
Abstract
Background:
Intestinal aspergillosis (IA) is a rare entity primarily discovered in immunocompromised patients. Because of its low incidence, IA is not considered routinely in the differential of abdominal pain, distension, and diarrhea. A systematic characterization of demographics, comorbidities, clinical presentations, and outcomes can help surgeons recognize and manage IA in critically ill patients.
Methods:
Two independent authors carried out the literature search using PubMed, MEDLINE, and Scopus databases. The Mesh terms utilized were: ‘intestinal’ and ‘aspergillosis’ combined with the Boolean operator ‘AND’ (synonyms were combined with the Boolean operator ‘OR’). Intestinal aspergillosis was defined as inflammation of the gastrointestinal tract (duodenum to rectum) caused by Aspergillus spp. All articles reporting IA were included. Articles describing aspergillosis of the esophagus or stomach were excluded. Statistical analysis was performed using SPSS software (version 18; SPSS Inc., Chicago, IL).
Results:
Forty-two articles reporting 56 cases were included in the study. Mean age was 44.9 ± 20.5 years. Male to female ratio was 29:27. The most common condition in patients who developed IA was transplantation (19 patients; 34%). The most common clinical presentations of IA were abdominal pain (21 patients; 38%) and diarrhea 12 patients; 21%). Sixty-six percent of patients had primary IA whereas 34% developed IA secondarily to systemic infection. Diagnostic modalities included exploratory laparotomy (35 patients; 63%) and endoscopy (7 patients; 13%). Mean time to diagnosis was 8.6 ± 11.3 days. Intestinal aspergillosis was limited to the small bowel in 61% of patients. In 43 (77%) patients, bowel resection is the definitive treatment, whereas 13 (23%) patients underwent antifungal therapy alone. Mortality rate was 39%. Sixty-three percent of patients treated with surgery survived, compared with 46% treated with antifungal therapy alone (p = 0.34).
Conclusion:
Intestinal aspergillosis is a life-threatening condition with a mortality rate of 39%. Extrapulmonary IA is seen in patients with neutropenia, sepsis, inflammatory conditions, and immunosuppression. Patients who undergo surgery are more likely to survive this infection.
Intestinal aspergillosis (IA) is a rare clinical manifestation of invasive aspergillosis that is primarily discovered in immunocompromised patients. Aspergillus spp. are spore (i.e., conidia) forming fungi that are usually found in the environment. In most cases, inhaled fungal conidia are cleared via the mucociliary escalator in the upper airway or by alveolar macrophages. The majority of human illness caused by this fungus belong to the Fumigatus, Niger, Flavus, and Clavatus species [1]. Notably, in immunosuppressed and neutropenic patients, Aspergillus fumigatus can evade the aforementioned host defense mechanisms to infiltrate the vasculature's endothelial cell lining to disseminate hematogenously to extrapulmonary sites [1]. The gastrointestinal (GI) tract is the second most commonly affected site after dissemination [1].
Comparably, the ingestion of Aspergillus conidia can present as IA in select patients with poor mucosal immunity and/or disruption to the GI mucosa [1]. Because of the low incidence of IA seen in the general population, intestinal aspergillosis is not considered routinely in the differential diagnosis of abdominal pain, distention, diarrhea, and lower GI bleeding.
The aim of this study was to review the literature on IA to characterize demographics, comorbidities, clinical presentations, and outcomes that can help surgeons recognize and treat IA in critically ill patients.
Materials and Methods
Search strategy and eligibility criteria
The literature search, data retrieval, and analysis, followed by critical appraisal, were performed by two independent researchers. Any disagreements occurring during the process were discussed and resolved. The PubMed, MEDLINE, and Scopus databases were searched systematically using the following Mesh terms: ‘intestines,’ ‘intestinal,’ and ‘aspergillosis’ combined with the Boolean operator ‘AND’ (all synonyms were combined with the Boolean operator ‘OR’). Inclusion criteria was all articles reporting IA. However, articles pertaining to aspergillosis of the esophagus and stomach were excluded to confine the study to IA. Relevant articles were identified and the search results were screened via the title, abstract, or full text article.
Definitions and data collection
Intestinal aspergillosis was defined as the inflammation of the GI tract from the duodenum to the rectum caused by Aspergillus spp. Data from selected publications were extracted into pre-defined tables. Collected data included demographics, comorbidities, patterns of clinical presentation, management modalities, and outcomes.
Statistical analysis
Statistical analysis was performed using SPSS Software (version 18; SPSS Inc., Chicago, IL). Continuous parameters were expressed as mean values with corresponding standard deviation whereas categorical parameters were represented by percentages and ratios.
Results
Forty-two publications reporting 56 cases were included in this review.
Demographics
The mean age of patients from the 56 reported cases was 44.9 ± 20.5 years with the male to female ratio being 29:27. Of note, the most common age distribution was 50–60 years, which comprised 17 cases (30%). In 86% of the cases, the patients' ethnicity was not reported. The most common pre-existing condition in patients who developed IA was transplant (19 patients; 34%), followed by acute myeloid leukemia (16 patients; 29%). Other predisposing conditions for the development of IA included: various hematologic malignancies (acute lymphoblastic leukemia, acute promyelocytic leukemia, and lymphoma), pancytopenia, appendicitis, ulcerative colitis, necrotizing enterocolitis (NEC), neuroectodermal tumor, and lung cancer.
Etiopathogenesis
The etiopathogenesis of IA proposed in previous publications is varied. For the development of IA, the fungus needs to either gain direct access to a compromised digestive tract or gain access to the human body, evade host immune defenses, and disseminate hematogenously to the GI tract.
As previously stated, airborne conidia have two common routes for entering the human body: inhalation or ingestion [1–3]. In addition to inhalation and ingestion, ostomies also act as potential entry sites [4]. Focusing on the inhalation pathway, conidia can colonize and become invasive if host immune defenses are impaired. For example, Safieddine et al. [5] and Shah et al. [6] state that impaired cilia lining the respiratory tract can lead to chronic fungal colonization. However, in patients with impaired phagocytosis by alveolar macrophages and neutrophilic granulocytes, IA occurs [5]. Notably, diabetes mellitus-induced hyperglycemia impairs phagocytosis and complement fixation, allowing for fungal colonization and possible dissemination [7]. Another mechanism that leads to Aspergillus colonization and eventual infiltration results from a hyperinflammatory state. Hyperinflammation is followed by a state of relative immune paralysis that deactivates monocytes and increases the risk for opportunistic infections such as disseminated aspergillosis [7,8]. Finally, the use of stress prophylaxis and proton pump inhibitors in select patients (e.g., burn) can result in an achlorhydric state that permits ingested conidia to invade the GI tract [9].
In physiologic states, an intact GI mucosa acts as a protective barrier to prevent pathogens from invading the GI tract. However, pathologic conditions that compromise the integrity of this barrier predispose individuals to GI aspergillosis. Most authors point to chemotherapy as the inciting event that disrupts the GI mucosal barrier. In particular, cytarabine has a direct cytotoxic effect on the GI mucosal barrier leading to mucositis. Mucositis can further lead to ulcerations, which provide a favorable environment for the colonization and invasion by Aspergillus spp. [1–3,6,10–14] Another mechanism that disrupts the mucosal barrier is NEC seen during the neonatal period [15]. The underdeveloped GI immune system combined with a chronic state of NEC results in an ideal setting for fungal infiltration of gastrointestinal mucosa [16–18].
In the presence of the above predisposing events, Aspergillus spp. can result in disseminated aspergillosis with GI involvement. This involvement can lead to numerous GI and systemic manifestations. Gastrointestinal manifestations can be categorized as parenchymal destruction, obstruction, or invasion. For example, Kinder and Jourdan [19] hypothesize that endotoxin release in the setting of GI aspergillosis causes tissue destruction as well as hemorrhage. The tissue and blood vessel destruction not only results in necrotic ulcers, but it also causes tissue ischemia that can lead to perforation [1,3,4,6,10,13,14,18,20–24]. One patient was found to have a colopleural fistula that was formed by a subdiaphragmatic abscess consisting of Aspergillus [25]. Additionally, GI aspergillosis can produce aspergillomas, fungal masses that can cause mechanical bowel obstruction or act as lead points in the pathogenesis of intussusception [6,26]. A unique sequalae of the bowel obstruction caused by GI aspergillosis is acute appendicitis [27,28]. After transmural invasion through the bowel wall, Aspergillus has a tendency to invade mesenteric vasculature [1,3,5,6,8–10,16,18,22,27,29–32]. With access to the blood vessels, the disseminated pathogen manifests as septic thromboembolism or intravascular thrombosis with associated intestinal ischemia [1,2,5,16,20,23,32,33]. Chronic necrotizing colitis and NEC (typhlitis) triggered by Aspergillus spp. were also suggested to lead to angioinvasion [3,9,16–18,30,33,34].
Clinical presentation
Figure 1 shows the patterns of clinical presentations of intestinal aspergillosis as seen in the 56 cases. Presenting symptoms included abdominal pain in 21 patients (38%), diarrhea in 12 cases (21%), GI bleed in 11 patients (20%), and abdominal distention in 11 patients (20%). Unfortunately, many cases of IA are missed because the abdominal symptoms of pain, distention, and diarrhea are overshadowed by systemic symptoms arising from the disseminated infection [29]. Some of these systemic symptoms include fever, fatigue, vomiting, as well as central nervous system, dermatologic, and pulmonary sequalae (e.g., altered mental status, dry cough, and sinusitis) [1,3,4,6,8–10,12,13,23,24,29,31,34–38]. The angioinvasive nature of Aspergillus spp. can result in intestinal ischemia, which presents clinically as GI bleeding in the form of hematochezia and bloody diarrhea [1,13]. Moreover, obstruction from IA can lead to acute appendicitis [28]. One patient presented with signs of peritonitis after bowel perforation [1,3,22–24,37,38]. In the absence of an acute abdomen, physical examination can be notable for pulmonary auscultatory findings of rhonchi and non-specific abdominal tenderness without guarding or rebound [1].
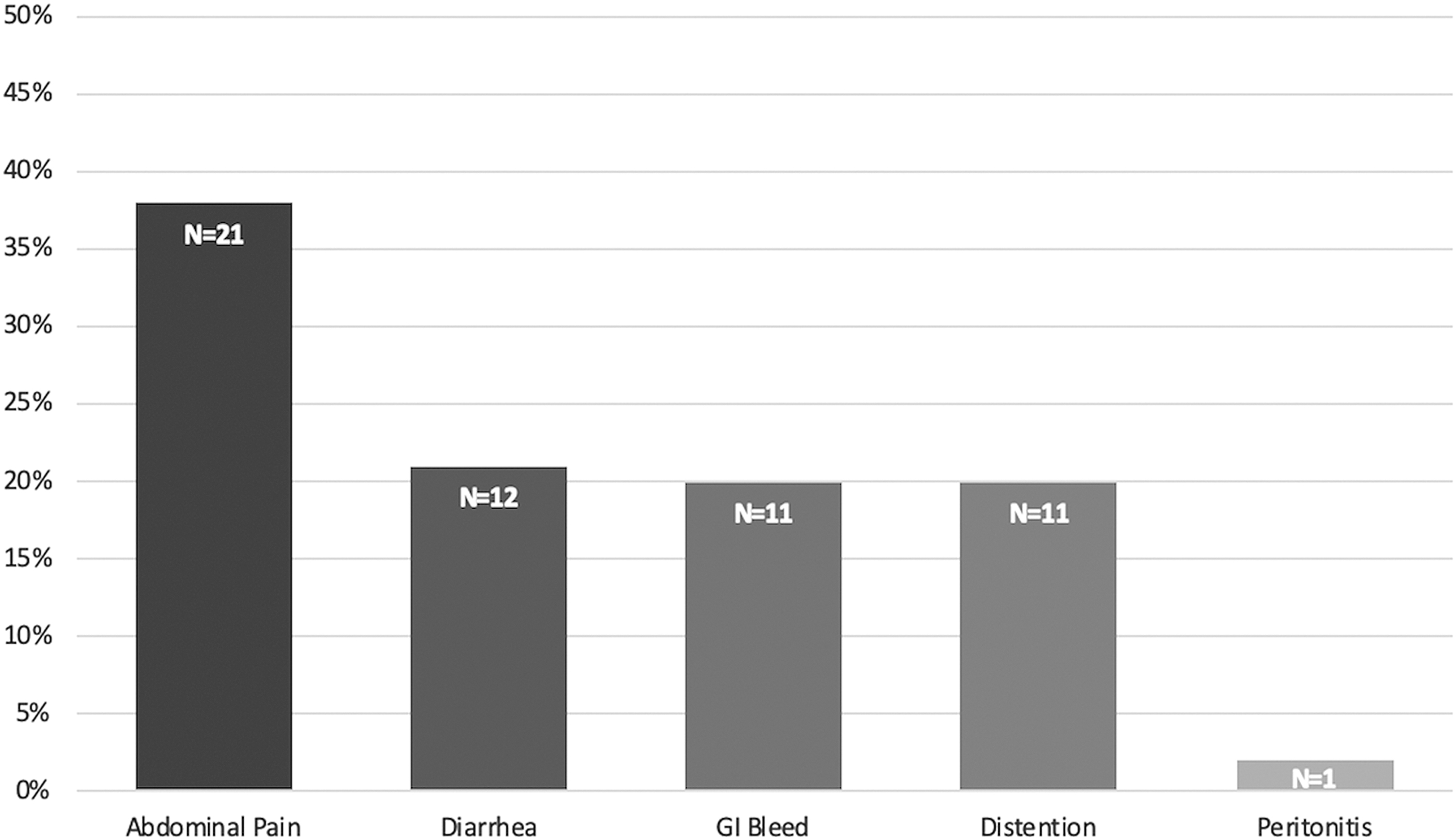
Patterns of clinical presentation of intestinal aspergillosis.
Diagnosis
Mean time to diagnosis was 8.6 ± 11.3 days. 37 (66%) patients had primary IA whereas 19 (34%) patients developed IA secondarily to a systemic infection. Diagnosis of IA has been historically made on post mortem autopsies. Figure 2 shows the range of diagnostic modalities used in cases previously reported. Given the non-specific clinical findings and negative blood cultures, a high level of clinical suspicion needs to be present to diagnose IA effectively in a timely manner [20]. Although there are no specific radiologic findings that are pathognomonic for IA, few authors began their workup using abdominal radiograms. Radiologic signs reported in the literature include gaseous distention of small bowel loops with air fluid levels, the stepladder sign, and pneumoperitoneum [6,7,18,24,26,29]. Although non-specific, multiple authors report using abdominal computed tomography (CT) as the imaging modality of choice for acute abdominal pain [1,4,6,8,13,17]. Abdominal CT findings of segmental wall thickening, semicircular perfusion defect of small-bowel, small bowel distention with a target or halo sign, inflammation of peripheral fat, and segmental mural thickening of the small intestine may support the diagnosis of IA [20]. Moreover, multiple authors utilized CT scans in acute abdomen to demonstrate a range of clinical findings from mechanical obstruction and pancolitis to multiple intestinal perforations with free peritoneal fluid and pneumoperitoneum [9,22,23,26,31,39]. As shown in Figure 3, 34 (61%) patients had IA confined to the small bowel, whereas IA was limited to the large intestine in 12 (21%) patients and to the ileocecal junction in seven (13%) patients.
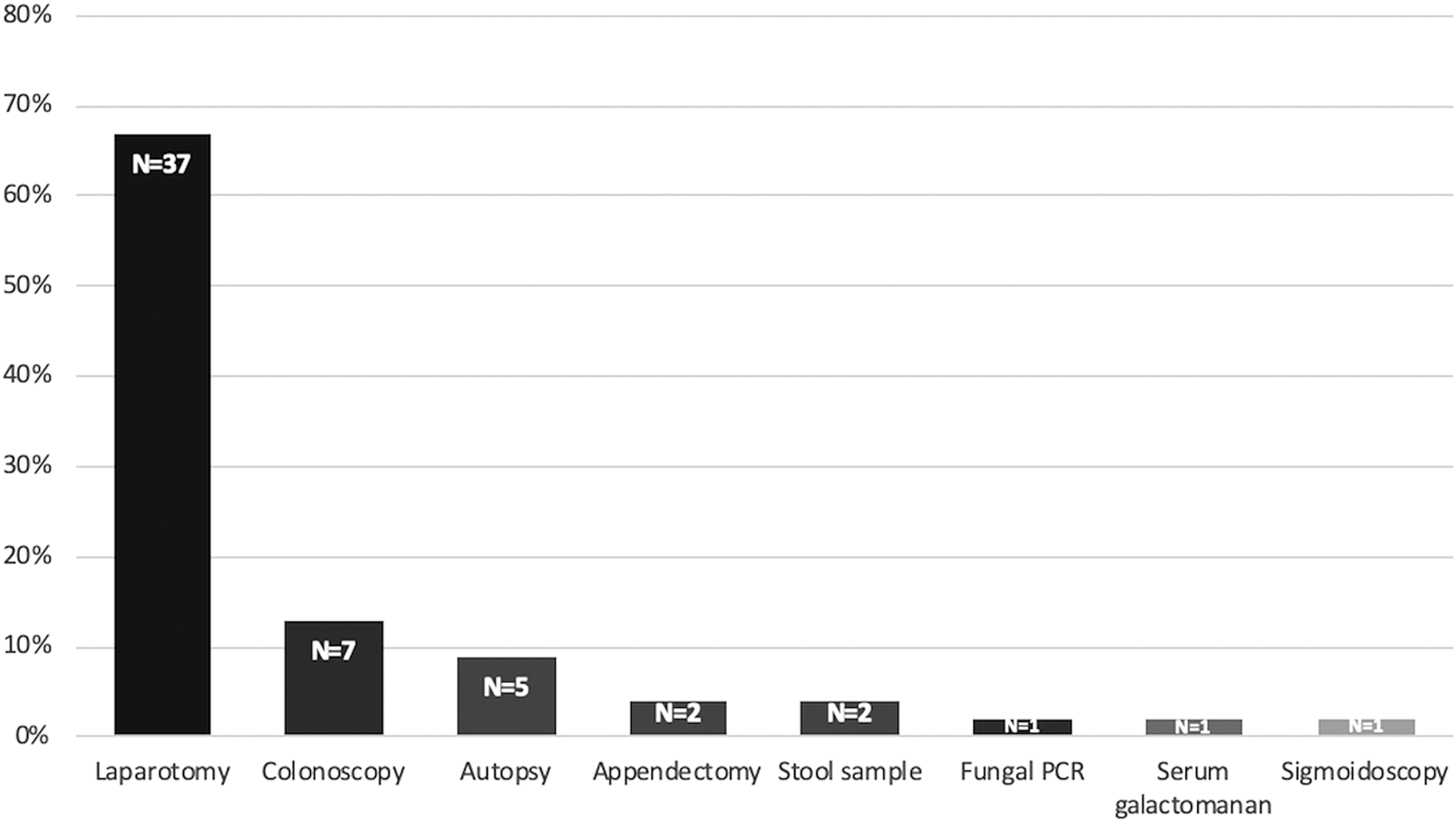
Modalities utilized for diagnosis of intestinal aspergillosis.

Intestinal sites of aspergillosis involvement.
The second most common mode of diagnosing IA was through colonoscopy in seven patients (13%). Through colonoscopy, biopsies of linear ulcers and areas of mucosal necrosis can be used as source tissue to perform histopathologic analyses [4,13]. Cultures in combination with histopathologic confirmation of mucosal invasion can provide evidence of IA. Histopathology has been used to show hemorrhagic infiltration, intravascular thrombosis, transmural necrosis, and other signs suggesting a diagnosis of IA [13,17,21,33]. However, microscopy with periodic acid-Schiff stain (PAS) or Grocott methenamine silver stain and culture are not sensitive [13]. Moreover, the potential for bleeding or perforation can complicate acquiring a biopsy specimen [13]. Kazan et al. [17] and others [8,12,17,26,35] report the utility of using the enzyme-linked immunosorbent assay (ELISA) galactomannan antigen test in combination with the clinical picture in order to support a diagnosis of IA. However, given the presence of galactomannan antigen in certain foods, Chambon-Pautas et al. [35] cautions the user of the substantial false-positive rate inherent in the ELISA test.
Reynolds et al. [40] recounted a patient who presented with IA masquerading as a Clostridium difficile infection [40]. Thus, an alternative diagnosis should be sought in patients who fail to respond to treatment. Two authors reported being able to diagnose IA by checking for the presence of fungal hyphae under direct microscopic stool examination [30,36]. More recently, Reynolds et al. [40] utilized polymerase chain reaction (PCR) to detect Aspergillus to diagnose IA. Unfortunately, the most common means of definitively diagnosing IA was through exploratory laparotomy in 63% of patients. Common laparotomy findings reported in the literature include thickened bowel wall, mucosal ulceration, full thickness necrosis, ascites, coloenteric fistula, obstruction, or perforation [20,22,24,38,41,42]. Given the inherent limitations of the indirect diagnostic methods (e.g. PCR), we believe the gold standard for IA diagnosis is either histopathological evidence showing hyphal infiltration of the intestinal wall, arteritis, and/or thrombus formation within intramural vessels; or tissue culture, taken from disease site, demonstrating Aspergillus spp. growth.
Treatment
Non-operative management using antifungal therapy alone was reported in 13 cases (23%) whereas all remaining 43 patients (77%) underwent some form of operative management. Operative treatment comprised either primary resection, resection with anastomosis, or total colectomy with ileostomy. Antifungal therapy was limited to prompt initiation with either intravenous voriconazole or intravenous amphotericin B. The efficacy of 5-fluororcytosine is still under investigation [6,37]. Twelve patients (21%) underwent only bowel resection whereas in 31 patients (55%) bowel resection was supplemented by antifungal therapy. The evaluation and treatment of IA patients is summarized in Figure 4.

Diagnosis and management algorithm for intestinal aspergillosis. *Risk factors include patients with hematologic malignancy, organ transplantation, ulcerative colitis, necrotizing enterocolitis (NEC), neuroectodermal tumor, and lung cancer. **Clinical symptoms include abdominal pain, diarrhea, gastrointestinal bleed, abdominal distention, pulmonary sequalae, and systemic involvement (e.g., fever, fatigue, etc.). ***Gross findings include thickened bowel wall, mucosal ulceration, full thickness necrosis, ascites, coloenteric fistula, obstruction, or perforation.
Outcomes
Overall mortality rate of IA was 39%. Figure 5 shows that in patients undergoing antifungal therapy alone, 54% did not survive. Post-therapy mortality was much lower at 37% for the cohort of patients who underwent surgery and received antifungal medication. The success rate of surgery in combination with antifungal therapy was 63% compared with the 46% survival rate with antifungal therapy alone (p = 0.34).
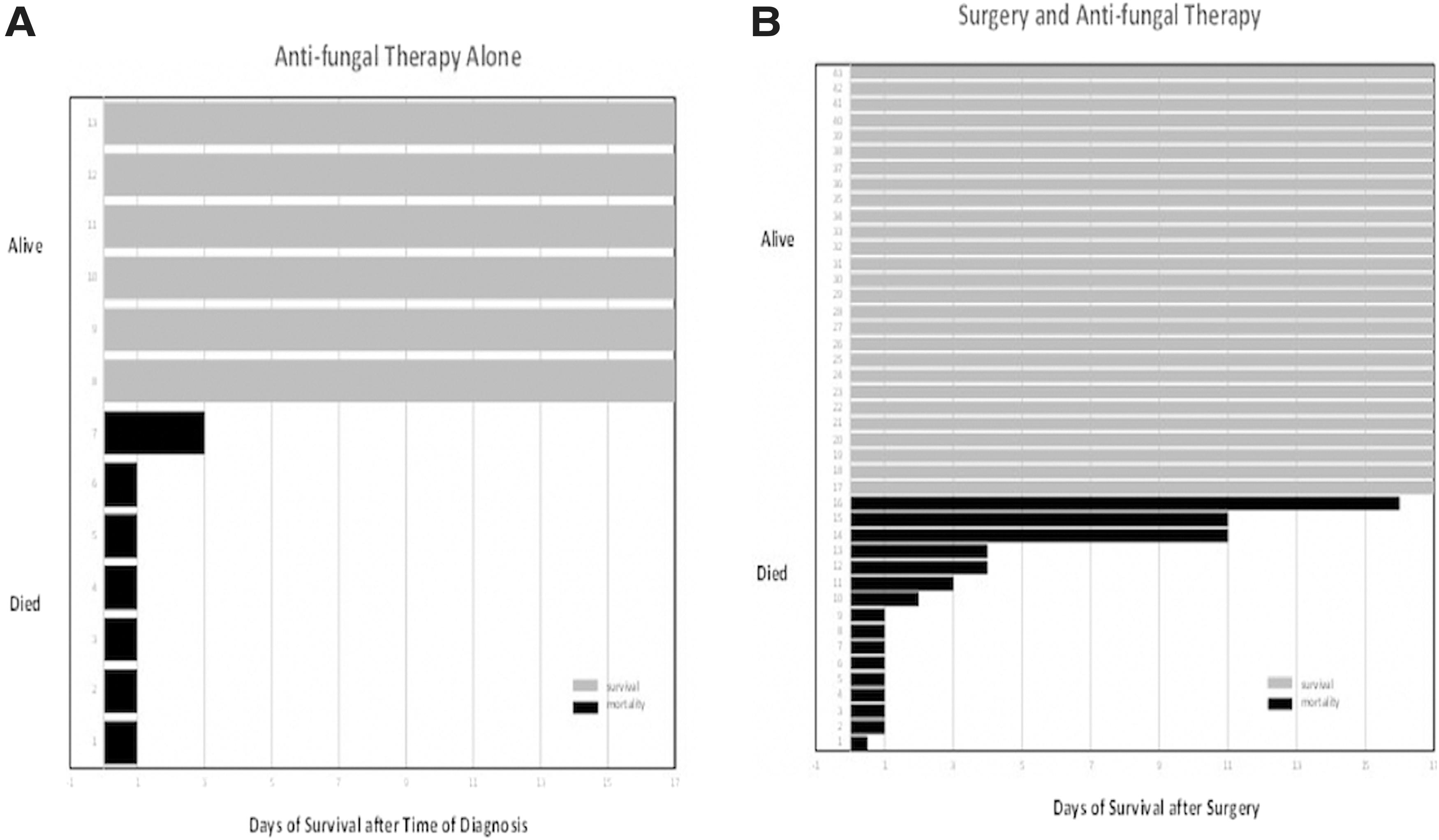
Histogram depicting the outcome (survival versus mortality) of patients treated with (
Discussion
Invasive aspergillosis arises most commonly from a primary pulmonary infection that secondarily disseminates hematogenously to distant sites such as the skin, paranasal sinuses, central nervous system, and GI tract. The gastrointestinal tract is the second most common site of invasive aspergillosis with the small intestine being the organ most commonly involved [1]. Although more rare, isolated GI aspergillosis without pulmonary involvement has been described in a few patients. The ingestion of Aspergillus conidia combined with a loss of mucosal barrier integrity can result IA. Predisposing factors that result in IA include a state of immunosuppression commonly seen in transplant, neutropenic, pancytopenic, burn, critically ill, and hematologic cancer patients [3,9,17,29,30]. In particular, of all the hematologic malignancies reviewed in this study, patients with acute myeloid leukemia (AML) were diagnosed with IA more frequently than patients with other hematologic and non-hematologic malignancies. Moreover, the use of steroids, cytotoxic chemotherapeutic agents, anti-tumor necrosis factor (TNF) medications, and broad-spectrum antibiotic agents have also been associated with IA [7,9,19,22]. Characteristic manifestations of GI aspergillosis include angioinvasion of mesenteric arteries that can result in intravascular thrombosis, septic thromboembolism, and subsequent tissue ischemia. Consequently, ischemia leads to tissue infarction, resulting in necrotic tissue and eventual bowel perforation [1,4,14,20].
Intestinal aspergillosis clinically presents as a mixture of systemic symptoms combined with non-specific abdominal findings. The most common symptom identified in this study was abdominal pain in 38% of the selected cases. Although abdominal pain is the most reported symptom, the location is non-specific. For example, Decembrino et al. [11] and Enjoji et al. [20] present patients who report lower right quadrant pain whereas the other patients presented in the selected case reports endorse diffuse pain. Remarkably, the abdominal symptoms are eclipsed by varying systemic symptoms that arise due to the disseminated infection affecting other organ systems. Consequently, in immunosuppressed or neutropenic patients presenting with constitutional findings and abdominal symptoms such as pain, distention, diarrhea, or gastrointestinal bleeding, there should be a high clinical suspicion for IA [6,23,38]. A high level of suspicion should also be exercised in patients with fever of unknown origin or those with persisting pyrexia despite clear lungs and sinuses [26,41]. This high index of suspicion should in turn be combined with early endoscopic biopsy and aggressive empirical antifungal therapy [12,14,26,30,32].
Given the grim fate of those affected by IA, preventative methods play an important role in reducing morbidity and mortality. Hayden et al. [12] suggest routinely requesting microbiologic investigation of surgical resection specimens in immunocompromised patients, even when an infective cause is not considered to be the most likely diagnosis.
Histopathologic analysis after endoscopic biopsy has been championed as a way of diagnosing IA [13]. Surprisingly, a review of the case reports included in this study found that exploratory laparotomy was required in 63% of patients to make a definitive diagnosis. One possible explanation for this discrepancy can be because of the rapidly deteriorating clinical condition of patients with IA. Not only does the clinical deterioration pose innumerable risks with acquiring biopsies for histopathology analysis but it also presents with complications (e.g., perforation) and clinical signs (e.g., peritonitis) that are managed via exploratory laparotomy. In addition to exploratory laparotomy, the use of ELISA, stool microscopy, and PCR tests, in tandem with the clinical picture, have shown diagnostic promise.
Treatment options outlined in the literature include non-operative, operative, or a combined approach. The combined approach of bowel resection and antifungal medication was the most common treatment modality as it was used in 31 (55%) patients. Bowel resection ranged from small bowel resection with anastomosis to partial or total colectomy with an ileostomy [2,9,30,34]. The survival rate following combination therapy (surgical resection and antifungal therapy) was higher than that of antifungal therapy alone. However, this finding is confounded by the possibility that patients offered antifungal therapy only were too ill to undergo surgery and therefore had a lower chance of survival at baseline.
Conclusion
Intestinal aspergillosis is a life-threatening condition with a mortality rate of 39%. This clinical entity is encountered mostly in patients with neutropenia, immunosuppression, and hematologic malignancies. These patients present with constitutional symptoms as well as extrapulmonary symptoms including abdominal pain, abdominal distention, diarrhea, and/or hematochezia. The majority of these patients require antifungal therapy accompanied by prompt surgical management with bowel resection in order to maximize survival rates.
Footnotes
Acknowledgment
This article does not contain any studies with human participants or animals performed by any of the authors. Informed consent was not obtained.
The abstract was presented at the 2018 American Society of Colon and Rectal Surgeons (ASCRS) Annual Meeting and the New York Society of Colon and Rectal Surgeons (NYSCRS) Meeting.
Author Disclosure Statement
The authors declare that they have no conflict of interest.