
Abstract
Background:
Peri-prosthetic joint infection (PJI) is a debilitating and costly complication of joint replacement. Synovial fluid cultures are negative in up to 25% of PJI cases. The purpose of this study was to compare the clinical characteristics and outcomes of culture negative and culture positive PJI.
Patients and Methods:
We conducted a retrospective study including all patients aged 18 and older admitted to a single tertiary-care hospital between 1998 and 2015 diagnosed with PJI and treated with antibiotic agents and surgery.
Results:
One hundred ninety-six patients with PJI were identified; 48 (24.5%) were culture-negative (CN) and 148 (75.5%) were culture-positive (CP). The groups were similar in age and presence of associated comorbidities. Fever was more common among the CP patients (CN, 23.8%; CP, 38.4%; p = 0.03) as was sepsis defined by Sepsis-2 criteria (CN, 12.8%; CP, 28.7%; p = 0.03). Patients who were CP had higher synovial white blood cell (WBC) count (CN, 30,500 per milliliter; CP, 95,400 per milliliter; p < 0.01), a longer length of stay (CN, 3.8%; CP,7.9%; p = 0.02), and fewer alternative diagnoses established within one year (CN, 25.0%; CP, 2.7%; p < 0.01). Our logistic regression models also found that CP patients had an adjusted odds ratio (OR) of 2.59 for rehabilitation placement with 95% confidence interval (CI) of 1.15–5.83 and adjusted OR of 0.04 for an alternative diagnosis within one year with 95% CI, 0.009–0.22 compared with their CN counterparts.
Conclusions:
This study suggests that patients with CN PJI have less severe disease, better outcomes, and higher rates of alternative diagnoses within one year.
In the past several decades, the incidence of septic arthritis has risen in the United States, especially among the elderly and chronically ill [1]. One contributor to this trend is the increase in joint replacement surgeries, which may be complicated by peri-prosthetic joint infection (PJI). Joint replacement surgeries are performed frequently, with close to a million procedures a year in the United States alone. With the aging of the population, the number of joint replacement surgeries is expected to reach 572,000 for hips and 3.48 million for knees by 2030 [2]. Peri-prosthetic joint replacement may complicate knee replacements in 0.86%–1.1% of cases [2,3] and hip replacements in 0.3%–1.7% of cases [3–5]. Although the overall rates of PJI are low, these complications are often costly, debilitating, and affect the lives of up to 22,000 patients per year [6,7]. Synovial fluid cultures are negative in up to 25% of these cases, making the diagnosis of PJI and its management challenging [8].
Because of the substantial morbidity associated with PJI [9,10], cases of suspected joint infection are often treated aggressively with early surgical intervention [11]. Surgical intervention may be associated with repeat procedures and substantial morbidity and mortality [12]. It is not clear whether surgery is superior to medical management of cases of clinically suspected culture-negative (CN) PJI, because outcomes of cases treated with either approach have never been compared carefully. Indeed, to our knowledge, there are currently no available guidelines or data to guide the differential treatment for culture-positive (CP) versus CN prosthetic joint septic arthritis (PJISA), because CN cases are often excluded from studies.
We hypothesized that patients with CN and CP PJI would be different in their clinical course and outcomes, which might warrant consideration of a more conservative approach in the CN group. The purpose of this study was to compare demographic features, clinical characteristics, and outcomes between those with CN PJI and their CP counterparts.
Patients and Methods
Study design
We conducted a retrospective chart review study of patients with PJI admitted to a single tertiary care center from 1998 to 2015. Permission was obtained to review data retrospectively based on medical record review from the Beth Israel Deaconess Medical Center Institutional Review Board. All authors attest to the accuracy of the reported data and analyses.
Study population
Eligible patients 18 years or older were identified using an International Classification of Disease, Ninth Revision (ICD-9) code for clinically suspected septic arthritis. We included patients with documented infection in their prosthetic joint for which surgery was performed during the index admission. Patients who were CP were defined as having any positive result of the following: synovial fluid gram stain, synovial fluid culture, synovial tissue biopsy gram stain, or synovial tissue biopsy culture. Patients who were CN had negative results in all four of these tests during their admission.
We excluded patients with a prosthetic joint that had been removed from the index joint prior to admission or patients with polyarticular septic arthritis, septic bursitis, or osteomyelitis. Patients were also excluded if they had a related episode of septic arthritis in the index joint within 90 days prior to admission.
Data collection
After identification of eligible patients, the electronic medical record for each patient was reviewed to obtain demographic data and information regarding comorbidities at the time of the index admission, presenting clinical and laboratory features, sites of joint involvement, synovial fluid data, and timing of antibiotic administration and operative intervention, if any. Sepsis-2 criteria were applied (≥2 systemic inflammatory response syndrome [SIRS] criteria plus infection) to define sepsis. Systemic inflammatory response syndrome was defined as the presence of more than one of four findings: body temperature >38.0°C or <36.0°C, heart rate >90 beats per minute, tachypnea >20 breaths per minute or hyperventilation with arterial carbon dioxide partial pressure <32 mm Hg, white blood cell (WBC) count >12,000 cells/mm3 or <4,000 cells/mm3 [13,14]. Length of hospital stay (LOS), admission to the intensive care unit (ICU), discharge to a rehabilitation facility, 60-day re-admission rates, and 30-day mortality rates also were determined. Note was made of subsequent operative interventions on the index joint. Surgery included arthroscopic, open, or irrigation and debridement (usually with liner exchange). Any non-infectious alternative diagnosis made either during the index admission or within one year of discharge was noted. De-identified data were stored securely in the Research Electronic Data Capture (REDCap), an institutionally available Web-based data repository.
Groups
Patients with septic arthritis were divided into those with CP or CN. Patients with CP PJI were compared with those with CN PJI with respect to presenting features, type of operation, and outcomes.
Outcomes
Outcomes included LOS, 60-day re-admission rates, ICU admission rates, rates of operative intervention during the index admission, discharge to a rehabilitation facility, 30-day mortality, need for additional operative interventions post-discharge, and alternative diagnoses within one year of the index admission.
Statistical analysis
Differences between groups for continuous variables were analyzed using the Student two-sample t-test or the Mann-Whitney U test where appropriate. Differences in groups between categorical variables were tested using the χ2 test or Fisher exact test where appropriate. A p value of <0.05 was considered as significant.
To compare outcomes between the CP and CN groups, we constructed both unadjusted and adjusted logistic regressions. Outcomes of interest included LOS, ICU admission, rehabilitation placement after inpatient stay, re-admission after 60 days, and if an alternative diagnosis within one year was found. We performed unadjusted logistic regression computing the odds ratio for each outcome based on culture positivity. We performed adjusted logistic regression computing the odds ratio for each outcome based on culture positivity with several covariates included in the regression. We included age, gender, multiple admissions, medical conditions such as chronic kidney disease (CKD), diabetes mellitus (DM), hepatitis C virus (HCV), human immunodeficiency virus (HIV), immunosuppression, rheumatoid arthritis, septic arthritis, and joint trauma. For ICU admission outcomes the presence of sepsis was included in the adjustment. To measure the effects of culture positivity on LOS, an ordered categorical variable with more than two values, ordered logistic regressions were formed. The odds ratios reported for these models are thus proportional odds ratios. Analysis was conducted in Stata, version 13 (StataCorp, College Station, TX).
Results
Characteristics of the study population
Over a period of 17 years (1998–2015), we identified a total of 196 patients with prosthetic joint septic arthritis for which surgery was performed in a single tertiary medical center. Of these, 48 (24.5%) had negative cultures and 150 (75.5%) had positive cultures. Culture-positive patients were more likely to have a prior history of septic arthritis, including episodes in both the index and non-index joints (CN, 10.4%; CP, 24.3%). The two groups were otherwise similar with respect to age, gender, race, and ethnicity with no difference in the prevalence of comorbidities or known medical risk factors for septic arthritis (Table 1).
Demographics and Comorbidities of Patients with Prosthetic Joint Septic Arthritis
CN = culture-negative; CP = culture-positive; SD = standard deviation; HIV = human immunodeficiency virus; SA = septic arthritis.
Characteristics of the index joint
The knee was the joint most commonly affected in both groups and was more frequently involved in the CN (91.7%) than the CP (67.6%) cases (p < 0.01). The hip joint was more frequently involved in the CP (27.7%) than the CN (8.3%) cases (p = 0.01). Figure 1 compares the prevalence of CN versus CP PJI for each joint.
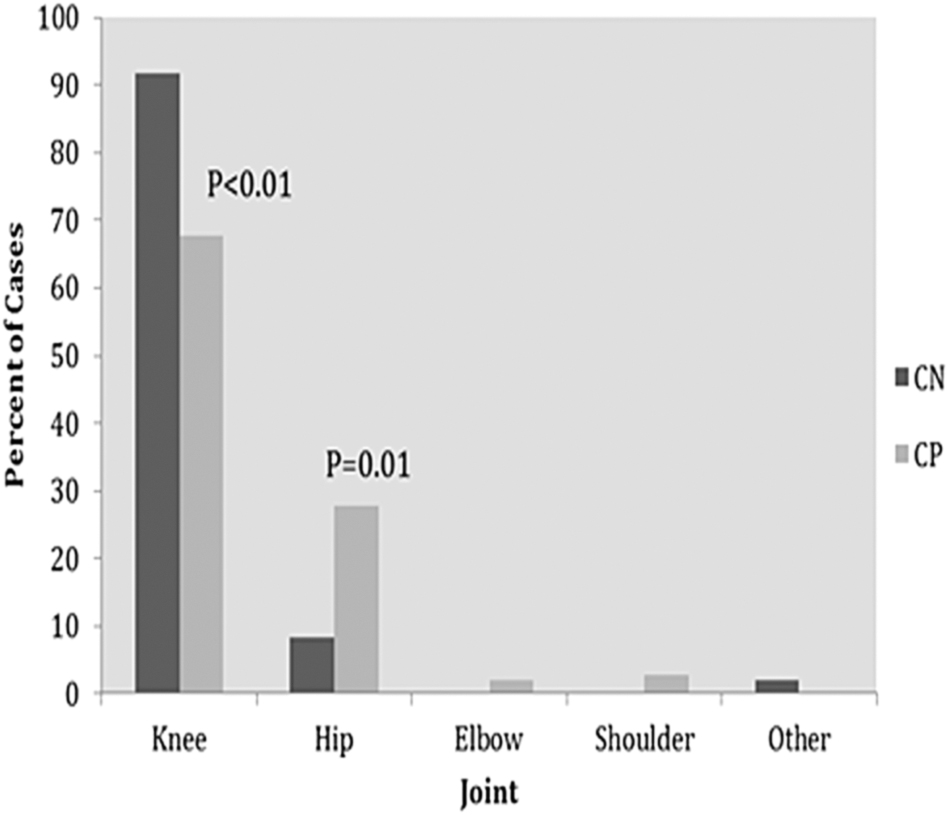
Joint involvement of patients with prosthetic joint septic arthritis stratified by culture results. CP = culture-positive; CN = culture-negative.
Duration of symptoms and timing post-prosthesis insertion
The duration of symptoms prior to admission was similar in both groups (CN, 13.6 days; CP, 10.6 days; p = 0.50). Additionally, the two groups did not differ in the percentage of patients with persistent symptoms, defined as septic arthritis symptoms persisting for at least 28 days prior to admission (CN, 13.2%; CP, 12.2%; p = 0.88). Culture-negative patients had, on average, a shorter number of days from prosthetic insertion to admission than CP patients (CN, 633.1 days; CP, 1,270.7 days; p = 0.02). When separated by interval, CN patients were also more likely to present early (0–42 days from prosthetic insertion; CN, 33.3%; CP, 14.9%; p = 0.01). No differences were noted in the prevalence of delayed and late admissions (Table 2).
Duration of Symptoms and Timing of Admission Relative to Initial Joint Replacement Surgery among Patients with Prosthetic Joint Septic Arthritis
Early, delayed, and late refer to time between insertion of prosthesis and diagnosis of septic arthritis: early = 0–42 d; delayed = 43–365־ d; late = >365 d.
CN = culture-negative; CP = culture-positive; SD = standard deviation.
Clinical characteristics
Culture-negative patients were less likely than CP patients to present with fever (CN, 23.8%; CP, 38.4%; p = 0.03) and sepsis, defined by Sepsis-2 criteria (CN, 12.8%; CP, 28.7%; p = 0.03). The two groups were similar with respect to mean WBC count, mean percentage of polymorphonuclear (PMN) cells, and degree of elevation of inflammatory markers (Table 3).
Clinical Features of Patients with Prosthetic Joint Septic Arthritis
CN = culture-negative; CP = culture-positive; WBC = white blood cell count; SD = standard deviation; PMN = polymorphonuclear lymphocyte; ESR = erythrocyte sedimentation rate; CRP = C-reactive protein.
Synovial fluid
The mean synovial WBC of the CP group was 95,400 per milliliter, whereas the CN patients had a mean synovial WBC of 30,500 per milliliter (p < 0.01). Culture-positive cases also demonstrated higher percentage of synovial fluid PMNs (CN, 77.0; CP, 90.1; p < 0.01; Table 3).
Microbiology
The mean number of blood cultures and synovial fluid cultures per patient in our cohort was 10.71 ± 5.93 and 2.44 ± 0.9, respectively. During the study period, the incubation time for specimens varied but was never less than five days and at times up to 14 days for tissue biopsy specimens obtained from revision surgeries.
The most common pathogens found in the CP group were methicillin-sensitive Staphylococcus aureus (MSSA; 52 cases; 35.1%), coagulase-negative staphylococci (CoNS) species (34 cases; 23.0%), and methicillin-resistant Staphylococcus aureus (MRSA; 23 cases; 14.9%). When stratified by time post-joint replacement, MSSA was the most prevalent organism in early (40.9%), delayed (29.8%), and late (32.9%) groups. Alphabetical lists of all isolated organisms stratified by joint distribution and time intervals post prosthetic insertion are available in Supplementary Table S1 and Table S2.
Antibiotic choice
The majority of the patients in both groups received antibiotic agents after the diagnostic aspiration (CN, 56.3%; CP, 61.5%; p = 0.52; Supplementary Table S3). Vancomycin was the most commonly prescribed antibiotic (CN, 91.7%; CP, 84.5%; p = 0.21), followed by cefazolin (CN, 25.0%; CP, 33.1%; p = 0.29) and ceftriaxone (CN, 37.5%; CP, 27.0%; p = 0.17). Nafcillin was administered to a greater proportion of CP (17.6%) than CN (4.2%) cases (p = 0.02; Supplementary Table S3). Vancomycin was also the most common initial empiric treatment for both CN (62.5%) and CP (67.6%) cases (p = 0.52; Supplementary Table S4).
Surgery
An arthroscopic procedure was performed in 10.4% of the CN patients and in 0.7% of the CP patients (p < 0.01). Arthroscopic procedures were performed only for knee PJI. Surgeons documented the presence of pus in 29.6% of CN patients and 68.4% of CP patients (p < 0.01). The prosthesis was removed in 45.9% of the cases. Table 4 outlined the rates of each operation stratified by the CN and CP groups.
Operative Findings and Type of Surgery Stratified by Culture Results
An antibiotic spacer was inserted more commonly when the patients presented late (e.g., >365 days post-prosthetic insertion; p = 0.01) whereas incision and debridement only was more commonly performed when patients presented early (0–42 days post-prosthetic insertion; p < 0.01; Fig. 2).
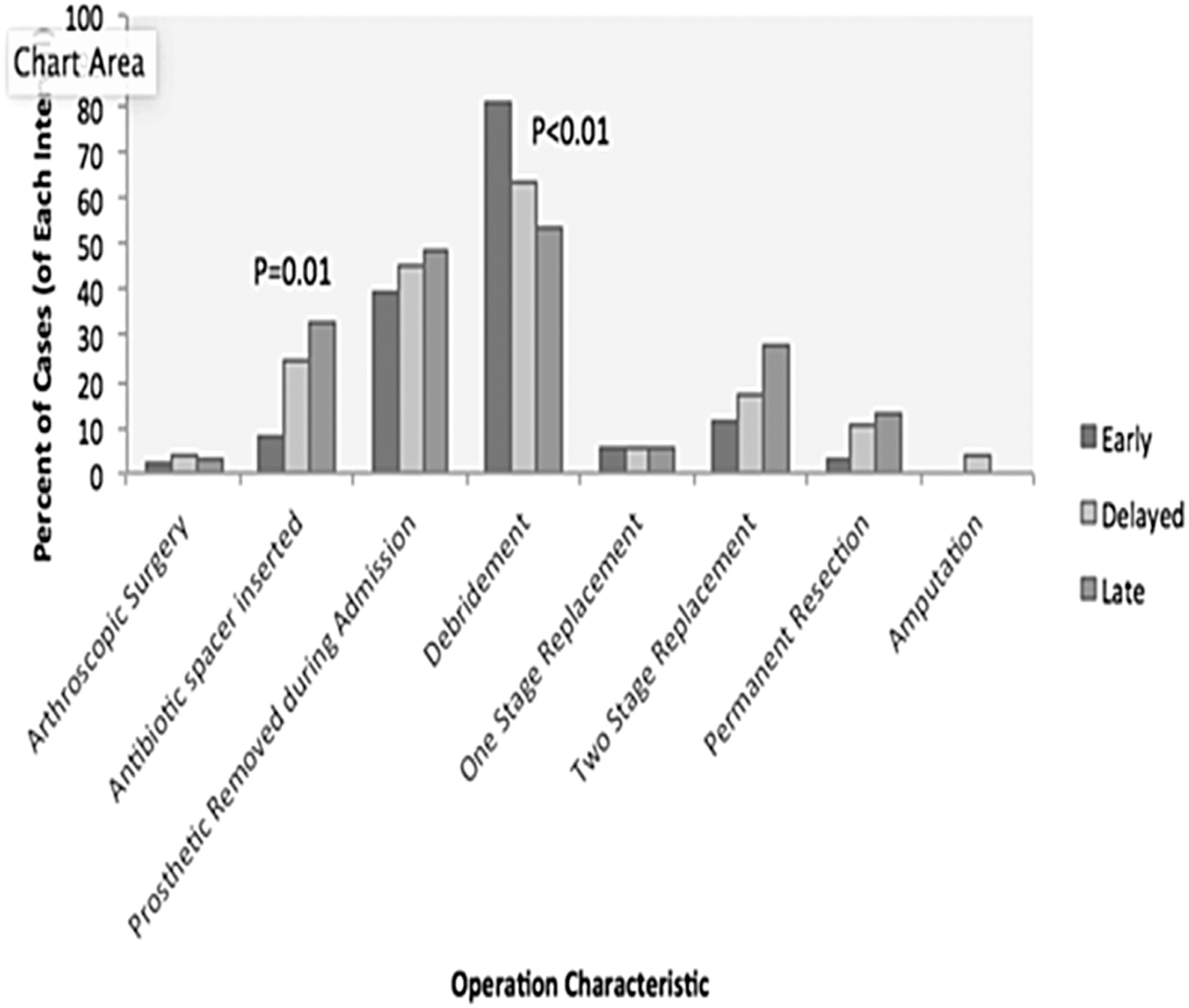
Type of surgery stratified by time after initial joint replacement surgery.
When stratified by prior incidence of septic arthritis, patients with a history of septic arthritis were more likely to have an antibiotic spacer inserted (no septic arthritis, 19.4%; septic arthritis, 48.8%; p < 0.01) and prosthetic removed during admission (no septic arthritis, 40.7%; septic arthritis, 65.9%; p < 0.01). These patients with prior septic arthritis were also less likely to have a debridement (no septic arthritis, 69.0%; septic arthritis, 36.8%; p < 0.01) but more likely to have a two-stage joint replacement (no septic arthritis, 16.2%; septic arthritis, 39.5%; p < 0.01; Table 5).
Type of Surgery among Patients with Prosthetic Joint Septic Arthritis Stratified by Prior History of Septic Arthritis
SA = septic arthritis.
Operative characteristics also differed by acute versus chronic symptom duration, defined as symptoms persisting for fewer or greater than 28 days. Patients with chronic symptoms were more likely to have an antibiotic spacer inserted (acute, 20.3%; chronic, 52.4%; p = 0.01) and prosthetic removed during admission (acute, 41.9%; chronic, 66.7%; p = 0.03). Patients with acute symptoms were more likely to receive debridement (acute, 68.2%; chronic, 28.6%; p < 0.01). Those with chronic symptoms had greater prevalence of both two-stage resection (acute, 17.6%; chronic, 42.9%; p = 0.01) and permanent resection (acute, 6.8%; chronic, 23.8%; p = 0.01; Table 6).
Type of Surgery among Patients with Prosthetic Joint Septic Arthritis Stratified by Symptom Duration
Acute = symptom duration ≤28 d. Chronic = symptom duration >28 days.
Outcomes
Culture-positive patients had a longer LOS (CN, 3.8%; CP, 7.9%; p = 0.02) and rates of discharge to a rehabilitation facility (CN, 52.1%; CP, 68.3%; p = 0.04). Rates of admission to an ICU did not differ substantially. However, CN patients had a higher prevalence of alternative diagnoses within one year (CN, 25.0%; CP, 2.7%; p < 0.01; Table 7). Among the patients who received alternative diagnoses, one was diagnosed with psoriatic arthritis, one with rheumatoid arthritis, two with gout, one with dysplastic tibial lesion, and the other seven were diagnosed with surgical site hematoma or skin cellulitis. Thus, in those seven cases the diagnoses were likely made in retrospect when cultures proved negative.
Outcomes for Patients with Prosthetic Joint Septic Arthritis
CN = culture-negative; CP = culture-positive; LOS = length of stay; SD = standard deviation; ICU = intensive care unit.
Logistic regression
We developed models to measure the effect of culture positivity in prosthetic joint presumed septic arthritis. We found that both unadjusted and adjusted ordered logistic models did not reveal differences in LOS between the CP and CN groups with adjusted OR of 1.47 and 95% CI, 0.78–2.76. The adjusted OR of ICU admission rates and re-admission rates after 60 days did not differ between the two groups.
Our outcomes models did find an effect for the need for rehabilitation, with those in the CP group having an adjusted OR of 2.35 for discharge to a rehabilitation facility, 95% CI, 1.15–5.83. Culture-positive PJI was also strongly associated with a lack of an alternative diagnosis within the next year with an adjusted OR of 0.04 and 95% CI, 0.009–0.22 (Table 8).
Effects of Culture Positivity on Health Outcomes in Patients with Prosthetic Joint Septic Arthritis
OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit; LOS = length of stay; ICU = intensive care unit; CP = culture positive.
Unadjusted OR calculated using a logistic regression with CP as the independent variable. Dependent variables are displayed in the left column.
Adjusted OR calculated using a multrvariable logistic regression with CP as the independent variable.
Discussion
In this study, we compared the clinical characteristics, management, and outcomes of CN versus CP PJI. Culture-positive patients were more likely to present with fever, sepsis, and highly inflammatory synovial fluid. Vancomycin was the antibiotic most commonly prescribed for both groups. They also had a similar prevalence of types of operations. Culture-positive patients were more likely to have longer hospital stays and the need for outpatient rehabilitation. An alternative diagnosis was found in 25.0% of the CN patients within a year.
Our observations suggest that the CN group is less systemically ill than patients with CP PJI. It appears that the CN patients may represent a different clinical entity that might benefit from a more conservative approach, especially if one considers the relatively high rate of alternative diagnoses established within year. This reported rate also might underestimate the true rate of an alternative diagnosis, as it is likely that at least some patients were followed in other institutions.
This work is timely, as the number of prosthetic joint replacements is expected to increase with an aging U.S. population. At the current time, there are an estimated 4.7 million Americans with a total knee arthroplasty (TKA) and 2.5 million with a total hip arthroplasty (THA) [15]. Approximately 1% of joint replacement surgeries are complicated by joint infections. Infectious disease specialists have reported that of these, 3%–35% are CN PJI [16]. However, there is currently little information on CN PJI, because these cases are often excluded from studies. Many of these cases may represent non-infectious inflammatory conditions such as gout or aseptic hardware loosening [17] rather than true infections. Other considerations include atypical organisms undetected by a traditional culture [18] and the administration of antibiotic agents prior to specimen collection [19].
Current practice suggests that patients with CP PJI should be managed surgically rather than with antibiotic agents alone [20,21]. However, with a short duration of symptoms (less than one month) and negative cultures, it is possible that an episode of PJI could be managed successfully with antibiotic therapy and without surgery [22]. We found that the prevalence of the operation types did not differ between CP and CN cases. This indicates that CN cases are being managed, in effect, as CP cases. Often, patients are treated aggressively and brought to the operating room before culture results return. Non-surgical management of CN PJI may be appropriate considering the risks inherent in an open, double procedure [23], especially for the elderly [24,25]. Current preferences in the care of CN PJI patients are often based on a lack of robust evidence. This contributes to wide variation in treatment strategy. With a high prevalence of joint replacements, there is a pressing need for evidence-based guidelines. Ideally, we will have randomized controlled trials of CN PJI comparing surgery versus conservative management to guide guideline development.
There are several limitations to this study. The study population was derived from a single tertiary referral center, which limits the diversity of the study population with higher prevalence of sick and complex patients. During the study period, which spanned 17 years, metagenomic techniques were not readily available. In recent years, many institutions have utilized polymerase chain reaction (PCR) testing, which may increase the diagnostic yield among CN patients. Additionally, at times the source of infection (peri-operative vs. hematogenous vs. contiguous skin) was either not known or not documented. Another limitation, common to retrospective studies reliant on medical chart review, was incomplete or variable reporting of clinically relevant data. The rationale for choice of surgical approach was not routinely documented. Follow-up data for patients seen in other institutions and functional outcomes were not routinely available.
Conclusions
Our findings support the concept that CN PJI is a different clinical entity from CP PJI with different clinical courses and outcomes. Future prospective randomized trials are warranted to provide evidence for optimal management of these cases.
Footnotes
Acknowledgments
This study was approved by Beth Israel Deaconess Medical Center review board. All data are available from the corresponding author upon request.
Funding Information
No funding was received for this study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.