
Abstract
Background:
Mesh infection is a serious complication of inguinal hernia repair, but surgeons have not reached a consensus on the method of treatment. The aim of this study was to assess the outcomes of maximal mesh removal therapy with methylene blue injection for mesh infection after inguinal hernia repair.
Patients and Methods:
The study was a monocentric retrospective analysis following STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statements of all patients with mesh infection undergoing maximal mesh removal operation with methylene blue injection. Demographics, mesh infection characteristics, microbiology, early post-operative data, and follow-up data were recorded.
Results:
Sixteen patients underwent complete removal of infected mesh and 13 had partial removal. The operation time was 76.3 ± 26.0 minutes. In 13 patients the cultures tested positive, five for Staphylococcus aureus. Twelve participants developed surgical site infection post-operatively and eventually healed after 27.4 ± 16.3 days of dressing. In a mean follow-up of 46 months, one patient suffered chronic pain and one had chronic sinus in the partial removal group, although none did in the complete removal group, without a statistically significant difference. No hernia recurrence occurred.
Conclusions:
Maximal mesh removal therapy with methylene blue injection can be considered as a feasible alternative for the treatment of mesh infection.
More than 20 million abdominal wall hernias are repaired worldwide yearly and inguinal hernia is the most common type accounting for approximately 70% of all hernias [1,2]. Currently, open tension-free repair using mesh has become the standard treatment for inguinal hernia because of low recurrence rate [3]. Although mesh repair has some advantages, several mesh-related complications are reported. Mesh infection is a serious complication of synthetic repair and most surgeons suggest mesh removal therapy for mesh infection [4,5]. However, some researchers indicate conservative treatment is also an option for these patients [6]. So far, there is no consensus on the treatment of mesh infection [7].
Methylene blue is a biologic dye, which can be used in the treatment of infections such as joint, urinary tract, and endodontic infections [8–11]. Although some surgeons utilize mesh removal therapy for mesh infection, currently there is no literature regarding mesh removal therapy with methylene blue injection [4,5,12]. Methylene blue injection into the sinus orifice can make the sinus and the infected patch blue-stained, and then clear the scope of resection and cure the infection factors. Maximal mesh removal means to remove the infected mesh as completely as possible or partially when part of the mesh is well incorporated. The aim of this study was to assess the outcomes of maximal mesh removal therapy with methylene blue injection for mesh infection after inguinal hernia repair.
Patients and Methods
Study design
The study was a monocentric retrospective analysis following STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statements of all patients with mesh infection undergoing mesh removal operation with methylene blue injection from February 2014 to May 2016 in The First Affiliated Hospital of Zhengzhou University. Demographics, mesh infection characteristics, and microbiology were documented in the medical charts and operative reports. In May 2019 participants were invited to the outpatient clinic for a clinical examination and questioned about operative outcomes. Follow-up data of those who did show up were collected by telephone interviews. Two residents performed the investigations and knew about the main content of this study and parameters in follow-up.
Operative procedure
All operations were performed under general anesthesia by one surgeon. Methylene blue was injected into the sinus orifice. We incised the skin and scar tissue along the blue-stained sinus until the abscess cavity. The pus was sent for culture. We attempted to excise the whole infected mesh and blue-stained infectious tissue (Fig. 1). Partial mesh removal was applied if part of the mesh seemed well incorporated. The incision was washed repeatedly with normal saline and hydrogen peroxide. We placed a closed vacuum drain in the abscess cavity and restored the strong scarred fascia with 2/0 polypropylene suture. Finally, the subcutaneous scar tissue and skin were sutured. In cases of large abscess cavity or severe infection, we packed the incision with gauze during the operation and performed secondary sutures after incision condition improved. After the operation, cefoperazone sodium and sulbactam sodium were used intravenously, and the appropriate antibiotic agents were selected according to the results of bacterial culture and drug sensitivity test.

Surgical procedure of infected mesh removal using methylene blue. (
Data analysis
Demographic data included gender, age, body mass index (BMI), and comorbid conditions. Data regarding mesh infection characteristics consisted of surgical site infection history after last repair, mesh infection duration, abscess cavity diameter, mesh type, removal type, drainage, operation time, and post-operative antibiotic agents. Early post-operative data included surgical site infection, seroma, hematoma, and hospital stay. Follow-up data comprised hernia recurrence, chronic pain, and chronic sinus. Surgical site pain was assessed by visual analog scale (VAS, 0–10) and chronic pain was defined as pain (VAS ≥3) lasting at least three months post-operatively. If recurrent hernia could not be determined by patient's complaint and physical examination, radiologic examination was applied.
Statistical methods
Data were analyzed with SPSS, version 19.0 (IBM Corp, Armonk, NY). Continuous parameters were presented as mean values ± standard deviation and categorical parameters were listed as numbers with percentage in parenthesis. We used Pearson χ2 test or Fisher exact test for categorical parameters. P < 0.05 was considered statistically significant.
Results
Patient demographics
Twenty-nine patients (age, 47.7 ± 20.1 years; BMI 24.3 ± 1.9 kg/m2) were included in this study, two of whom were female. There were seven smokers, two patients with hypertension, and one participant with chronic obstructive pulmonary disease (Table 1). A flow chart of this cohort is provided in Figure 2. One patient died and one participant could not be contacted. Two patients were interviewed by telephone.
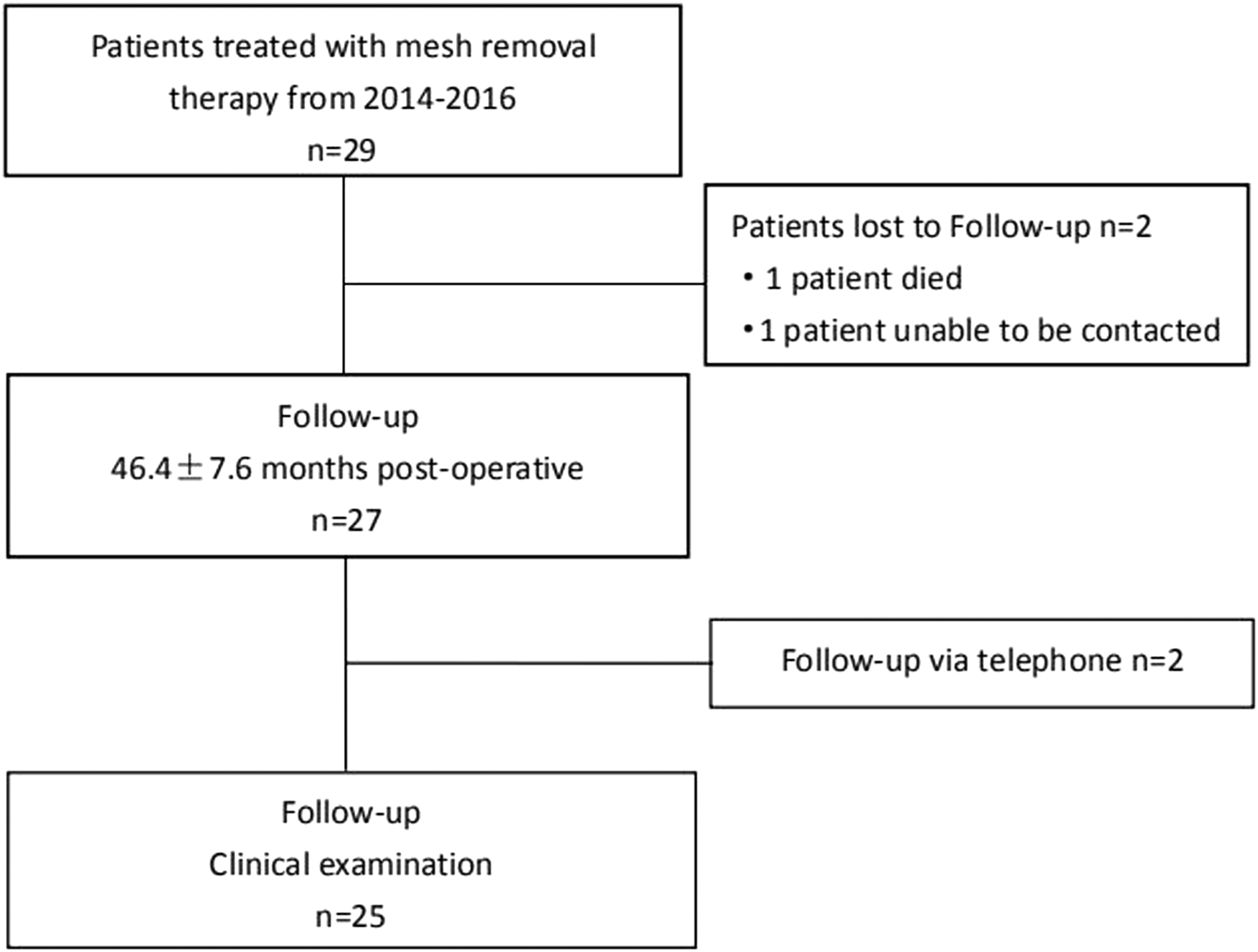
Study flow chart of 29 patients treated with maximal mesh removal therapy using methylene blue for mesh infection after inguinal hernia repair.
Patient Demographics
Values in parenthesis are percentages unless indicated otherwise.
BMI = body mass index.
Values are mean ± standard deviation
Mesh infection characteristics
The use of prophylactic antibiotic agents was recorded in nine patients during the last repair. Eleven patients had surgical site infection history after the last repair and median duration of mesh infection was four months. The diameter of the abscess cavity was 36.5 ± 25.4 mm. Sixteen persons underwent complete removal, 13 with partial removal. There were three types of infected mesh removed: plug (n = 7), flat patch (n = 18), and plug plus patch (n = 4). They were all made of polypropylene. Drains were placed in 26 patients, while the incisions of three participants were packed with gauze. The operation time was 76.3 ± 26.0 minutes and post-operative antibiotic agents were used for 9.5 ± 2.5 days. These data are provided in Table 2.
Mesh Infection Characteristics
Values in parenthesis are percentages unless indicated otherwise.
Values are median.
Values are mean ± standard deviation.
Microbiology of mesh infection
In 13 patients the cultures tested positive, five for Staphylococcus aureus. Other bacteria included Klebsiella pneumoniae, Escherichia coli, Enterococcus faecalis, and Staphylococcus epidermidis. These data are presented in Table 3.
Microbiology of Mesh Infection
Values in parenthesis are percentages unless indicated otherwise.
Early post-operative data
Twelve participants had surgical site infection postoperatively and eventually healed after 27.4 ± 16.3 days dressing. The length of hospital stay was 19.4 ± 7.4 days. These data are provided in Table 4.
Early Post-Operative Data
Values in parenthesis are percentages unless indicated otherwise.
Values are mean ± standard deviation.
Literature follow-up data of mesh removal therapy
In the follow-up of 46.4 ± 7.6 months, one participant experienced mild chronic pain and one had chronic sinus on operation site. No hernia recurrence occurred in our study. Follow-up data of mesh removal therapy without methylene blue injection are provided in Table 5.
Literature Follow-Up Data of Mesh Removal Therapy
Values in parenthesis are percentages unless indicated otherwise.
NG = not given.
Analysis of removal type for early post-operative and follow-up data
Seven patients in the complete removal group and five in the partial removal group had surgical site infection; no difference was verified. One patient suffered chronic pain and one had chronic sinus in the partial removal group, whereas none did in the complete removal group, without a statistically significant difference. These data are presented in Table 6.
Analysis of Removal Type for Early Post-Operative and Follow-Up Data
Discussion
Mesh infection is a serious complication of synthetic repair and its risk factors include diabetes, obesity, smoking, chronic obstructive pulmonary disease, and immunosuppressive therapy [13,14]. Regarding treatment, different methods were proposed recently. Meagher et al. [6] treated 11 patients with mesh infection conservatively by negative pressure wound therapy, local surgical site care, and antibiotic agents. Berrevoet et al. [15] suggested that negative pressure therapy was effective for salvage of deep infected meshes, particularly when large-pore mesh was applied. Sabbagh et al. [16] reported 23 patients who underwent partial removal of mesh and concluded that partial removal of mesh was feasible in the treatment of mesh infection. Birolini et al. [17] presented chronic mesh infection could be treated by removal of the infected mesh and simultaneous mesh replacement, which cured 95% of patients after a mean follow-up of 74 months. In addition to these trials, some surgeons applied the mesh removal therapy for mesh infection without methylene blue injection [4,5,12]. Our study was to assess the outcomes of maximal mesh removal therapy with methylene blue injection for mesh infection after inguinal hernia repair.
In this study, the use of prophylactic antibiotic agents was recorded in nine of 29 patients. It was reported that the rate of mesh infection in patients undergoing prosthetic repair was 1.4% in the antibiotic group and 2.9% in the control group. The authors concluded that routine antibiotic prophylaxis could not be recommended to reduce the infection rate in hernia repair [18]. In clinical centers with low rates of surgical site infection, there is no indication for the routine use of prophylactic antibiotics in elective open or endoscopic inguinal hernia repair in low-risk patients. In the presence of risk factors, such as recurrence, advanced age, immunosuppressive conditions, long operation time, or use of drains, the use of antibiotic prophylaxis could be considered [19].
Our research revealed the cultures tested positive in 13 patients, five for Staphylococcus aureus. Other bacteria included Klebsiella pneumoniae, Escherichia coli, Enterococcus faecalis, and Staphylococcus epidermidis. In the bacteriologic analysis by Sabbagh et al. [16], germs were found in 15 patients, eight for Streptococcus. In research by Akyol et al. [12], 15 complete infected mesh removals were performed, and bacterial isolates were obtained in six patients. Four cultures were positive for Staphylococcus aureus, one for Escherichia coli, one for coagulase-negative staphylococci. It is known that Staphylococcus aureus is the common bacteria in mesh infection and can form biofilm on the surface of patch, resulting in low detection rate of bacterial culture [20].
In this research, 12 participants had surgical site infection post-operatively and eventually healed after 27.4 ± 16.3 days dressing. Regarding the study by Fawole et al. [5], 14 patients with mesh infection had mesh removals and no peri-operative complications occurred after mesh removal. In our study, one participant had chronic sinus on operation site during follow-up. Regarding the study by Akyol et al. [12], no chronic sinus occurred in follow-up. In the research by Chung et al. [21], 10 partial and eigh total mesh excisions were done for chronic mesh infection after abdominal wall hernia repair. At follow-up, three in total and seven in partial excision group had sinus on operation site, without a statistically significant difference. Patients undergoing partial excision of the infected mesh may have problems with a discharging sinus because of the small fragments of mesh left. However, persons with complete mesh excision may also have the risk of developing a wound sinus, which may be related to chronic infection of sutures for the defect closure [21]. In addition to the infectious mesh, the surrounding blue-stained tissue was also excised in our trial. This process, which eradicated infectious factors, might have something to do with the low incidence of chronic sinus.
In our series, no hernia recurrence occurred in 46 months of follow-up. Regarding the work by Akyol et al. [12], one patient developed recurrent hernia in 62 months of follow-up. In the work by Chung et al. [21], three in the partial mesh excision group and three in the complete mesh excision group had recurrent hernia in 19 months of follow-up. Fawole et al. [5] found two recurrences in 44 months of follow-up. In our study, we restored the strong scarred fascia with 2/0 polypropylene suture. The inflammatory cell infiltration occurs after prosthetic mesh implantation, and fibroblast infiltration gradually replaces inflammatory cells through the mesh pores. The mesh incorporates into the surrounding tissue by fibrous infiltration and the neo-fascia formation [12,22]. Polypropylene mesh was applied in all patients in this study. The strength of prosthetic repair lies in the fibrous reaction induced by the mesh rather than the mesh itself, therefore, mesh removal may not necessarily result in hernia recurrence if sufficient fibrous scarring remains [4].
In our study, one participant suffered mild chronic pain in follow-up. Delikoukos et al. [4] reported that five patients with mesh infection underwent complete mesh removals and none had chronic pain in 22 months of follow-up. In the study by Akyol et al. [12], one person reported a burning sensation on operation site. In follow-up of the work by Fawole et al. [5], no one had chronic pain. In this trial, we excised not only the infectious mesh but also the surrounding blue-stained tissue during operation, which might increase the incidence of nerve injury. In addition, the follow-up time and diagnostic criteria of chronic pain were different among these studies.
Our research does have some limitations. First, it is a retrospective cohort study. Second, the sample size is small and mean follow-up of 46 months is insufficient to assess the outcomes. In addition, hernia recurrence may be asymptomatic and only can be detected by ultrasound examination.
Conclusions
Maximal mesh removal therapy with methylene blue injection has demonstrated reasonable results in this study. Our research is a retrospective trial with a small number of patients, and large-scale randomized controlled trials with long-term follow-up are essential to evaluate the post-operative outcomes such as hernia recurrence and chronic pain further. Maximal mesh removal therapy with methylene blue injection is a safe and promising technique and can be considered as a feasible alternative for the treatment of mesh infection after inguinal hernia repair.
Funding Information
The study was funded by Scientific and Technological Development Project of Henan Province in 2017 (Number: 172102310274).
Footnotes
Author Disclosure Statement
No competing financial interests exist.