41% of patients had classic US findings of cholecystitis in addition to cholelithiasis, and a larger meta-analysis found US has a sensitivity of 81% for cholecystitis
Strength of Recommendations and Levels of Evidence
Ultrasound Findings of Acute Cholecystitis
Sonographic Murphy's sign is maximum abdominal tenderness caused by pressure of ultrasound probe over gallbladder.
Other imaging studies that may be valuable are computed tomography (CT) and hepatobiliary iminoacetic acid (HIDA) scan. Computed tomography is poor as an adjunct for diagnosing biliary pathology and should not be performed unless other causes of abdominal pain are higher on the differential diagnosis. A HIDA scan has a high sensitivity and specificity for acute cholecystitis. The tracer is excreted by the hepatocytes into the biliary system, and non-visualization of the gallbladder indicates a blockage at the cystic duct and is consistent with cholecystitis. Meta-analysis suggests HIDA is 96% sensitive and 90% specific for diagnosing cholecystitis [13]. Despite its accuracy and utility for this purpose, HIDA has clear drawbacks, including its utilization of ionizing radiation, long examination time, and inability to investigate alternative diagnoses. It should be performed only in rare circumstances when the history, physical examination, laboratory findings, and US scans are inconclusive or discordant.
Putting the above diagnostic utilities together, the patient with classic symptoms of cholecystitis, cholelithiasis on US, persistent RUQ pain, and no other findings of acute cholecystitis on US is a common encounter. We propose offering cholecystectomy for treatment of cholecystitis if the patient is a fit operative candidate.
Treatment
Proper treatment relies on accurate recognition of a patient's underlying pathology and clinical status. Other biliary pathology may coexist, and proper treatment of each is imperative. The following discussion focuses on gallbladder pathology.
Biliary colic
The choice of treatment for biliary colic is dependent largely on symptom severity and patient tolerance. For the patient with rare and minor episodes of pain, expectant management is appropriate. Studies have followed large cohorts of patients with cholelithiasis: For those with mild symptoms, the rate of progression to worsening symptoms or cholecystitis is 25%, but more than 50% will experience resolution of symptoms [14]. Even though progression to more severe disease occurs in the minority, more than half of patients who initially undergo a watch-and-wait protocol will eventually require cholecystectomy [15]. These data should be used to counsel patients on making appropriate treatment decisions. For patients with persistent symptoms, elective laparoscopic cholecystectomy is the standard of care, as it is a safe operation and widely accessible to patients [II-C]. Elective cholecystectomy is performed as an outpatient operation and results in high patient satisfaction rates [16, 17]. These patients typically are referred to a surgeon's clinic for discussion of cholecystectomy. For patients with continuous pain that does not subside and is severe, there should be a high clinical suspicion for cholecystitis and the patient be treated as having such, even in the absence of sonographic findings of cholecystitis that extend beyond cholelithiasis (discussed above in greater detail).
Acute cholecystitis
Initial treatment of cholecystitis should follow the principles of any other infectious process and include timely initiation of antibiotics, fluid resuscitation, and pain control. For patients with signs of clinical deterioration, treatment should be in accordance with the Surviving Sepsis Campaign Guidelines [18]. Antibiotic selection is somewhat variable, although the drug chosen should cover typical enteric pathogens (Table 3) [19,20]. Local antibiotic resistance patterns differ across hospitals and regions, and physicians should consult their institutions' data for appropriate antibiotic selection. Providers should be mindful that patients may require significant fluid resuscitation secondary to an underlying infection and inflammatory response, as well as many patients having had essentially nothing by mouth for hours prior to presentation given their abdominal pain.
Antibiotic Treatment of Acute Cholecystitis
Adjust dose according
MRSA = methicillin-resistant Staphylococcus aureus.
After initial medical treatment, most patients should undergo cholecystectomy within 24 to 48 hours [I-A] (Fig. 1). The old surgeon's dogma of initial medical treatment followed by interval cholecystectomy weeks to months later to “let the gallbladder cool down” has been debunked. Early cholecystectomy (within 72 hours) compared with delayed cholecystectomy has been demonstrated to be safe in multiple randomized trials, as well as a large Cochrane review that included data from six trials [21-25]. Safety markers included 0 deaths in any of the trials, similarly rare bile duct injury (0.4%–0.9%) and similar rates of conversion to open surgery; early surgery had a four-day shorter hospitalization on average [25]. Early cholecystectomy was found to have lower morbidity than delayed cholecystectomy (14% versus 39%) in a small randomized trial of patients presenting with >72 hours of symptoms [26]. Performing cholecystectomy within 24 hours also decreases hospital length of stay as well as costs associated with cholecystitis [23].
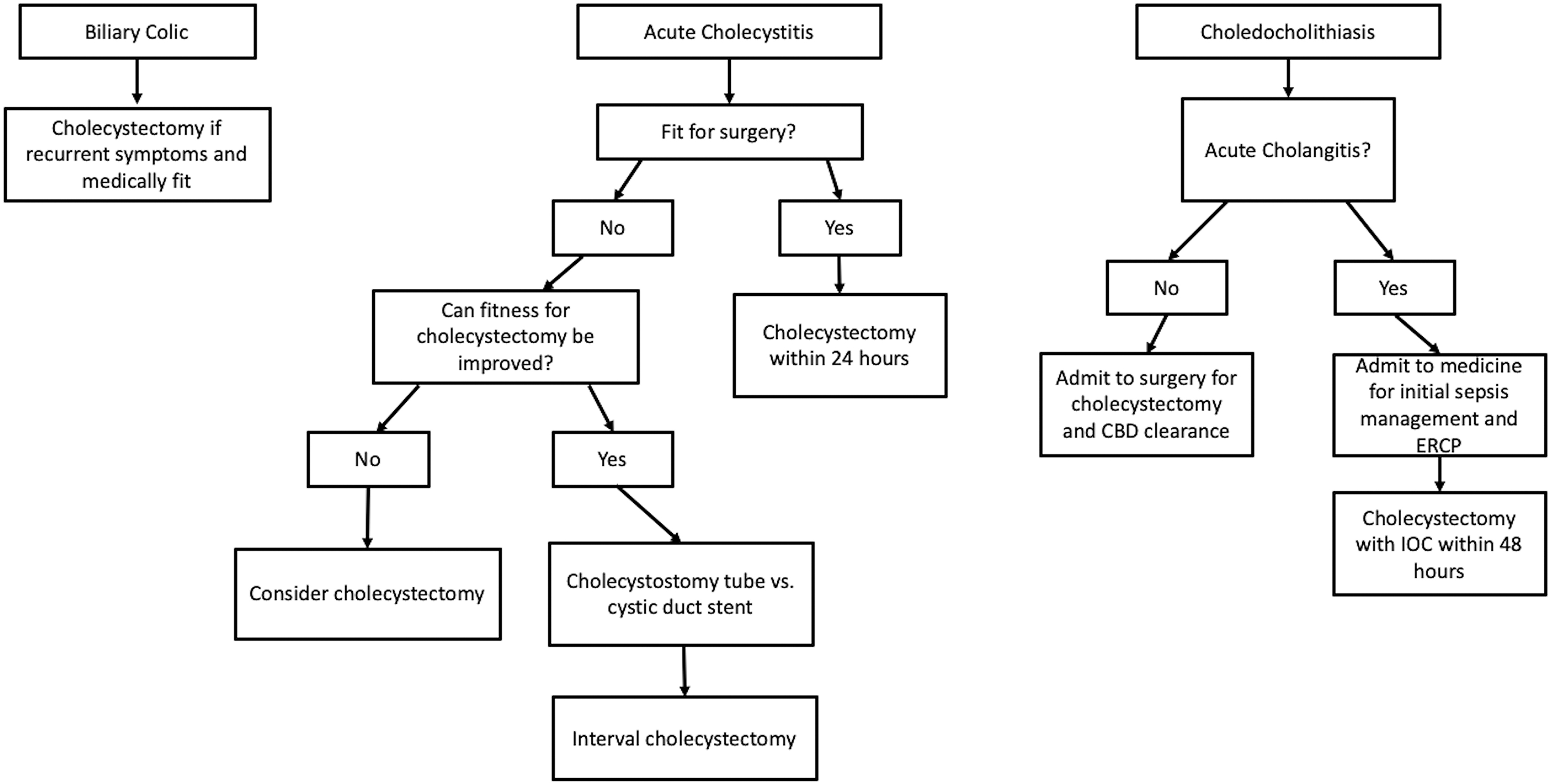
Treatment algorithms for biliary colic, acute cholecystitis, and choledocholithiasis. CBD = common bile duct; ERCP = endoscopic retrograde cholangiopancreatography; IOC = intraoperative cholangiogram.
Laparoscopic cholecystectomy has become the standard of care in preference to open cholecystectomy [27,28]. Laparoscopic cholecystectomy is as effective and as safe as open cholecystectomy but has the added benefit of lower morbidity and a shorter length of hospitalization [29,30]. Other options to achieve source control for cholecystitis are discussed below.
The utilization of alternatives to cholecystectomy is a matter of debate. The 2018 Tokyo Guidelines recommend percutaneous cholecystostomy tube placement for high-grade cholecystitis and for serious co-morbidities that make cholecystectomy unsafe [31]. The Tokyo Guidelines grade cholecystitis severity from I–III. Grade III (most severe) is based on the presence of organ system dysfunction; grade II (moderate) includes having any of WBC >18,000/mm3, palpable RUQ mass, symptom duration exceeding 72 hours, or marked local inflammation; grade I (mild) is the presence of cholecystitis but absence of any grade II or III criteria. However, determining who has moderate or severe inflammation may be difficult pre-operatively, and in a large series of cases of acute cholecystitis, cholecystectomy was found to be safe even for those with some medical co-morbidities or a severely inflamed gallbladder [12]. The most common alternative for source control is drainage of the gallbladder with a percutaneous cholecystostomy tube. Its use in special populations deemed at prohibitively high risk for cholecystectomy is discussed below.
Post-operatively, patients typically recover well. The safety of early laparoscopic cholecystectomy has led to significant cost savings and shorter hospital stays. “Enhanced recovery pathways” or “fast-track protocols” similarly have been demonstrated both to be safe and to result in significantly shorter lengths of stay and cost savings after laparoscopic cholecystectomy [32]. These post-operative care pathways typically target prompt transition to oral intake, cessation of intravenous fluids, early ambulation, and limiting intravenous opioid use. Patients undergoing urgent laparoscopic surgery may even qualify for same-day discharge or require a single-night admission to the hospital. Post-operative opioid requirements for pain control likely are much lower than previously thought, especially when adjuncts such as ibuprofen and acetaminophen are prescribed liberally [33]. This gives the surgeon peace of mind to prescribe lower opioid doses safely, while maintaining high satisfaction and pain control [34]. This is an important consideration given the risk of new persistent opioid use after even minor operations [35]. Patients should receive 0–10 tablets of 5 mg of oxycodone for the opioid-naïve after laparoscopic cholecystectomy [36].
Choledocholithiasis
This review focuses on cholecystitis. However, not infrequently, physicians find themselves needing to rule out choledocholithiasis while caring for a patient with biliary colic or cholecystitis. Patients with cholangitis should be treated with prompt biliary decompression (Fig. 1). Early recognition is important because of the risk that choledocholithiasis will cause cholangitis or gallstone pancreatitis if left untreated. The risk of choledocholithiasis without cholangitis is summarized in Table 4 [37]. For patients at high risk of choledocholithiasis, the biliary system should be evaluated, most commonly with an intra-operative cholangiogram (IOC) done at the time of cholecystectomy or ERCP. If common duct stones are discovered, the CBD should be cleared [I-A]. This clearance may be done at the time of cholecystectomy with flushing attempts or a laparoscopic common bile duct exploration, which can clear the common duct of stones effectively [38]. Another diagnostic and therapeutic option is ERCP, which could be done either during the same anesthesia episode as cholecystectomy or peri-operatively. If performed during cholecystectomy, it saves the patient an extra episode of anesthesia and is cost containing [39]. Both options are effective, with similar complication rates although they require technical expertise and so should be performed by those with adequate experience [38]. Routine IOC during cholecystectomy is controversial, and it is unclear if it improves outcomes significantly compared with selective IOC for detection of CBD stones [40,41]. Routine IOC has not been shown to decrease the rate of bile duct injury, and it leads to longer operating times and higher costs [42,43]. If there is a low likelihood of choledocholithiasis, we do not recommend routine IOC [III-B].
Probability of Choledocholithiasis
Acute cholangitis
If a gallstone passes into and obstructs the common bile duct, acute cholangitis can ensue. These patients are at high risk of death without prompt antibiotics and biliary decompression and often require critical care resources [44]. This review focuses on cholecystitis, although patients with cholecystitis and cholelithiasis are at risk for concomitant choledocholithiasis; and, given the urgency of attention that cholangitis demands, it is worth discussing briefly.
Classically, the diagnosis was based on Charcot's triad, namely jaundice, fever, and RUQ pain. However, this is not sensitive [45]. The 2013 Tokyo Guidelines on cholangitis have been validated in a series of more than 6,000 patients as yielding a much higher rate of diagnosis of 90% [45]. These criteria rely on evidence of systemic inflammation (fever, shaking chills, or laboratory evidence), cholestasis (jaundice or abnormal liver function tests), and imaging findings (biliary dilation or evidence of obstructive etiology such as stone or stricture) [44]. Imaging investigation begins with abdominal US, although reports show differing success rates; it is highly specific for bile duct dilation and stones, although some investigators have reported a sensitivity of just 42% for biliary dilation in a meta-analysis [46], whereas others have shown a sensitivity of 98% for choledocholithiasis in patients with obstructive jaundice [47]. Reliable results of US are likely operator and patient dependent. Still, given its ready availability, it is likely the best first test to obtain prior to moving on to other imaging studies if necessary. Computed tomography is another option that affords the option to evaluate other causes of abdominal pain more thoroughly. Despite its poor sensitivity to gallstones, as outlined above, CT will demonstrate biliary dilation readily if it is present. Another option is magnetic resonance cholangiopancreatography (MRCP), but it is time and labor intensive and can result in delays in diagnosis and treatment and so should be used only in carefully selected cases.
Once the condition is diagnosed, biliary decompression should be pursued swiftly (Fig. 1). Prompt drainage can improve mortality outcomes as well as reduce hospital length of stay [45,48]. The largest review of patients with cholangitis suggested that there is a mortality benefit specifically for those with moderate cholangitis based on the Tokyo Guidelines classification when ERCP is performed within 24 hours [45]. In an effort to reduce gallstone-related complications, cholecystectomy should be performed after patients have recovered from acute cholangitis, prior to hospital discharge [I-C]. The largest trial to guide decision making comes from the PONCHO trial, which compared same-admission cholecystectomy with interval cholecystectomy at 4 weeks after gallstone pancreatitis [49]. The incidence of a recurrent gallstone event within 4 weeks without cholecystectomy was 17%, but this was was reduced to 5% with same-admission cholecystectomy. Although these data are from a gallstone pancreatitis population, we believe the principles likely carry weight in patients with cholangitis. Although the data are not evidence from a randomized trial, this view that earlier cholecystectomy reduces gallstone events is supported in large reviews of cholangitis and choledocholithiasis [50,51].
Special Populations
Pregnant women
Gallstones are more common during pregnancy and are associated with adverse maternal and neonatal outcomes [52]. Providers and patients alike tend to overestimate significantly the risks of diagnostic tests and intervention for non-obstetric health problems occurring in pregnancy, leading to delays in therapy or to undertreatment [53]. Leukocytosis is normal during pregnancy (normal range 9,000–15,000 cells/mcL), which reduces the utility of this test to diagnose cholecystitis. The American College of Obstetricians and Gynecologists suggests US should be performed only when clinically indicated; but it does not use ionizing radiation, and there have been no documented adverse effects to the fetus of US used for maternal diagnosis. This opinion has been endorsed by the American College of Radiology [54]. Magnetic resonance imaging (MRI) with gadolinium contrast medium has fetal risks, but non-contrast MRI is safe [55]. Use of HIDA scans is more controversial, although the fetal risk likely is small and difficult to quantify [56,57]. The fluoroscopy required for ERCP will result in low doses of radiation to the fetus, although if a therapeutic ERCP is needed, the benefits to the mother and fetus of treating the biliary pathology likely outweigh the risks [58,59]. Strategies such as preprocedural MRCP and endoscopic US could limit fluoroscopy times during ERCP and any perceived fetal radiation risk. Penicillins and cephalosporins generally are considered safe antimicrobial coverage during pregnancy. If the patient has an anaphylactic penicillin and cephalosporin allergy, clindamycin or aztreonam with metronidazole are acceptable alternatives; ciprofloxacin is potentially teratogenic.
Biliary colic should be managed on an individual basis; providers should weigh the benefit of symptom control with the risks of miscarriage and teratogenesis in the first trimester and pre-term labor in the third trimester [60,61]. Any necessary cholecystectomy for biliary colic should be performed during the second trimester when possible. If RUQ pain persists or recurs frequently, the woman should be re-evaluated for development of complications and cholecystitis. A large study of pregnant women in Australia who had gallstone disease showed that most of them were identified in their third trimester, with 97.8% having the diagnosis made in the 34th week of gestation or later; and having gallstones was associated with adverse maternal and neonatal outcomes [52]. For women in the third trimester, the decision to perform cholecystectomy or wait until the post-partum period is contentious, and practice patterns differ, although recent evidence from a large California state database suggests cholecystectomy during the third trimester increases the rate of pre-term delivery (in addition to hospital length of stay and maternal re-admissions) compared with initial non-operative management followed by post-partum cholecystectomy. Other outcomes such as length of stay, re-admission, and open surgery favor delaying cholecystectomy to the post-partum period [61-63]. Conflicting evidence from Australia found no difference in pre-term delivery rate for operative versus medical management [52]. When cholecystectomy is performed during pregnancy, there is an approximately 5% rate of adverse obstetric-related outcomes (pre-term delivery or pre-term labor during the third trimester and miscarriage during the first and second trimester) in the Nationwide Inpatient Sample (this study sample included appendectomy as well as cholecystectomy) [64]. Perhaps alternative therapies such as cystic duct stenting or cholecystostomy tubes have a role in bridging to the post-partum period, and this option warrants additional investigation.
Chronic illness
Any surgeon treating a patient with cholecystitis must decide if the risks of cholecystectomy are worth the benefit of definitive management by removing the gallbladder. Clearly, in a patient with no co-morbidities, the optimal treatment is cholecystectomy. However, patients with significant co-morbidities have a heightened risk of morbidity or death from general anesthesia or surgery. Numerous risk calculators exist to aid in this treatment decision [65]. These are imperfect although being refined continually [66-68].
There are several key questions to address. If there is a modifiable risk factor, such that delaying surgery and intervening on the co-morbidity would make cholecystectomy significantly safer at a later date, initial non-operative management is appropriate. A good example of this would be a patient receiving anticoagulation therapy for atrial fibrillation, which can be held safely peri-operatively [69]. Other modifiable co-morbidities could warrant delaying surgery if it changes the associated risk.
The typical bridge treatment to cholecystectomy is a cholecystostomy tube. Such tubes have a high technical success rate and typically are used in patients with co-morbidities such as old age, coronary artery disease, cirrhosis, atrial fibrillation, congestive heart failure, or sepsis [70-72]. Utilization took a sharp rise after release of the 2007 Tokyo Guidelines, which recommended cholecystostomy tube placement for high-grade cholecystitis [73]. Reported mortality rates differ after cholecystostomy tube placement. Some studies show the tubes are associated with a high mortality rate, although this likely is biased by the selection of sicker patients to receive cholecystostomy tubes [73,74]. Medicare claims data looking at patients with high-grade cholecystitis found a 47% 90-day mortality rate for patients who were treated with a cholecystostomy tube [73].
Despite the high technical success rate, the tubes have a high rate of post-procedure problems including dislodgement (40%–50%), bile leaks, long hospital stay, and a high re-admission rate compared with definitive cholecystectomy [73,75]. The high complication rate leads to a similarly high rate of re-intervention [76]. Additionally, around 40% of patients initially treated with a cholecystostomy tube eventually will undergo cholecystectomy [72,73,77]. This practice of avoiding an interval cholecystectomy likely is appropriate for patients with acalculous cholecystitis. However, in several large series, around 25% of patients with calculous cholecystitis re-present with cholecystitis if they did not undergo cholecystectomy, and cholecystectomy reduces the risk of recurrent biliary events [73,74,76]. Because of the risk of recurrent cholecystitis, the frequent need for cholecystectomy, and the high complication rate of cholecystostomy tubes, we advocate consideration of early cholecystectomy in lieu of a cholecystostomy tube [II-D]. For patients whose fitness for surgery may be optimized in the time after initial presentation of cholecystitis, a temporizing cholecystostomy tube is appropriate as a bridge to cholecystectomy (Fig. 1). A common example of this is a patient with a recently placed drug-eluting coronary stent who is on dual antiplatelet therapy (DAPT); bridging with cholecystostomy so the cholecystectomy may be performed when DAPT is no longer necessary could be ideal. If the risk profile for cholecystectomy cannot be improved, consideration should be given to early surgery [12].
Patients with cirrhosis also represent a unique population for whom treatment of cholecystitis should be altered. For patients with compensated cirrhosis, we still advocate cholecystectomy. In decompensated cirrhosis, as evidenced by portal hypertension, ascites, and thrombocytopenia, a cholecystostomy tube could be uniquely problematic because of the risk of ascites leak that is difficult to resolve or a more devastating complication of seeding the ascites with bacteria during the procedure. Peri-portal varices also can increase the risk of significant bleeding with cholecystectomy or a cholecystostomy tube. For these patients, co-management with a hepatologist is warranted, and endoscopic treatments such as a transpapillary cystic duct stent (see below), which does not violate the peritoneal cavity, is a treatment option for patients with decompensated cirrhosis as a bridge to liver transplant or as terminal therapy for those with end-stage liver disease [78-80].
With these considerations in mind, most patients may undergo cholecystectomy safely despite high-grade cholecystitis or co-morbidities [12]. The general safety of cholecystectomy coupled with the high complication rate of the cholecystostomy tube has led us to favor cholecystectomy and reserve tube placement for those with modifiable risk factors that will change the risk profile of cholecystectomy significantly and for patients with a limited life expectancy, for whom a cholecystostomy tube would be definitive therapy. For patients with calculous cholecystitis initially managed with a cholecystostomy tube, the high rate of biliary complications and subsequent re-interventions mandate that these patients receive meticulous follow-up care after hospital discharge and strong consideration for eventual cholecystectomy. Clearly, though, the severity of cholecystitis and of risk factors lie on a wide spectrum mandating that treatment be tailored to the individual patient.
Emerging Therapies
Endoscopic therapies
Numerous endoscopic therapies have emerged as treatment options for patients with cholecystitis and have the common goal of draining the gallbladder enough to obtain source control and decompress the organ. One such example is a transpapillary cystic duct stent in which an ERCP is performed, the cystic duct is cannulated, and a stent is placed in the cystic duct for gallbladder decompression. This treatment has been described for patients with cirrhosis as well as other significant medical co-morbidities and seems to be a useful treatment option for such patients [78,79,81]. Long-term data on stent patency and re-intervention rates are sparse, although re-intervention rates appear to be much lower than for cholecystostomy tubes [82]. Transmural gallbladder drainage is another possible endoscopic treatment in which the gallbladder is visualized using endoscopic US and accessed endoscopically via a transgastric or transduodenal approach, and a lumen-opposing metal stent is placed. This typically is attempted if transpapillary cystic duct stent placement is unsuccessful [83-85] or when there is a large burden of cholelithiasis, as the stents can be as much as 2 cm in inner diameter [86]. These alternative therapies have been used for patients deemed unfit to undergo cholecystectomy. Typically, this population previously has undergone cholecystostomy tube placement, and endoscopically placed stents have a clear benefit of internal drainage without the need for external tubes that can be burdensome to patients. These catheters and stents are difficult to place and require an endoscopist skilled in advanced endoscopic therapies, which limits accessibility for patients being treated at hospitals without an experienced endoscopist. However, the technical success rate has been high in experienced hands [81,85].
These treatments do carry with them a risk of pancreatitis, bleeding, and luminal perforation, which differs according to the procedure. Meta-analysis comparing transpapillary drainage and transmural gallbladder drainage found a technical and clinical success rate of 83% and 88% for transpapillary drainage and 95% and 97% for transmural drainage, respectively. Pancreatitis risk is highest in transpapillary drainage (5.1%), whereas transmural drainage carries a higher risk of bleeding (4.3%) and perforation (3.7%) [87]. Compared with cholecystostomy tubes, endoscopic therapies require half of the re-interventions, have shorter hospital stays, and cause less pain [82]. These options could be useful especially for patients who require a bridge to cholecystectomy with ascites, or for those who will never be a surgical candidate, including patients with terminal illnesses who may avoid a cholecystectomy and thus external drainage and the complications that go with cholecystostomy tubes [II-D]. If an endoscopic treatment is the destination therapy, and the patient will never be a candidate for cholecystectomy, transmural drainage with a stent could be a better option because it has a lower rate of long-term stent or catheter occlusion compared with transpapillary drainage (12% versus 3%; odds ratio 0.33) [88,89]. If used as a bridge to cholecystectomy, a surgeon and endoscopist may elect transpapillary drainage, given its lower risk of bleeding and perforation. These decisions should be individualized and made between surgeons, gastroenterologists, and patients with a longitudinal treatment plan in mind.
Percutaneous therapies
The cystic duct also may be accessed percutaneously via either a transhepatic or a transcholecystic approach, although these approaches have been described only in relatively small case series [90]. Patients with cholecystostomy tubes require diligent management, including follow-up intervention. Especially after the percutaneous tract has formed and epithelialized, an option at subsequent interventions is to internalize the drainage by placing a cystic duct stent. This obviates the nuisance of patients having to be concerned about having an external drain. Similar to endoscopically placed stents, these are technically challenging procedures and require an experienced interventional radiologist. Given the technical difficulty of both, an option that has been described to increase the success of cystic duct stent placement is to access the cystic duct percutaneously and place the stent endoscopically via a rendezvous approach [91]. This is a burgeoning idea with literature filled with low-quality data and small case series. Robust data on long-term patency, re-intervention rates, and long-term success are limited for this technique. making review and recommendations on its use difficult.
Conclusion
Gallstones and cholecystitis are common clinical problems. There is a wide spectrum of disease severity, from rare symptoms of biliary colic to severe cholecystitis with marked gallbladder infection and inflammation that can cause life-threatening sepsis. The care of such patients is similarly varied and multidisciplinary. Despite the prevalence of cholecystitis, there are improvements that can be made in the care of these patients. Questions remain on the optimal treatment of special patient populations, and there are new treatment options available that may serve these special populations particularly well. As experience continues to grow and be studied, optimal care pathways may be established.
Footnotes
Author Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors have no competing financial interests.