
Abstract
Background:
In this systematic review and meta-analysis, we aimed to assess the clinical efficacy and safety of cefoperazone–sulbactam against alternative antibiotics in the treatment of intra-abdominal infections.
Methods:
The PubMed, Cochrane, Web of Science, Ovid Medline, and CKNI databases were searched for relevant articles up to November 25, 2020. The primary outcome was clinical efficacy rate, and the secondary outcomes were microbiologic eradication rate, mortality rate, and adverse event (AE) risk.
Results:
Twelve studies involving 1,674 patients were included. Overall, the clinical efficacy rate of cefoperazone–sulbactam and comparators was 87.7% and 81.7%, respectively, and cefoperazone–sulbactam was associated with a higher clinical efficacy rate than that the comparator (odds ratio [OR] 1.98; 95% confidence interval [CI] 1.31–3.00; I2 = 36%). Additionally, cefoperazone–sulbactam was associated with a lower clinical failure rate (OR 0.40; 95% CI 0.28–0.57; I2 = 0) and a higher clinical cure rate (OR 1.54; 95% CI 1.17–2.03; I2 = 0) than the comparators. Cefoperazone–sulbactam was associated with a higher microbiologic eradication rate than the comparator (OR 2.54; 95% CI 1.72–3.76; I2 = 0). Finally, there was no significant difference between cefoperazone–sulbactam and the comparators in terms of mortality rate (OR 090; 95% CI 0.38–2.16; I2 = 0) and AE risk (OR 1.07; 95% CI 0.74–1.55; I2 = 0).
Conclusions:
The clinical efficacy and safety of cefoperazone–sulbactam were similar to those of alternative antibiotics in the treatment of intra-abdominal infections. Therefore, cefoperazone–sulbactam could be recommended as an effective and safe antibiotic for treating intra-abdominal infections.
Intra-abdominal infections are severe infections associated with multiple organ dysfunctions and a high mortality rate, 23–38% in critically ill patients [1–3]. Besides timely and adequate source control, treatment with appropriate antimicrobial agents is important for the management of intra-abdominal infections. In this era of rapidly increasing multi–drug-resistant organisms, several antibiotic-resistant bacteria, such as extended-spectrum β-lactamase (ESBL)-producing and carbapenem-resistant Enterobacteriaceae members, have been reported to cause intra-abdominal infections [4–8]. An ineffective or otherwise inadequate antimicrobial regimen is one of the variables strongly associated with unfavorable outcomes [9], and initial broad-spectrum antibiotics are recommended for patients with severe intra-abdominal infections [10–13].
Cefoperazone–sulbactam is a combination of a third-generation cephalosporin and β-lactamase inhibitor, which exhibits potent in vitro activity against commonly encountered gram-positive bacteria such as Streptococcus spp. and methicillin-susceptible Staphylococcus aureus; gram-negative bacteria such as Escherichia coli, Enterobacter cloacae, and Klebsiella pneumoniae; and several anaerobes [14–19]. With the addition of sulbactam, cefoperazone shows enhanced activity and potency in vitro against ESBL-producing E. coli and K. pneumoniae, carbapenem-resistant Enterobacteriaceae, and carbapenem-resistant Acinetobacter baumannii [20,21]. In addition, the action of cefoperazone–sulbactam is not affected by a greater inoculum size of ESBL-producing E. coli and K. pneumoniae [22].
Although several studies [23–25]. have investigated the clinical efficacy of cefoperazone–sulbactam in the treatment of intra-abdominal infections, most of them had a small number of patients; and their findings cannot be generalized. Therefore, we conducted this systematic review and meta-analysis to assess the clinical efficacy and safety of cefoperazone–sulbactam in comparison with alternative antibiotics in the treatment of intra-abdominal infections.
Patients and Methods
Study search and selection
We searched the PubMed, Cochrane, Web of Science, Ovid Medline, and CKNI databases up to November 25, 2020, using the search terms were used: “cefoperazone,” “sulbactam,” and “infect.” Only clinical studies that compared the clinical efficacy and safety of cefoperazone–sulbactam with those of alternative antimicrobial agents in the treatment of patients with intra-abdominal infections were included. The reference list of the relevant articles also was searched manually to identify additional eligible articles. We did not apply language limitations. We performed this systematic review in accordance with the preferred reporting items for systematic reviews and meta-analysis guidelines [26].
Study selection and data extraction
Three investigators (SHL, CMC, and SPC) screened and reviewed each study independently. Studies were included if they met the following criteria: (1) Patients with intra-abdominal infection; (2) intervention with cefoperazone–sulbactam; (3) comparison with other antibiotic regimens; and (4) reported outcomes of efficacy, including clinical and microbiologic responses. The exclusion criteria were: (1) Case reports; (2) single-arm studies; (3) studies that did not report outcomes for cefoperazone–sulbactam in the treatment of intra-abdominal infections; (4) studies that did not compare the outcomes for cefoperazone–sulbactam with those for other antibiotic regimens; (5) pharmacokinetic studies; and (6) in vitro studies. If there were any disagreements, two other investigators (LCL and CCL) were consulted. For each included study, we extracted the following data: Year of publication, study design, antimicrobial regimens, clinical and microbiologic outcomes, and adverse event (AE) risk.
Outcome measurement
The primary outcomes were clinical efficacy, clinical cure, and clinical failure rates. The secondary outcomes were microbiologic eradication rate, mortality rate, and AE risk. Clinical efficacy included clinical cure and improvement. Clinical cure was defined as follows: If the infections were treated only with the assigned study antibiotics and resolved without relapse and if no other antibiotic was administered during the follow-up period. Patients whose primary infection was controlled but who presented persisting clinical disability or developed superinfections were considered to have exhibited clinical improvement. Clinical failure was defined as the need to: (1) Include additional antimicrobial agents to control intra-abdominal infection, (2) drain an abscess or a incision infection surgically, or (3) death related to infection. Microbiologic eradication was defined as the elimination of the source of infection with no further material left to culture or lack of growth in cultures of residual drainage.
Data analysis
The risk of bias in the randomized controlled trials (RCTs) and retrospective observational studies included was assessed using the Cochrane risk-of-bias tool [27] and Newcastle-Ottawa Scale [28]. Statistical analyses were performed using Review Manager version 5.3 (The Nordic Cochrane Center, Copenhagen, Denmark) with the random-effects model. The degree of heterogeneity was evaluated using the Q statistic generated from the χ2 test. The proportion of statistical heterogeneity was assessed using the I2 measure. Heterogeneity was defined as significant when the p value was <0.1 or I2 was >50%. The pooled OR and 95% CI were calculated, and results with a p value of <0.05 were considered statistically significant.
Results
Study selection
The search yielded a total of 2,974 studies, of which 614 were excluded as duplicates. Moreover, 2,329 studies were found to be irrelevant after the title and abstract were screened, and 19 studies were excluded after the full text was examined. Finally, 12 studies (23–25,29–37) were included in this meta-analysis (Fig. 1).
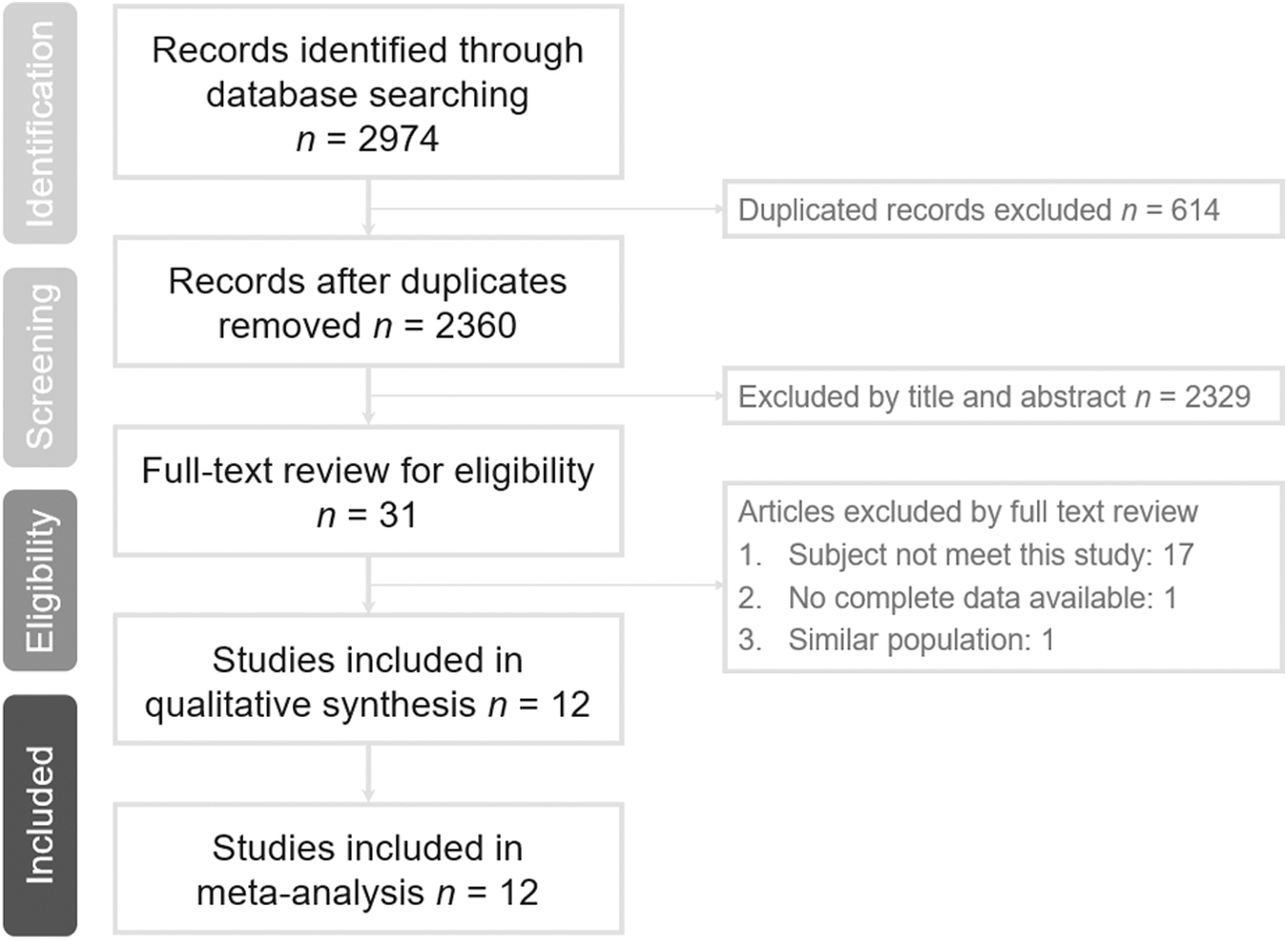
Flow chart of study selection.
Study characteristics
The 12 studies comprised 10 RCTs (23–25,29–34,37) and two retrospective studies [35,36] (Table 1). Five of the studies were multicenter [23–25,29,37], the remaining seven being single center [30–36]. Eight studies [30–37] were conducted in China, two in the USA [24,25], and one each in Japan [23] and India [29]. The study population and the comparative agents differed among the studies (Table 2). Overall, 1,674 patients were included, of whom 781 received cefoperazone–sulbactam.
Characteristics of Included Studies
RCT = randomized controlled trial; SBP = spontaneous biliary peritonitis.
Summary of Diagnoses in Each Study
Clinical efficacy
Overall, the clinical efficacy rate of cefoperazone–sulbactam and comparators was 87.7% and 81.7%, respectively; and cefoperazone–sulbactam was associated with a higher clinical effective rate than the control drugs (OR 1.98; 95% CI 1.31–3.00; I2 = 36%; Fig. 2). The superiority of cefoperazone–sulbactam over the comparator remained unchanged in the pooled analysis of the 10 RCTs (OR 1.89; 95% CI 1.18–3.03; I2 = 45%). The results of the leave-one-out sensitivity analysis showed that the magnitude of association of cefoperazone–sulbactam with clinical efficacy was not influenced by individual studies.
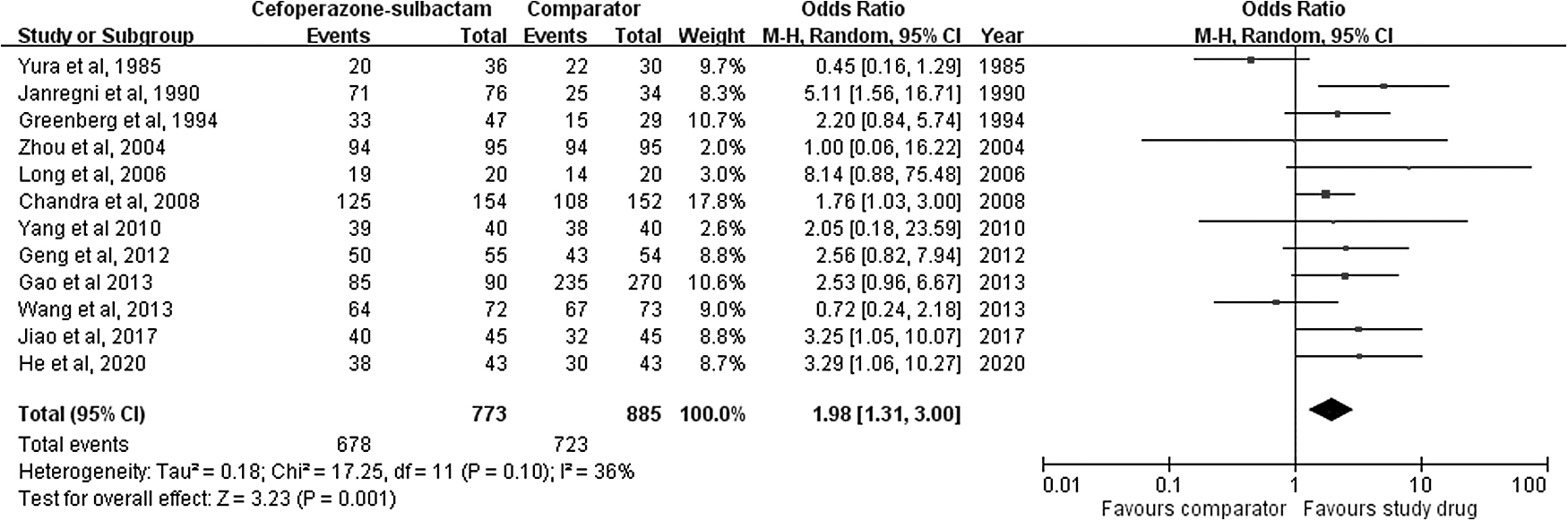
Forest plot of clinical effectiveness rate of cefoperazone–sulbactam and comparators in treatment of intra-abdominal infection.
In the subgroup analysis, cefoperazone–sulbactam presented a higher clinical efficacy rate than the comparators in the eight studies conducted in China (OR 2.26; 95% CI 1.43–3.59; I2 = 0). Although cefoperazone–sulbactam presented a numerically higher clinical effectiveness rate than the comparator in the pooled analysis of the four studies outside China (79.6% versus 69.3%), the difference was not statistically significant (OR 1.70; 95% CI 0.76–3.81; I2 = 69%). In the pooled analysis of the studies published before 2000, the clinical efficacy rate of cefoperazone–sulbactam was comparable to that of control drugs (OR, 1.69; 95% CI, 0.44–6.52; I2 = 79%). In the pooled analysis of the studies after 2000, the clinical efficacy rate of cefoperazone–sulbactam was higher than that of control drugs (OR 2.03; 95% CI 1.43–2.88; I2 = 0).
According to the site of infections, we found that the clinical efficacy rate of cefoperazone–sulbactam was similar to that of the control group in the patients with biliary tract infection (OR 1.76; 95% CI 0.83–3.75; I2 = 31%), spontaneous bacterial infections (OR 3.97; 95% CI 1.44–10.93; I2 = 0), or other intra-abdominal infections (OR 1.82; 95% CI 0.99–3.35; I2 = 51%). Moreover, the clinical efficacy rate of cefoperazone–sulbactam was comparable to that of third-generation cephalosporin-containing regimens in the subgroup of patients with biliary tract infection (OR 1.58; 95% CI 0.86–2.90; I2 = 38%).
Eleven studies reported the clinical failure rate, and the pooled analysis showed that cefoperazone–sulbactam was associated with a lower rate than the comparators (OR 0.40; 95% CI 0.28–0.57; I2 = 0; Fig. 3). This result did not change in the leave-one-out sensitivity analysis. Moreover, the relatively lower clinical failure rate of cefoperazone–sulbactam was observed in the subgroup analysis of RCTs only (OR 0.42; 95% CI 0.25–0.69; I2 = 12%). Similar findings were noted in the pooled analysis of the studies in China (OR 0.42; 95% CI 0.25–0.70; I2 = 7%) and outside China (OR 0.38; 95% CI 0.24–0.63; I2 = 0).

Forest plot of clinical failure rate in cefoperazone–sulbactam and comparators in treatment of intra-abdominal infection.
Nine studies [23–25,30–32,34–36] reported a clinical cure rate, and their analysis showed that cefoperazone–sulbactam was associated with a higher rate than the comparators (OR 1.54; 95% CI 1.17–2.03; I2 = 0; Fig. 4). This finding did not change in the leave-one-out sensitivity analysis. In the subgroup analysis of seven RCTs [23–25,30–32,36], a higher clinical cure rate was observed in the cefoperazone–sulbactam group than that in the control group (OR 1.78; 95% CI 1.22–2.59; I2 = 7%). In addition, the higher clinical cure rate of cefoperazone–sulbactam than of the comparators did not change in the subgroup analysis of six studies [30–32,34,36] conducted in China (OR 1.37; 95% CI 1.00–1.87; I2 = 0) or the three studies [23,24,31] conducted outside China (OR 2.25; 95% CI 1.09–4.62; I2 = 34%).
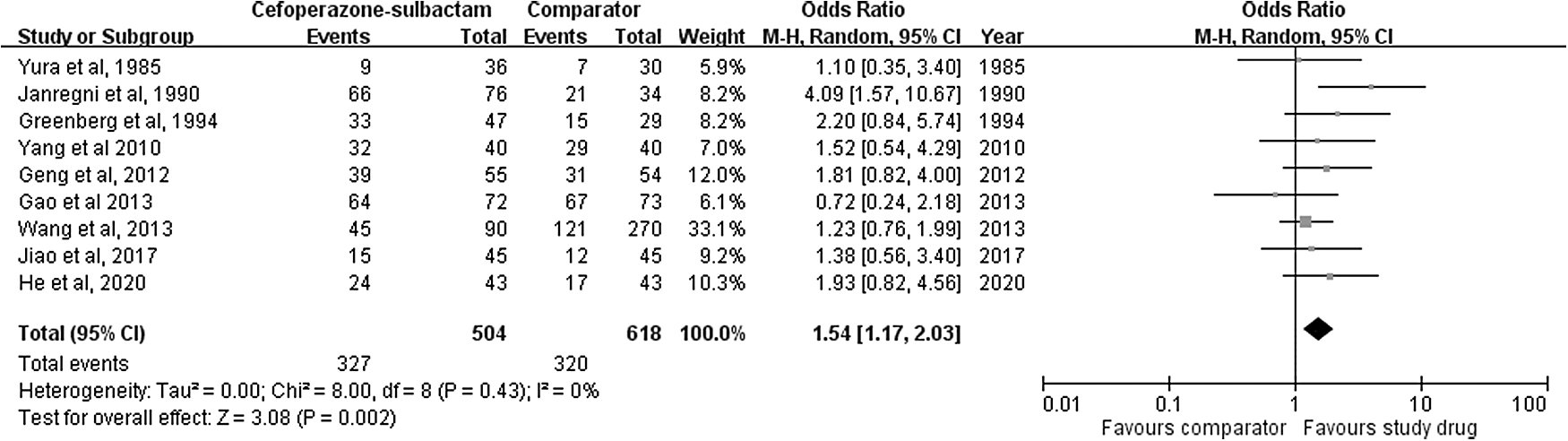
Forest plot of clinical cure rate of cefoperazone–sulbactam and comparators in treatment of intra-abdominal infection.
Secondary outcomes
Eight studies [23–25,29–32,36] reported the microbiologic eradication rate, and their pooled analysis showed that cefoperazone–sulbactam was associated with a higher eradication rate than the comparators (OR 2.54; 95% CI 1.72–3.76; I2 = 0; Fig. 5). The pooled analysis of three studies [25,29,33] that reported the mortality rate showed no significant difference in deaths between cefoperazone–sulbactam and the comparators (OR 90; 95% CI 0.38–2.16; I2 = 0). Finally, there was no significant difference in the risk of AEs between cefoperazone–sulbactam and the comparator in the pooled analysis of seven studies [29–31,33,34,36,37] (OR 1.07; 95% CI 0.74–1.55; I2 = 0; Fig. 6).
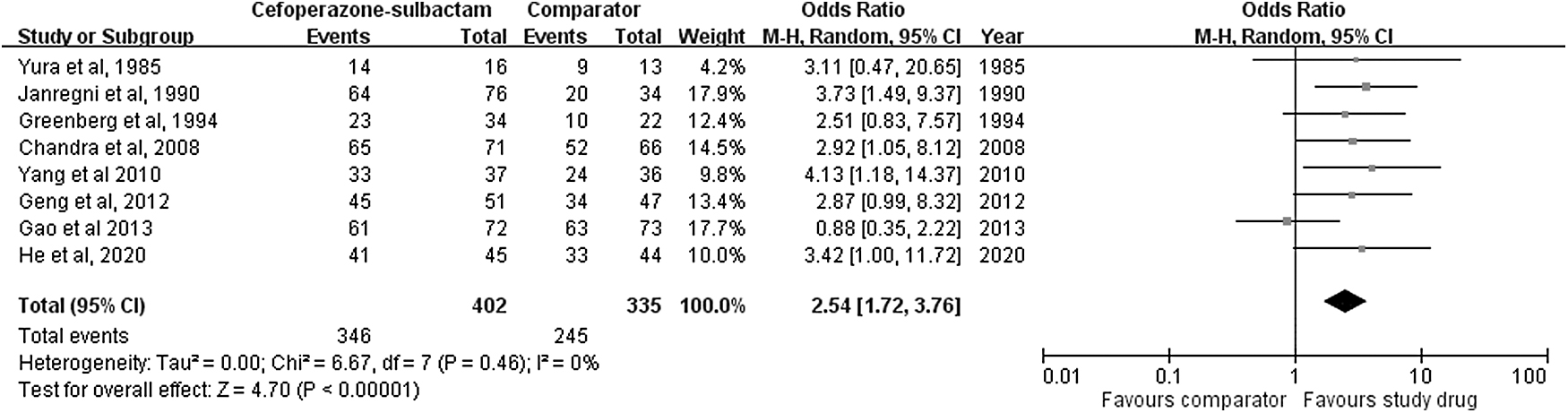
Forest plot of microbiologic eradication rate of cefoperazone–sulbactam and comparators in treatment of intra-abdominal infection.
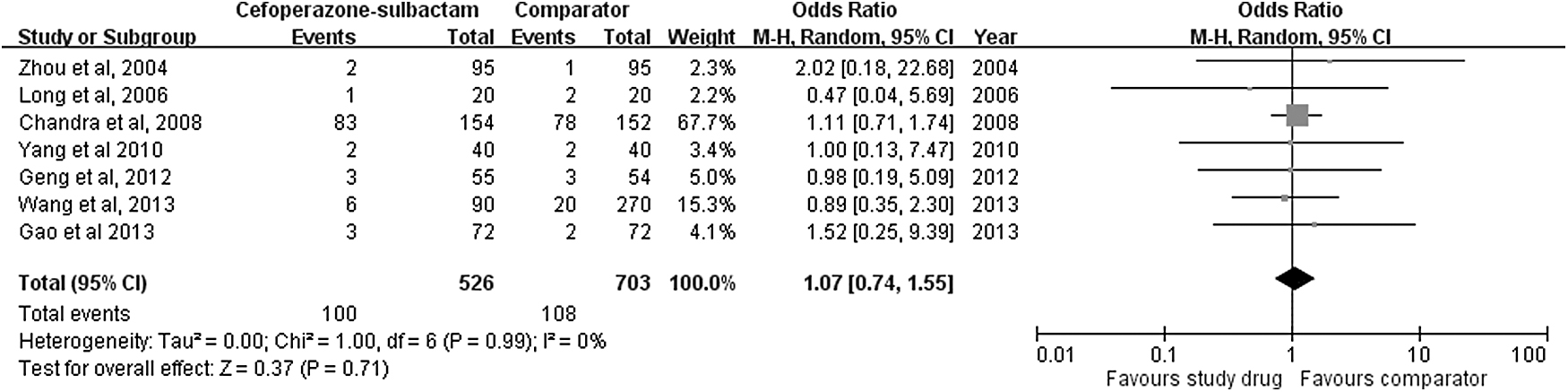
Forest plot of risk of adverse event with cefoperazone–sulbactam and comparators in treatment of intra-abdominal infection.
Discussion
In this meta-analysis of 12 clinical studies involving 1,674 patients, we investigated the clinical efficacy and safety of cefoperazone–sulbactam in the treatment of intra-abdominal infections. Most importantly, we found that the clinical efficacy of cefoperazone–sulbactam was comparable to that of alternative antibiotics, and this finding was supported by the following evidence.
First, cefoperazone–sulbactam was associated with a higher clinical efficacy rate than the comparators in the pooled analysis of the 12 studies. Moreover, the higher clinical efficacy rate of cefoperazone–sulbactam than that of the comparators also was demonstrated in the sensitivity test, and the subgroup analysis of the 10 RCTs and 8 studies in China. An exception was the finding of the subgroup analysis of the four studies conducted outside China, in which no significant difference was observed between cefoperazone–sulbactam and the comparators.
Second, the clinical efficacy rate of cefoperazone–sulbactam remained comparable to that of the control group in the further subgroup analysis according to study year (before and after 2000), source of infection, and commonly used antibiotic regimen containing a third-generation cephalosporin.
Third, the clinical failure rate of cefoperazone–sulbactam was similar to that of the comparator in the pooled analysis of all the 12 studies and the subgroup analysis. Fourth, we found that cefoperazone–sulbactam was associated with a higher clinical cure rate than the comparator. Finally, cefoperazone–sulbactam was associated with a mortality rate similar to that of the comparators.
In summary, all these findings indicate that cefoperazone–sulbactam was as effective as alternative antibiotics in the treatment of intra-abdominal infections; and as a guideline, cefoperazone–sulbactam could be recommended as a therapeutic option for intra-abdominal infections [13].
In this study, we compared the microbiologic eradication rate of cefoperazone–sulbactam and that of the comparator in the treatment of intra-abdominal infections using meta-analysis. We found that cefoperazone–sulbactam was associated with a significantly higher eradication rate than the comparator. This is supported by the findings of several studies [5,6,38], which demonstrated the potency of cefoperazone–sulbactam against commonly encountered pathogens causing intra-abdominal infections.
Although this study did not assess the utility of cefoperazone–sulbactam against ESBL-producing organisms, some in vitro studies (20,38) have demonstrated its potent activity against such bacteria. Lai et al. [20] found that 75.9% and 91.4% of ESBL organisms—K. pneumoniae and E. coli—remained susceptible to cefoperazone–sulbactam in a 1:1 ratio. Shi et al. showed that more than 50% of E. coli and K. pneumoniae strains were resistant to the third-generation cephalosporins or quinolones, but cefoperazone–sulbactam exhibited potency in vitro against these two common pathogens, irrespective of the presence of ESBL genes [38]. Therefore, our findings indicate that cefoperazone–sulbactam could be used to treat intra-abdominal infections.
Finally, we assessed the safety of cefoperazone–sulbactam for treating patients with intra-abdominal infections. We found that cefoperazone–sulbactam did not increase the risk of AEs compared with that of alternative antibiotics. Therefore, our findings suggest that cefoperazone could be a safe antibiotic for treating patients with intra-abdominal infections.
The meta-analysis conducted by us has its strength in the large number of patients, and all analyses including subgroup studies showed consistent results. However, this study had some limitations. First, the comparative agents were mostly third-generation cephalosporins, and no other β-lactam/β-lactamase inhibitor combinations, such as piperacillin–tazobactam, were compared. Second, we did not assess the association between clinical/microbiologic responses and individual antibiotic-resistant bacteria, such as ESBL organisms. Thus, we could not determine the effect of cefoperazone–sulbactam on the outcome of intra-abdominal infections caused by multi–drug-resistant organisms. Further studies are warranted to clarify these issues. Third, in addition to antibiotic treatment, source control for complicated intra-abdominal infection is another important treatment option. However, this study did not assess the confounding effect of source control. Finally, a short course of antibiotic treatment with adequate source control has been promoted after the STOP IT trial [39]; however, the studies included in the meta-analysis did not apply short-course regimens. Further study is warranted to investigate these issues.
In conclusion, the clinical efficacy and safety of cefoperazone–sulbactam were comparable to those of alternative antibiotics in the treatment of intra-abdominal infections. Therefore, cefoperazone–sulbactam could be recommended as an effective and safe antibiotic for treating these infections.
Funding Information
No financial support was received for the writing of this manuscript.
Author Disclosure Statement
The authors have no conflicts of interest regarding this manuscript.