
Abstract

To the Editor:
A
Case Report
Acute respiratory failure developed in a 71-year-old male on hospital day (HD) 11 that necessitated endotracheal intubation and mechanical ventilation after a total pelvic exenteration, muscle flap closure, and abdominal wall reconstruction for a perineal recurrence of rectal adenocarcinoma. He had a long history of Crohn colitis, which had been managed surgically by total abdominal colectomy with end-ileostomy in 1982 (age 39), and after development of adenocarcinoma in the rectal stump, by neoadjuvant chemoradiation followed by abdominoperineal resection in 2015 (age 66).
The patient's past medical history included a homozygous factor V Leiden mutation with multiple previous episodes of lower extremity deep venous thrombosis. For anticoagulation, the patient had received heparin intravenously in the peri-operative period, and the etiology of respiratory failure was determined to be multi-factorial (post-operative delirium, oversedation from polypharmacy, and profound post-operative weakness) after venous thromboembolism was excluded.
The patient was extubated to intermittent non-invasive ventilation with bi-level positive airway pressure (BiPAP) on HD 15. He continued to require intermittent BiPAP over the next five days. On HD 20, fever to 39.0°C developed as well as left pre-auricular induration and erythema. Purulent fluid was expressed from the Stensen duct. Linezolid and meropenem were administered after fluid was cultured. Neither ultrasound nor maxillofacial computed tomography (Fig. 1) demonstrated an abscess.
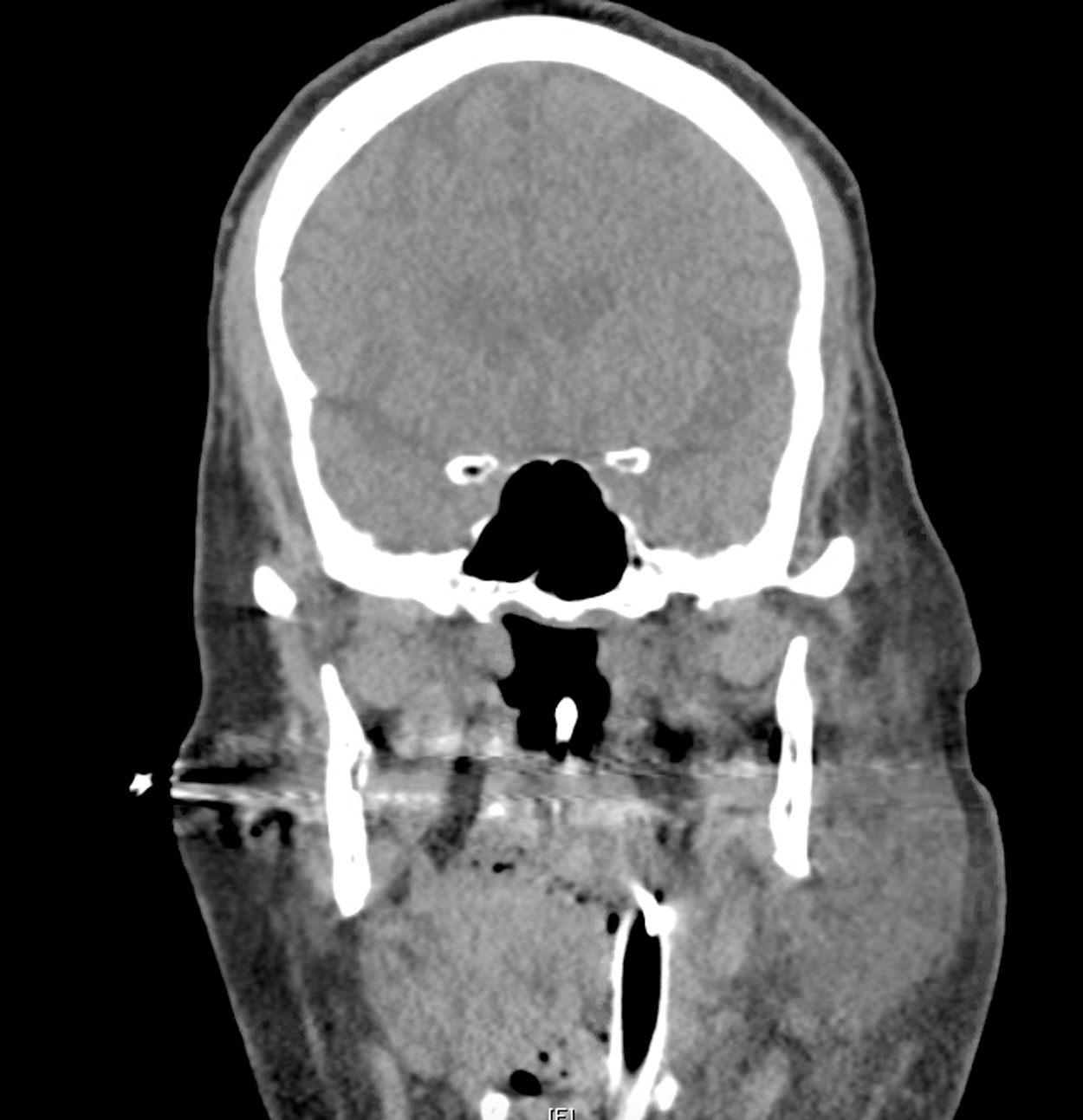
Acute parotitis with swelling of the left parotid gland.
Duct fluid yielded MRSA and C. glabrata, and blood cultures also yielded C. glabrata, so meropenem was changed to micafungin. The parotitis improved over the next two weeks with anti-infective agents, warm compresses, and parotid massage, and the patient was transferred to a rehabilitation facility.
Discussion
Acute parotitis can be caused by bacterial or viral (e.g., mumps orthorubulavirus, human immunodeficiency virus, and Epstein-Barr virus, among others) pathogens, but it is usually an acute bacterial infection [2]. Infection can be complicated by abscess formation or may progress into the parapharyngeal space or rarely the mediastinum [3]. Other rare complications of acute parotitis include internal jugular infective thrombophlebitis (Lemierre syndrome, usually associated with Fusobacterium necrophorum) [2] or facial nerve palsy secondary to mass effect (abscess or edema) [4].
Risk factors for parotitis in post-operative patients include dehydration foremost, but additionally older age, prolonged endotracheal intubation, anti-cholinergic agents, oral cavity neoplasm, or obstruction of the Stensen duct [2]. Pathogenesis is likely related to retrograde ascension of bacteria from the buccal mucosa along the Stensen duct. Diagnosis is usually clinical, but patients may need imaging to evaluate for fluid collections. Treatment consists of appropriate antimicrobial therapy, parotid massage, and sialogogues, plus drainage of appreciable fluid collections if indicated [1,2].
This case is unique for several reasons. First, a mixed bacterial and fungal parotid infection developed in our patient, heretofore unreported. Candida spp. rarely cause acute parotitis, with only four cases reported previously [4–7]. Only a single, fatal case of parotitis because of C. glabrata has been reported, with the demise of the patient related to delayed diagnosis and lack of antifungal therapy for a prolonged period [7]. The present case is the first reported with fungemia, the presence of which lends credence to the true, invasive nature of the pathogen.
Although several risk factors for development of acute parotitis were present in this patient (e.g., elderly, post-operative, prolonged intubation), it did not develop until after prolonged (>48 h) non-invasive ventilation. Only four cases of acute parotitis have been reported after non-invasive ventilation [8–11], with time to onset ranging from eight hours to several days. The proposed mechanisms are mucosal dessication and partial obstruction of the Stensen duct from continuous positive airway pressure, causing salivary stasis and retrograde migration of bacteria into the gland.