
Abstract
Background:
Methicillin-resistant Staphylococcus aureus (MRSA) is a major cause of skin and soft tissue infections and their recurrences. Although traditionally not considered for use against MRSA, cefazolin presents a possible option when administered using ultrasonic drug dispersion (UD2). This novel technique localizes delivery of drug into the subcutaneous tissue and achieves concentrations that exceed the minimum inhibitory concentrations (MICs) of most clinical MRSA isolates. The purpose of this study was to evaluate the impact of achievable cefazolin concentrations on the rate and extent of bactericidal activity using time-kill methodologies
Materials and Methods:
The cefazolin MICs of the four MRSA isolates selected for this in vitro time-kill study were 64, 128, 256, and 512 mg/L. Duplicates of drug-free control and cefazolin experiments were carried out using the average UD2-achievable cefazolin concentration (1,300 mg/L). Experiments were incubated at 37°C throughout each run. Samples were plated and incubated for 18 to 24 hours. The lower limit of detection of colony forming units per milliliter (CFU/mL) was 1.7 log10 CFU/mL. Cefazolin was considered bactericidal when it decreased bacterial density by ≥3 log10 CFU/mL from the initial inoculum after 24 hours of incubation.
Results:
Cefazolin produced mean 24-hour CFU changes of −4.39 to −4.89 log10 CFU/mL against MRSA isolates with MICs from 64 to 512 mg/L. Cefazolin demonstrated bactericidal activity against all studied MRSA isolates and no regrowth was observed at 24 hours.
Conclusions:
The mean cefazolin tissue concentration achieved by UD2 was bactericidal against four MRSA isolates. Further investigation is warranted to assess the utility of UD2-administered cefazolin against MRSA skin and soft tissue infections.
Methicillin-resistant Staphylococcus aureus (MRSA) continues to be a major pathogen of concern in skin and soft tissue infections (SSTI). Originally associated with causing hospital-acquired infections in the 1960s, MRSA is now also frequently responsible for community infections, possibly as much as 60% of emergency department SSTIs [1,2]. Recurrent infections are also a common occurrence with rates of over 50% in certain populations [3]. Traditionally deemed intrinsically ineffective against MRSA, β-lactams are passed over in favor of vancomycin, linezolid, daptomycin, tigecycline, and other newer agents [4].
By its nature, cefazolin, a first-generation cephalosporin, is not customarily considered to treat MRSA infections because required concentrations far exceed those achieved through conventional systemic administration [5]. However, a novel drug technique, ultrasonic drug dispersion (UD2), has the potential to address these concerns. During UD2, the drug is injected subcutaneously into the infected area before being dispersed with ultrasound (3 W/cm2) applied across the skin for three minutes [6]. This method previously has shown favorable results for cefazolin in a study for treatment-resistant patients, wherein 98% of the 96 patients were successfully treated [6]. These promising results support the use of cefazolin administered in this specialized manner against MRSA.
To gauge the viability of this approach, our laboratory conducted a surveillance study of 1,239 clinical MRSA isolates from hospitals in the United States and observed that, with the exception of one strain, all isolates had cefazolin minimum inhibitory concentrations (MICs) ≤512 mg/L [5]. This was encouraging, considering that a UD2 study performed on patients undergoing elective abdominoplasty observed a higher average cefazolin tissue concentration of approximately 1,300 mg/L [6]. Therefore, the objective of this study was to assess the in vitro antibacterial efficacy of the tissue-achievable cefazolin concentration against clinical MRSA isolates with a wide range of MICs.
Materials and Methods
Four MRSA isolates selected from the abovementioned surveillance study were included. Based on the surveillance study, which observed an MIC50 of 64 mg/L and MIC99.9 of 512 mg/L [5], isolates spanning 64 to 512 mg/L were chosen for this study (Table 1).
Minimum Inhibitory Concentrations against the Four MRSA Study Isolates
MRSA = methicillin-resistant Staphylococcus aureus; MIC = minimum inhibitory concentrations.
Duplicate antibiotic-free control experiments and cefazolin experiments were conducted on each of the selected MRSA isolates using the average cefazolin concentration observed when utilizing the UD2 technique (1,300 mg/L) [6]. Commercially available cefazolin vials (lot 9C0216A18; Apotex Inc., Toronto, Ontario, Canada) were obtained through Cardinal Health (Dublin, OH) and stored at room temperature until use. The vials were reconstituted according to manufacturer specifications and the appropriate volumes were added to the time-kill vessels to reach the target cefazolin concentration.
Experiments were carried out using Mueller-Hinton broth (Becton, Dickinson and Company; Sparks, MD) inoculated with a bacterial suspension to resulting in approximately 106 colony forming units per milliliter (CFU/mL). Two formats of these experiments were performed: an eight-hour format and a 24-hour format. The eight-hour experiments were conducted in capped glass test tubes with final bacterium-drug volumes of 10 mL and incubated in a shaking water bath (37°C). Samples were obtained at 0, 0.25, 0.5, 1, 2, 4, and 8 hours. The 24-hour experiments were conducted in drained PVC Viaflex infusion bags (lot Y292854; Baxter Healthcare, Inc., Deerfield, IL) with final bacterium-drug volumes of 200 mL and incubated at 37°C. Samples were obtained at 0, 0.5, 1, 2, 4, 8, 12, and 24 hours. To assess mean bacterial densities, samples were diluted, plated on blood agar plates, and incubated for 18 to 24 hours. The lower limit of detection of CFU/mL was 1.7 log10 CFU/mL. For the 24-hour experiments, cefazolin was categorized as bactericidal when it demonstrated a reduction of ≥3 log10 CFU/mL from the initial inoculum after 24 hours of incubation.
Results
Time-kill curves for cefazolin in the eight-hour and 24-hour experiments are depicted in Figure 1. The mean bacterial density at 0 hours was 6.59 ± 0.17 log10 CFU/mL across the four studied isolates. Antibiotic-free control experiments grew by 2.17 ± 0.15 log10 CFU/mL over the 24-hour study period. Cefazolin produced 24-hour CFU changes of −4.70 ± 0.27, −4.89 ± 0.00, −4.39 ± 0.71, and −4.79 ± 0.14 log10 CFU/mL for STA 142, STA 145, STA 147, and STA 150, respectively. Overall, the rate and extent of cefazolin kill was similar over the MIC range 64 to 512 mg/L. Cefazolin achieved bactericidal activity against all studied MRSA strains. No re-growth was observed at 24 hours among any of the isolates.
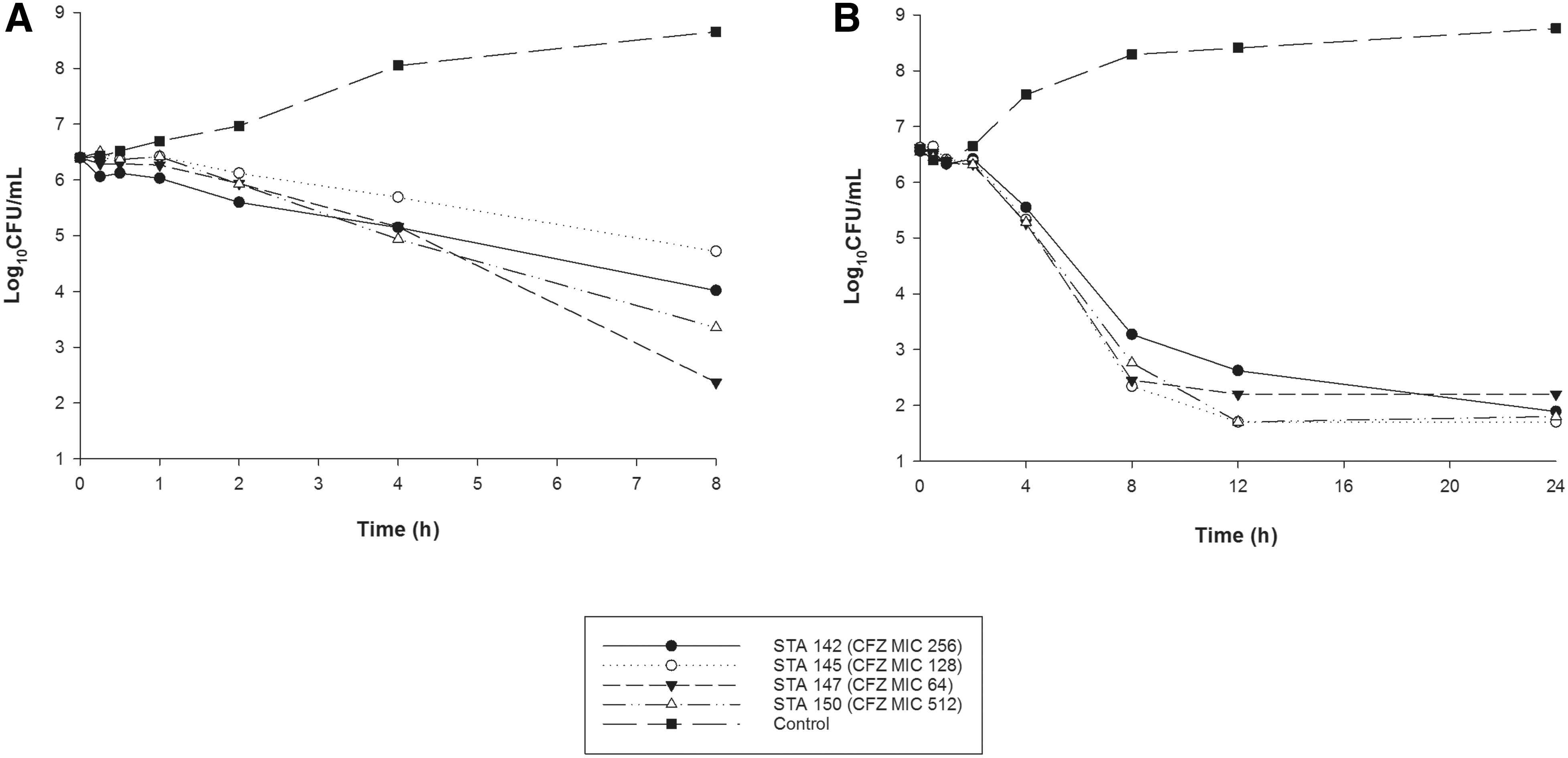
Time-kill experiments depicting the activity of cefazolin (CFZ) against methicillin-resistant Staphylococcus aureus (MRSA) isolates with CFZ minimum inhibitory concentrations (MICs) of 64, 128, 256, and 512 mg/L during (
Discussion
Methicillin-resistant Staphylococcus aureus has been challenging healthcare providers for more than half a century. In particular, higher mortality and longer length of stay have been associated with MRSA SSTIs compared with cases caused by other pathogens [7,8]. Whereas the development of new antimicrobial agents has generated alternative options to the standard of vancomycin, the long timelines associated with drug development emphasize the importance of using agents that have already been approved and have historical safety data to further guide decision-making. Strategies include maximizing dosing regimens, prolonging infusions, and using alternate routes of administration, such as UD2. More specifically, UD2 aims to tackle pharmacokinetic issues through a combination of local delivery and active dispersion. Thus, patients with infections at poorly vascularized sites, which antibiotics may otherwise fail to penetrate sufficiently, have a potential treatment option.
The previously conducted surveillance study demonstrated that most clinical MRSA isolates had MICs below the average tissue concentration of UD2-delivered cefazolin [5,6] and the bactericidal activity demonstrated in our study is promising. Given the frequency of recurrent MRSA SSTIs and resistance development, the lack of re-growth is especially encouraging. These in vitro time-kill experiments using isolates with a wide range of MICs further support the utility of what is customarily considered an ineffective antibacterial agent for MRSA.
A limitation of this study is that the time-kill methodology only allows for a single concentration to be tested, as opposed to a pharmacodynamics model that could more closely replicate the concentration profile of cefazolin as it is cleared from the subcutaneous tissue over time. This is especially important due to cefazolin's nature as a time-dependent antibiotic [9]. The serum half-life of intravenous cefazolin is only approximately 1.8 hours [10], although Dubrovsky et al. [11] observed a half-life of approximately 4.4 hours after subcutaneous administration in a porcine model. Meanwhile, an hour after administration with UD2, the mean cefazolin tissue concentration in the aforementioned study on the elective abdominoplasty patients was approximately 520 mg/L, nearly the same as the highest MIC of the isolates we studied [6]. Further study using an in vitro pharmacodynamic model would be helpful in assessing the impact of the changing concentration of the rate and extent of kill.
Conclusions
In summary, we investigated the effect of the average tissue concentration of cefazolin achieved when administered using UD2 against MRSA isolates in an in vitro time-kill study. The bactericidal effects demonstrated in these experiments support the use of cefazolin against MRSA infections that can be addressed with this procedure. Additional studies focused on the pharmacokinetic and pharmacodynamic profiles of cefazolin in the subcutaneous environment are needed to fully explore the viability of UD2 of this compound in the management of MRSA infection.
Footnotes
Acknowledgments
The authors thank Janice Cunningham, Elizabeth Cyr, Nicole DeRosa, Lauren McLellan, Elias Mullane, Alissa Padgett, Julio Rodriguez, Rebecca Stewart, and Ceara Wettemann from the Center for Anti-Infective Research and Development, Hartford Hospital for their assistance with the conduct of this study.
Funding Information
No funding was received for this study.
Author Disclosure Statement
Dr. Silberg and Dr. Nicolau are shareholders in Sonescence, Inc., the developer of the UD2 technique. No other competing financial interests exist.