
Abstract
Background:
Pseudomonas aeruginosa is isolated at variable rates from intra-abdominal infections (IAI). Not all recommended empiric regimens for IAI include anti-Pseudomonas aeruginosa activity, for example, ceftriaxone and metronidazole. We hypothesized that within an adult population, Pseudomonas aeruginosa is a relatively rare isolate and has no association with mortality, and thus, empiric therapy with anti-Pseudomonas aeruginosa activity is not warranted.
Patients and Methods:
All IAI with positive cultures treated between 1997 and 2017 at a single institution were analyzed. This data set was divided into two cohorts, namely, those with cultures positive for Pseudomonas aeruginosa and those without. Demographics and in-hospital mortality were compared by Student t-test and χ2 analysis. Predictors of isolation of Pseudomonas aeruginosa and in-hospital mortality were done by logistic regression (LR) analysis.
Results:
In total, 2,420 IAIs were identified, 104 (4.3%) with Pseudomonas aeruginosa and 2,316 (95.7%) without. Major demographic differences between patients with Pseudomonas aeruginosa and those without included a higher rate of health-care–associated infections (87/104, 83.7% vs. 621/2316, 26.8%; p = 0.02), a higher rate of intensive care unit (ICU)-acquired infections (23/104, 22.1% vs. 329/2316, 14.2%; p = 0.04) and a higher Acute Physiology and Chronic Health Evaluation (APACHE) II score (17.7 ± 0.8 vs. 14.5 ± 0.2; p < 0.0001). There was an increased rate of Pseudomonas aeruginosa isolation with increasing APACHE II score. Independent predictors of isolation of Pseudomonas aeruginosa by LR included APACHE II score and days of hospitalization prior to diagnosis. Crude in-hospital mortality was similar between groups: Pseudomonas aeruginosa 14/104 (13.5%) and 276/2316 (11.9%), p = 0.79. After controlling for age, gender, APACHE II, prior transfusion, immunosuppression status, solid organ transplant status, healthcare-association, and days of hospitalization prior to diagnosis, the isolation of Pseudomonas aeruginosa was not associated with mortality.
Conclusion:
Pseudomonas aeruginosa is infrequently isolated and overall not associated with mortality. Nonetheless, there may be a population that merits empiric anti-Pseudomonas aeruginosa therapy: those with APACHE II ≥20 or a significant length of hospitalization prior to diagnosis.
Intra-abdominal infections (IAI) encompass a wide variety of pathologies ranging in severity from uncomplicated appendicitis to peritonitis [1]. Complicated IAIs affect multiple organs in peritonitis. Treatment modalities conventionally include source control and antimicrobial therapy [2]. However, the latter is often a challenge because of the often polymicrobial etiology of IAIs. Major pathogens isolated are largely from the Enterobacteriales family, including Escherichia coli, Klebsiella spp., Salmonella spp., Shigella spp., and Yersinia pestis [3,4]. The 2014 Complicated intra-abdominal infections worldwide observational study (CIAOW) study, a multicenter observational study of IAIs in 1,898 patients across 68 medical institutions worldwide, found that Pseudomonas aeruginosa comprised 5.1% of all identified bacterial isolates and 5.6% of all micro-organisms isolated in the intra-operative samples [3].
Given its relatively low prevalence, treatment of Pseudomonas aeruginosa presents a unique challenge of equipoise. Its large genome enables a broad arsenal of antibiotic resistance mechanisms, encompassing agents from almost every class of antibiotic agents, including piperacillin-tazobactam, cefepime, meropenem, imipenem, any aminoglycoside, and ciprofloxacin [5]. However, evidence-based empiric antimicrobial regimens for IAI often do not include anti-Pseudomonas aeruginosa activity, for example, the use of ceftriaxone and metronidazole, and there is no consensus on whether to empirically treat for Pseudomonas aeruginosa in the context of IAIs [6,7]. Additionally, although inappropriate antibiotic selection has been associated with mortality, it remains unclear whether there is a survival benefit associated with the inclusion of anti-Pseudomonas aeruginosa activity in empiric treatment [8].
We hypothesized that within an adult population, Pseudomonas aeruginosa is a relatively rare isolate, has no association with mortality, and that empiric therapy with anti-Pseudomonas aeruginosa activity is not warranted. The purpose of the study was to describe the prevalence of and risk factors for the isolation of Pseudomonas aeruginosa from patients with IAI, as well as to assess the importance of empirical anti-Pseudomonas aeruginosa therapy.
Patients and Methods
This project was approved by the University of Virginia Institutional Review Board and the need for informed consent was waived. Inclusion criteria included all patients older than 18 years treated for IAI with positive cultures between 1997 and 2017 as inpatients at a single hospital. No specific institutional guidelines were in place related to spectrum of antimicrobial coverage for IAI during this period. This data set was divided into two cohorts, namely those with cultures positive for Pseudomonas aeruginosa and those without.
Potential risk factors for the isolation of Pseudomonas aeruginosa and mortality were chosen a priori and included age, gender, Acute Physiology and Chronic Health Evaluation (APACHE) II score at time of infection diagnosis, prior cellular transfusion, immunosuppression status, solid organ transplant status, healthcare-association, and days of hospitalization prior to diagnosis. For the purposes of this study, empiric anti-Pseudomonas aeruginosa activity included regimens containing piperacillin-tazobactam, cefepime, meropenem, imipenem, any aminoglycoside, or ciprofloxacin. Neither ceftazidime nor levofloxacin were used empirically.
Demographics and in-hospital mortality were compared by Student t-test and χ2 analysis. Primary outcomes of predictors of isolation of Pseudomonas aeruginosa and in-hospital mortality were analyzed using logistic regression (LR) analysis. A second LR for mortality was performed in a similar manner to the first except for addition of the variable “received empiric anti-Pseudomonas aeruginosa therapy.” Secondary outcomes were also analyzed using LR.
Results
In total, 2,420 IAIs were identified, 104 (4.3%) with Pseudomonas aeruginosa and 2,316 (95.7%) without Pseudomonas aeruginosa. Demographics are provided in Table 1. Major differences between patients with Pseudomonas aeruginosa and those without included a higher rate of health-care–associated infections (87/104, 83.7% versus 621/2316, 26.8%; p = 0.02), a higher rate of intensive care unit (ICU)-acquired infections (23/104, 22.1% versus 329/2316, 14.2%; p = 0.04) and a higher APACHE II score (17.7 ± 0.8 versus 14.5 ± 0.2; p < 0.0001). There was an increased rate of Pseudomonas aeruginosa isolation with increasing APACHE II score (Fig. 1).
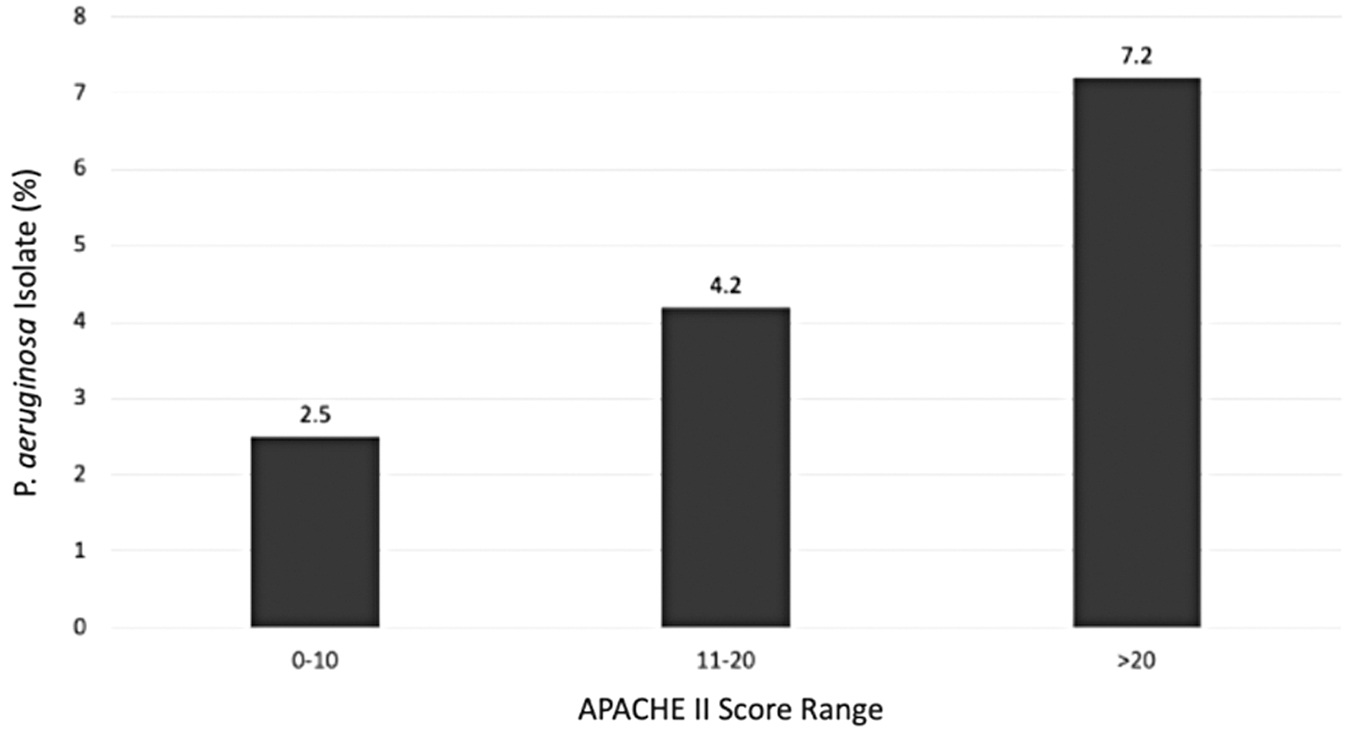
Association between Pseudomonas aeruginosa isolate percentage and Acute Physiology and Chronic Health Evaluation (APACHE) score range.
Patient Demographics and Outcomes
CAD = cardiovascular disease; DM = diabetes mellitus; ICU = intensive care unit; APACHE II = Acute Physiology and Chronic Health Evaluation II.
Major outcomes are given in Table 1. Duration of therapy, length of stay, and in-hospital mortality were all similar between groups. Independent predictors of isolation of Pseudomonas aeruginosa by LR included APACHE II score and days of hospitalization prior to diagnosis (Table 2).
Multivariable Analysis of Risk Factors for the Isolation of Pseudomonas aeruginosa
C statistic = 0.77, Hosmer-Lemeshow test = 0.20
OR = odds ratio; CI = confidence interval; APACHE II = Acute Physiology and Chronic Health Evaluation II.
Independent predictors of mortality included age, APACHE II status, and receipt of cellular transfusion prior to the diagnosis of infection, but not isolation of Pseudomonas aeruginosa (Table 3). Of the 2,420 IAIs treated, 2,022 (83.6%) received an empiric regimen including anti-Pseudomonas aeruginosa activity. The most commonly used empiric agent with anti-Pseudomonas aeruginosa activity was piperacillin-tazobactam. Crude mortality for patients receiving empiric anti-Pseudomonas aeruginosa therapy was 11.9% (240/2,022) compared with 12.6% (50/398) not receiving anti-Pseudomonas aeruginosa empiric therapy (p = 0.70 for the difference). By LR, including the receipt of empiric anti-Pseudomonas aeruginosa therapy was associated with a lower mortality compared with other regimens, even though the isolation of Pseudomonas aeruginosa was still not a predictor of mortality (Table 4).
Multivariable Analysis of Risk Factors for Mortality after Intra-Abdominal Infection, Excluding Receipt of Empiric Anti-Pseudomonal Therapy
C statistic = 0.85, Hosmer-Lemeshow test = 0.061.
OR = odds ratio; CI = confidence interval; APACHE II = Acute Physiology and Chronic Health Evaluation II.
Multivariable Analysis of Risk Factors for Mortality after Intra-Abdominal Infection, Including Receipt of Empiric Anti-Pseudomonal Therapy
C statistic = 0.85, Hosmer-Lemeshow test = 0.28.
OR = odds ratio; CI = confidence interval; APACHE II = Acute Physiology and Chronic Health Evaluation II.
Discussion
The optimal management of IAIs remains controversial. Some of this controversy is related to the frequency of polymicrobial infection and whether or not antimicrobial management needs to provide activity against some or all of the causative pathogens. Pseudomonas aeruginosa and the Enterococcus species are the most common pathogens that are isolated with some regularity but are not susceptible to many commonly prescribed antibiotic regimens, specifically those based on first-, second-, or most third-generation cephalosporins. We sought to document the prevalence of Pseudomonas aeruginosa isolation in adults with IAI and determine risk factors for both isolation of Pseudomonas aeruginosa as well as mortality from IAI.
Our data suggest a relatively low prevalence of Pseudomonas aeruginosa in IAI (4.3%), a number consistent with the global CIAOW study (5.1%) and other studies describing a prevalence between 4% and 9% [3,9–11]. In addition, the crude mortality for infections with Pseudomonas aeruginosa and those without Pseudomonas aeruginosa were similar. In isolation, those two figures alone suggest that in this era of increasingly resistant micro-organisms with antimicrobial stewardship efforts focused on preserving the utility of available drugs, routine use of empiric agents with anti-Pseudomonas aeruginosa activity is not indicated.
Unexpectedly, although the isolation of Pseudomonas aeruginosa was not associated with outcomes, the receipt of empiric anti-Pseudomonas aeruginosa therapy was associated with survival. However, agents typically used for empiric anti-Pseudomonas aeruginosa therapy often have a wide breadth of coverage that includes all gram-negative bacilli. This may partly explain the unexpected mortality benefit. Previous studies have described how gram-negative bacteria are commonly isolated and are and have an alarmingly high rate of morbidity and mortality [12,13]. Overall, it remains unclear whether differences in outcomes are related specifically to a specific regimen's anti-Pseudomonas aeruginosa activity or the overall breadth of spectrum. Previous studies have addressed the difficulty in selecting appropriate initial antibiotic therapy for IAIs given lack of universal classification systems [14].
Despite the seeming contradictory nature of our data, it is possible to speculate which patients would benefit most from empiric anti-Pseudomonas aeruginosa antimicrobial therapy. Because the isolation of Pseudomonas aeruginosa was related to severity of illness, one group may be those with severe illness. Indeed, Ballus et al. [15] isolated Pseudomonas aeruginosa in 19.3% of patients with a mean APACHE II score of 19.7 ± 7.8, and our findings are further consistent with several studies that showed that the risk of developing nosocomial infections increased with high APACHE II score [16,17]. A second group of patients that may benefit from empiric anti-Pseudomonas aeruginosa therapy includes the immunosuppressed in whom inadequate empiric therapy may have a more serious consequence. Finally, it is unclear whether or not healthcare-acquisition is enough of a risk factor for the isolation of Pseudomonas aeruginosa that routine empiric anti-Pseudomonas aeruginosa therapy is warranted outside of the other risk factors noted above. A long-standing discussion, the benefit of avoiding unnecessary therapy must be weighed against the cost of initial antibiotic treatment failure that has been associated with MDR pathogens such as Pseudomonas aeruginosa [18–22].
Our study has a few important limitations to consider. Its retrospective nature precludes accounting for any changes in antibiotic stewardship practices or other institutional changes that occurred within the study frame. Additionally, assessing the presence of Pseudomonas in the context of intra-abdominal infections may be difficult when a majority of patients (83%) have received anti-Pseudomonas aeruginosa therapy. Timing of antimicrobial therapy may vary and introduce a mild degree of sampling error. In addition, because microbiology laboratories do not routinely identify more than the three most prevalent bacteria, there is a real possibility that Pseudomonas aeruginosa are present in substantially more infections than we noted using culture-based techniques. High-quality metagenomics could answer this question more thoroughly. Recognizing these limitations, a future study design would be to collect data on patients with IAI prospectively and randomize them to either an empiric anti-Pseudomonas aeruginosa therapy group or a control group based on their risk and severity of illness.
Conclusions
Surgical infections remain a persistent source of morbidity and mortality. Intra-abdominal infections often are caused by multiple organisms and require a particularly nuanced approach, namely which organisms to empirically cover in the context of increasing antimicrobial resistance. For example, we present data that indicates a low prevalence of Pseudomonas aeruginosa. Given the low prevalence of Pseudomonas aeruginosa, empiric therapy for low-risk, low severity of illness IAIs should not include anti-Pseudomonas aeruginosa activity. However, vulnerable populations such as those with prolonged hospital stays or who are critically ill may benefit from empiric anti-Pseudomonas aeruginosa therapy.
Footnotes
Acknowledgments
The authors would like to thank the Departments of Surgery at the University of Virginia and Western Michigan University.
Funding Information
No funding was received to support this study.
Author Disclosure Statement
Jesse Chou has no commercial associations to disclose. Dr. Knight has no commercial associations to disclose. Dr. Sawyer has no relevant commercial associations to disclose.