
Abstract
Background:
The impact of negative pressure wound therapy (NPWT) as an adjunct to colorectal surgery is largely unknown. The purpose of this study was to determine whether NPWT impacts wound complications during elective open colectomy.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) and colectomy targeted procedure databases were queried from 2012–2018 for patients undergoing non-emergent planned open colectomies. Groups were propensity score matched for anastomosis type (ileo-colic, colo-colic, colo-rectal), age, body mass index (BMI), diabetes, smoking, steroid use, wound classification, American Society of Anesthesiologists (ASA) class, operative time, and wound layers closed. Wound complications were defined as superficial surgical site infection (SSI), deep incisional SSI, and dehiscence.
Results:
A total of 15,770 patients were identified; 92 underwent simultaneous NPWT (0.58%). Non-NPWT patients were matched at a 5:1 ratio, producing 460 comparisons. There was no difference in wound complications (8.26% non-NPWT vs. 6.52% NPWT; p = 0.574). In addition, there were no differences in wound complications when only including patients who had NPWT placed over closed skin (9.11% non-NPWT vs. 7.25% NPWT; p = 0.789). On multivariable analysis, NPWT was not associated with wound complications (odds ratio [OR] 0.79; 95% confidence interval [CI], 0.37–1.69).
Conclusions:
Negative pressure wound therapy does not reduce wound complications in open elective colectomies. Large randomized studies and more granular data are needed to ascertain if there is any benefit in select patient populations.
In open colorectal surgery, surgical site infection remains one of the most common and problematic complications [1–3]. Surgical site infections (SSI) are associated with morbidity, as well as psychological burden and increased economic burden to the healthcare system. Surgical site infection rates remain high in colorectal surgery despite targeted implementations including prophylactic antibiotic agents, aseptic technique, and use of two tables (a clean and a dirty table) [4]. The rate of SSI in open colorectal surgery historically ranges from 15% to more than 30% [1,2]. Inclusion of negative pressure wound therapy (NPWT) in SSI bundles has been advocated by some, and most often, its use has been reserved for complex open wounds in both acute and chronic care situations [5,6]. The device consists of an open-pore foam that is placed in the wound, covered by a semi-occlusive dressing, and connected by a tube to a vacuum source [7]. The exact mechanism by which NPWT reduces the incidence of infections is unknown. However, it is theorized that NPWT functions by promoting angiogenesis, reducing edema, providing a sterile physical barrier, and preventing sheer forces.
Currently there is no standard of care method recommended by any society for the method of wound closure after open colorectal surgery. Given the paucity and conflicting literature regarding the role of NPWT as an adjunct to wound closure in open colorectal surgery, the purpose of this study is to determine whether NPWT impacts wound complications during elective open colectomy.
Patients and Methods
Inclusion and exclusion of patients
Participant Use Data File (PUF) and Procedure Targeted PUF data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database were extracted encompassing cases from the years 2012 to 2018. Inclusion criteria were patients 18 and older who underwent open partial colectomy with anastomosis (CPT 44140), open partial colectomy with coloproctostomy (CPT 44145), or open partial ileocecectomy (CPT 44160). Patients were excluded if the primary surgeon was not a general surgeon and if the surgery was non-elective (emergent) (Fig. 1). Of note, the ACS-NSQIP database does not differentiate between general surgeons and colorectal surgeons. Other exclusion criteria included if the patients had pre-operative ventilator support, pre-operative septic shock, pre-operative wound infection, pre-operative distant cancer, American Society of Anesthesiologists (ASA) class 5, or if the fascia was not closed at the time of surgery. Patients were then divided into two patient groups, those who underwent a simultaneous NPWT procedure (CPT 97605, 97606, 97607, 97608) and those who did not (non-NPWT patients). Because the data are publicly available, Institutional Review Board approval was not required.
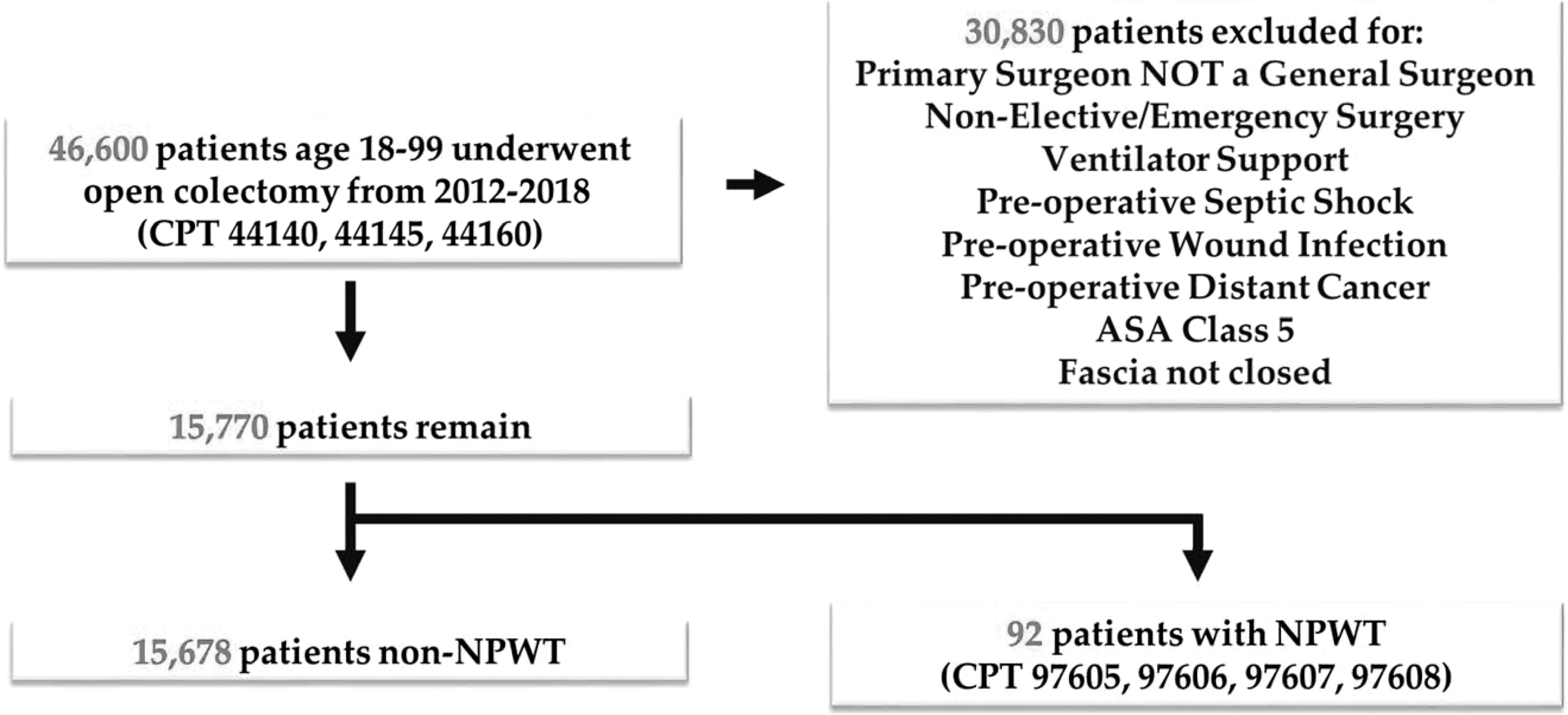
Inclusion and exclusion criteria flowchart. NPWT = negative pressure wound therapy; ASA = American Society of Anesthesiologists.
Propensity score matching
Propensity score matching was performed using R, an open source statistical software package. The two groups were matched based on age, gender, smoking, obesity (body mass index [BMI] >30), diabetes, hypertension, ASA class, wound classification, type of colectomy (as defined by Current Procedural Terminology [CPT] code), use of pre-operative steroids, oral antibiotic bowel preparation, operative time, and wound closure. Non-NPWT patients were matched at a 5:1 ratio to NPWT patients. This ratio was selected to maximize efficiency and minimize sampling variance; relative gains in efficiency are minor when matching ratios exceed 5:1 [8]. Matching was conducting using the “matchit” package and the “nearest neighbor” technique as described by Randolph et al. [9].
Statistical analysis
For qualitative parameters, a univariable analysis was performed using either a χ2 with more than 10 occurrences or a Fisher exact test for 10 or fewer occurrences. A two-tailed Student t-test was utilized for continuous parameters. Univariable analysis was performed before and after propensity score matching. Outcomes analysis was only performed on propensity score matched patients. Minor and major morbidities were defined according to the Clavien–Dindo classification [10]. All p values were two-sided and p < 0.05 was considered statistically significant. Data were extracted and analyzed using both Microsoft Excel (Microsoft Corporation, Redmond, WA) and R, open source software.
Results
A total of 15,770 elective open colectomy patients met inclusion criteria. The patients were separated into 15,678 patients without the use of NPWT and 92 patients with the use of NPWT (Table 1). Elective open colectomies and NPWT were associated with younger patients (62.6 non-NPWT vs. 58.7 NPWT; p < 0.011), obesity or BMI >30 (34.69% non-NPWT vs. 46.74% NPWT; p < 0.15), smoking (18.15% non-NPWT vs. 27.17% NPWT; p < 0.025), pre-operative dialysis (0.67% non-NPWT vs. 3.26% NPWT; p < 0.025), and the use of oral antibiotic preparation (45.04% non-NPWT vs. 60.87% NPWT; p < 0.002).
Univariate Analysis of Pre-Operative Factors for Use of NPWT with Elective Colectomies
Bold values indicate significant p values.
NPWT = negative pressure wound therapy; SD = standard deviation; BMI = body mass index; COPD = chronic obstructive pulmonary disease; CHF = congestive heart failure; HTN = hypertension.
After undergoing propensity score matching in a 5:1 ratio (Fig. 2), the two groups underwent univariable (Tables 2 and 3) and multivariable analysis (Table 4). Univariable analysis on the propensity score matched revealed no statistically significant difference with the use of NPWT for pre-operative, intra-operative, and post-operative factors (Tables 2 and 3, respectively).
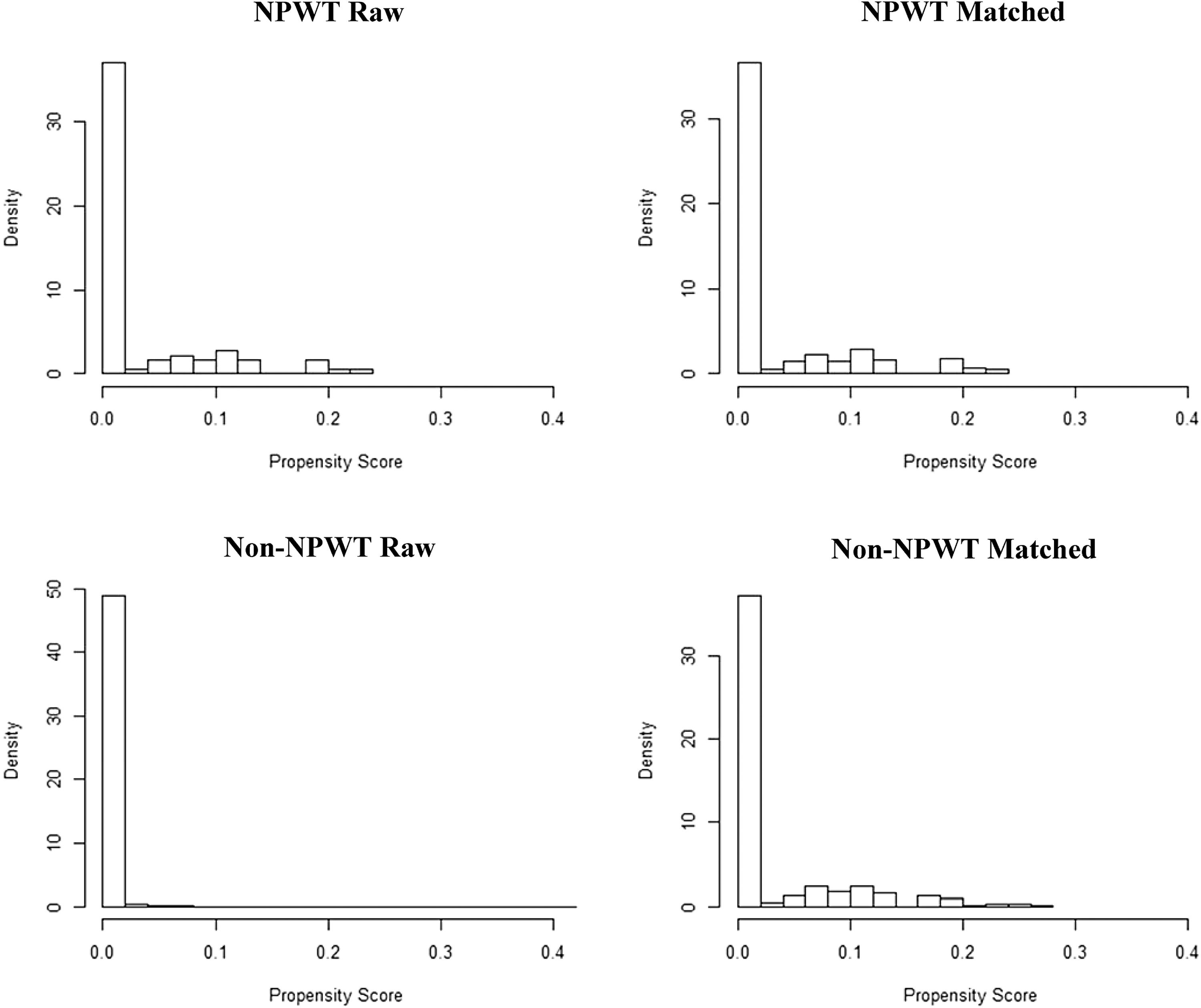
Propensity score matching histogram. NPWT = negative pressure wound therapy.
Propensity Score Matched Univariable Analysis of Pre-Operative and Intra-Operative Factors for Use of NPWT with Elective Open Partial Colectomies
Bold values indicate significant p values.
NPWT = negative pressure wound therapy; SD = standard deviation; BMI = body mass index; COPD = chronic obstructive pulmonary disease; CHF = congestive heart failure; HTN = hypertension; ASA = American Society of Anesthesiologists.
Propensity Score Matched Univariable Analysis of Post-Operative Factors for Use of NPWT with Elective Open Partial Colectomies
Bold values indicate significant p values.
NPWT = negative pressure wound therapy; SSI = surgical site infection; SD = standard deviation; OR = operating room.
Minor and major complications defined by Clavien-Dindo classification.
Propensity Score Matched Multivariable Regression of Pre-Operative and Intra-Operative Factors for Wound Complications During Elective Open Partial Colectomies
Bold values indicate significant p values.
CI = confidence interval; NPWT = negative pressure wound therapy; BMI = body mass index; ASA = American Society of Anesthesiologists.
On multivariable analysis, longer operative times were associated with the primary outcome of wound complications (superficial SSI, deep SSI, or wound dehiscence) (odds ratio [OR] 1.149; 95% confidence interval [CI], 1.03–1.28). Last, the specific use of NPWT was not associated with wound complications (OR 0.794; 95% CI, 0.37–1.69; Table 4).
Discussion
The current literature reveals conflicting data on the use of NPWT in open colorectal procedures. In 2013, Bonds et al. [11] performed a single-center retrospective study and found incisional NPWT reduced SSI in open colorectal surgery (OR 0.32; 95% CI, 0.1–0.9). Most recently, the NEPTUNE randomized controlled trial by Murphy et al. [4] compared the occurrence of SSI with NPWT versus standard gauze dressing after open colorectal surgery. In this trial, NWPT was not associated with a decrease in SSI compared with standard gauze dressing. Additionally, Webb et al. [12] reported an increase in SSI utilizing NPWT in patients undergoing open colorectal surgery, especially with concomitant ostomy formation.
Even with only 92 NPWT patients, this study is the largest in the literature examining the use of NPWT and its impact on wound complications with regard to elective open partial colectomies [4]. On our analysis, the association between the use of NPWT and wound complications was not statistically significant. These findings help clarify the possible unnecessary role of NPWT in elective open colectomy by mirroring evidence previously reported in the literature.
The majority of studies currently in the literature evaluate incisional NPWT in elective open colorectal surgery. Whereas traditional NPWT applies negative pressure to the wound bed itself via an open incision or wound, incisional NPWT therapy applies negative pressure around and over the site of a closed incision. Incisional NPWT, in particular, has been proposed to decrease SSI by sealing the wound and preventing contamination from repeated dressing changes [13]. Because of the limitations of NSQIP and CPT coding, the specific use of incisional NPWT is not an option. Therefore, in our study we queried for the use of NPWT in general via CPT coding.
When we included only patients who had NPWT placed over closed skin (subgroup analysis of the previously matched data), there was no difference in wound complications (31 or 9.11% of 340 total non-NPWT vs. 5 patients or 7.25% of 69 total NPWT, p = 0.789). The majority of NPWT placed in elective open colectomies are performed in the setting of closed wounds. Through the use of the NSQIP database, we are unable to determine the etiology as to why the skin was left open during some elective procedures. More than likely, the operating surgeon made a clinical decision to not close the skin due to a combination of classic pre-operative or intra-operative factors concerning for increased risk of wound complications such as increased pre-operative comorbidities, smokers, obesity, fecal spillage or contamination, etc.
Two main factors may explain our discrepancy of wound complication rate versus reported SSI complication rates as stated in the background [1,2]. First, wound complications (superficial SSI, deep SSI, and wound dehiscence) rather than SSI was chosen as our primary outcome because the use of NPWT should not affect organ space infections whereas the rate of wound dehiscence may be altered. Second, the patient population selected for this study is biased toward relatively healthy, non-emergent, and hemodynamically stable patients. Therefore, one would expect lower rates of both wound complications and SSI in this selected population.
Although there are many strengths and limitations of post hoc analyses, there remains merit to these statistical tools when used appropriately because they can provide “valuable insights and associations that were not anticipated by assumptions made a priori” [14]. This current study is underpowered, therefore it may not be able to detect a substantial difference between NWPT and traditional wound care when one actually exists. However, if the absolute difference in wound complications were significant (8.26% non-NPWT vs. 6.52% NPWT; p = 0.574), the absolute risk reduction was only 1.74%, resulting in a number needed to treat (NNT) being approximately 57 patients to prevent one wound complication. Using the approximated cost of an incisional NPWT system of $495, the cost of preventing one wound complication (NNT × incisional NPWT system cost) is approximately $28,448 [15]. Gantz et al. [16] reported the cost of treatment for an SSI after elective colorectal surgery on average is $18,410, which raises the question of whether incisional NPWT is a cost-effective method for preventing wound complications or SSIs after elective colorectal surgery.
In addition, the use of NPWT was incredibly low, approximately 0.6% of cases meeting inclusion criteria. This may have occurred for a number of reasons. Operative notes may be dictated by residents and can be inaccurate with missed CPT codes and associated under-reimbursement [17]. Furthermore, the NPWT may be placed in the operating room by a wound care team as opposed to the surgeon, which may not be reflected in surgical billing or documentation [18]. Additionally, it is probable that many surgeons are unaware that intra-operative NPWT placement is a billable event.
Limitations of this study include its retrospective nature and the susceptibility to clerical errors within large databases such as NSQIP [19]. Variations in protocols used for peri-operative care per physician and institution, specifically post-operative wound assessment, could have impacted the rate of SSI, as well as the use of NPWT therapy. Another limitation includes the presence of other procedures listed under concurrent or other CPT when selecting patients whose primary CPT was 44140, 44145, or 44160. We mitigated this by the use of propensity score matching specifically addressing type of colectomy (primary CPT), operative time, and other pre-operative factors that may influence our patient cohorts.
Although the ACS-NSQIP database contains numerous variables for data analytic purposes, there are variables that this study may not be accounting for (i.e., the use of a wound protector or peri-operative systemic antibiotic agents) and should be considered a possible limitation as well to this study. Last, there was no standardized use or methodology for implementation of NPWT.
Future considerations and studies should attempt to determine if NPWT impacts SSI and wound complication rates in patients who are high risk, i.e., contaminated and dirty wound classification, emergent surgery, septic shock, etc. Whereas this study demonstrates that the use of NPWT may not benefit the elective partial colectomy population, perhaps its use may show benefit to a high surgical risk demographic. Further understanding of the impact of NPWT on SSI in open colorectal surgery should be gained from a randomized controlled study that is currently underway [20].
Conclusion
Negative pressure wound therapy does not reduce wound complications in elective open colectomy substantially. Given that NPWT is unproven in the literature and that there is an unclear cost benefit, we caution against its use in elective open colectomy. Large randomized trials are necessary to investigate NPWT use during elective open colectomy further and are currently underway.
Footnotes
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. No competing financial interests exist.
Funding Information
No funding was required or received for this study, therefore, the authors have no financial disclaimers.
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.