
Abstract
Background:
Most incisional surgical site infections (ISSI) are now diagnosed after discharge from hospital. In this context, it is important to document the impact ISSI has on our patients.
Patients and Methods:
Our surgical department sent a validated questionnaire to patients after they had been discharged. This documented incision problems, the 36-Item Short Form Health (SF-36) qualify of life questionnaire, and a patient satisfaction survey (PSS). We retrospectively reviewed records for 115 patients with an ISSI and 115 matched controls with no documented complications. Patient demographics and outcomes were collected. Differences in physical component summary (PCS) score and mental component summary (MCS) score and the PSS score were compared.
Results:
A majority (87%) of ISSIs were diagnosed after discharge from hospital. There were no differences in demographics, the American Society of Anaesthesiologists grade, or length of stay (LOS) between groups. Two months after surgery, ISSI was associated with lower post-operative SF-36 scores. The PCS was 42.9 (95% confidence interval [CI], 41.3–44.8) for ISSI cases and 47.0 (95% CI, 45.1–48.7) for controls (p ≤ 0.001). The MCS was 45.8 (95% CI, 43.7–47.9) and 50.2 (95% CI, 48.0–52.3), respectively (p = 0.01). Patients had less vitality, increased pain, and a reduction in physical activities and roles. The PSS score was 82.5 (95% CI, 79.6–85.4) in the control group and 74.1 (95% CI, 71.1–77.0) in the ISSI group (p < 0.001). Patients with ISSI reported worse satisfaction ratings with the quality of information received (p = 0.005) and their satisfaction with surgery (p < 0.001).
Conclusions:
Incisional surgical site infection was correlated with lower quality of life and PSS scores for up to two months after surgery. Prospective studies with pre-operative and post-operative quality of life are required to confirm causality.
Surgical site infection (SSI) is one of the most common causes of nosocomial infection. Surgical site infection includes superficial incisional SSI, deep incisional SSI, and space SSI [1]. Depending on the surgical procedure and how SSI is monitored, these occur in up to 20% of patients after general surgery [2–6]. Historical studies of SSI diagnosed in hospital report a two-fold increase in mortality, greater than five day increase in length of stay (LOS), a five-fold increase in rates of re-admission, and mean increase in costs greater than $5,000 [7,8]. Whereas a majority of costs are related to an increase length of hospital stay [7], there are also indirect and social costs, including loss of productivity and income [9].
The impact of incisional surgical site infection (ISSI) is more difficult to define because ISSI and space SSI are often reported as one entity [1–8]. Abdominal space infections, usually caused by enteric organisms, differ in pathophysiology and consequences from ISSI [9]. Based on first principles, it is expected that the morbidity of space SSI would be greater than deep ISSI, which would be greater than superficial ISSI. In a study of 2,832 SSI diagnosed in a range of surgical specialities [7], superficial ISSI, deep ISSI, and space SSI accounted for approximately 70%, 20%, and 10% of SSI, respectively. Deep ISSI and space SSI were combined and compared with superficial ISSI. The cost and increase in LOS were approximately one-half in the superficial ISSI group, with no increase in mortality compared with a two-fold increase in the combined group. The literature comparing deep and superficial ISSI confirm a greater cost and LOS for deep ISSI [7,11,12]. Additionally, reports that focus on ISSI have demonstrated an increase in LOS [7,12–15] and re-admissions [2,11]. In our institution, the mean increase in LOS because of ISSI after abdominal surgery was 4.4 days [16]. The cost attributable to ISSI in the United Kingdom ranged from £14 to £6,161 in one study [7], with costs being higher (£10,523) after colorectal surgery [15]. The majority of ISSI costs were also because of an increased LOS [7,11,16–19].
Historical literature on the impact of ISSI usually report on ISSI diagnosed in hospital [13,14,19]. This highlights a major difference compared with contemporary clinical practice, in which the majority of ISSIs are diagnosed after discharge from hospital [20,21], with only 50%–80% of ISSIs being identified by the sixteenth post-operative day [22–24]. Because ISSIs identified in hospital are more severe than those diagnosed after discharge [4], historical data on the impact of ISSI are likely to be worse than what is currently experienced in many patients with ISSI. Another challenge with ISSIs diagnosed after discharge is that the surgeon may not directly manage these ISSIs, which may contribute to underestimating the rate and morbidity of ISSI [3,4]. This may include pain, time off work, antibiotic agents, dressing changes, loss of income, reduced work productivity, increased stress [11], and subsequent incisional hernia formation.
Another way to measure the impact of ISSI is to assess patient satisfaction and quality of life (QOL). Few studies have investigated QOL outcomes associated with ISSI. A 2017 systematic review [11] identified only one randomized controlled trial (RCT) assessing QOL. This found a reduction in QOL scores (EQ-5D) 30 days after surgery in patients with an ISSI [25]. There is no evidence that ISSI reduces long-term QOL [26]. With respect to patient satisfaction, a small series of structured interviews indicated a reduced satisfaction because of uncertainty, anxiety, lack of support from healthcare providers, and inability to manage an ISSI at home [27]. In our institution, we have developed and validated a post-discharge questionnaire, incorporating the 36-Item Short Form Health (SF-36) QOL survey [28], a patient satisfaction score (PSS), and questions to identify complications experienced after discharge from hospital [29]. When assessing all complications after general surgery, 80% of patients with complications had these diagnosed after discharge from hospital. These were associated with a statistically significant reduction in patient satisfaction and QOL [3]. Using this questionnaire, we wanted to explore what impact ISSI had on our patient's recovery from surgery, QOL, and their overall satisfaction with their medical management.
Patients and Methods
This is a retrospective review of prospectively collected data. All patients in the study underwent surgical procedures at Dunedin Public Hospital and completed a questionnaire. Routine post-operative management included documentation of outcomes using the Otago Clinical Audit (OCA), a structured telephone interview, and a post-discharge postal questionnaire. The OCA [30] is an established audit system capturing all surgical admissions and re-admissions. This documents patient demographics, American Society of Anaesthesiologists (ASA) grade, operation details, and complications identified at discharge. A senior nurse performed a structured telephone interview one to two weeks after discharge, including questions about post-operative problems. Details of the nature of any incision problems including their commencement, duration, and management were asked. The validated postal questionnaire was sent approximately one month after discharge. This included the same questions assessing post-operative incision problems, the SF-36 QOL survey, and the patient satisfaction score (PSS). The PSS is based around eight questions that asks patients to rank their experience on five-point Likert scales (Fig. 1). The PSS was derived from the summation of the scores from the eight Likert scales (each with a score range of 0–4) to give a total score out of 32 that was then converted to a percentage. Electronic patient records available on the hospital's patient management software, including outpatient clinic notes, emergency department presentations, and discharge summaries were utilized to answer queries.
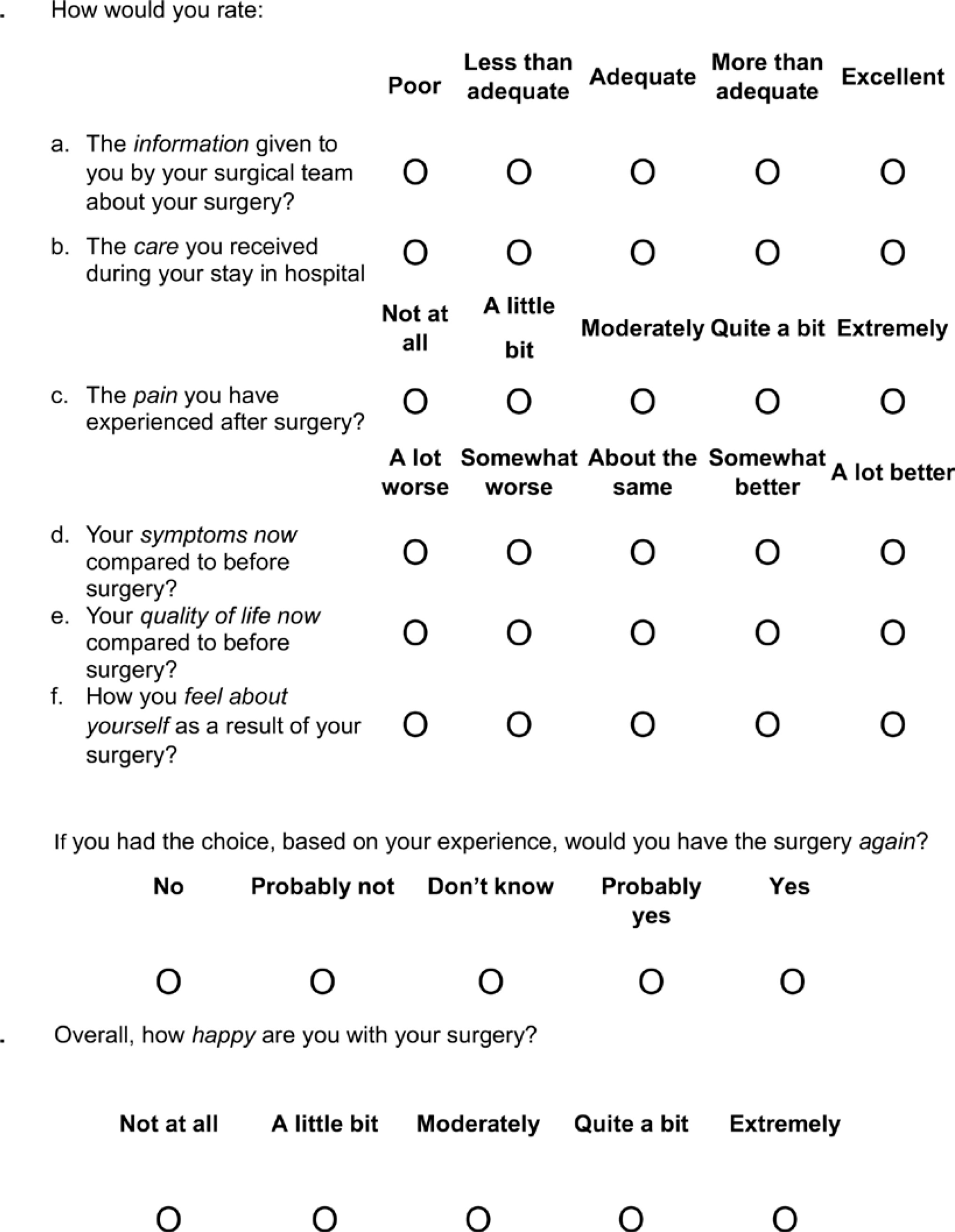
Patient satisfaction survey.
Identification of an ISSI was primarily from the patient's perspective, with patients self-reporting “wound infection” at the time of the telephone interview or questionnaire. Confirmation of ISSI required a questionnaire description consistent with purulent discharge, cellulitis, being prescribed antibiotic agents for an incision problem, and, to a lesser degree, incision breakdown associated with infection. Superficial dehiscence without infection, seroma, or hematomas did not qualify as ISSI. Because we were interested in documenting the impact of ISSI, patients who identified other post-operative complications were excluded. For example, if a patient reported both an incision infection and a pain problem, they did not qualify unless the pain was centred in the surgical incision. Controls were patients with no self-reported or documented evidence of complications on their OCA, telephone interview, questionnaire, or electronic medical records. Controls were matched to ISSI patients for gender, age within 10 years, and comparable operation.
Potential patients were identified from boxes containing folders of validated postal questionnaires. These were not stored in sequential order. To avoid selection bias, consecutive boxes were opened, and the folders in each were consecutively assessed by two surgical registrars (C.F., A.H.). Incomplete questionnaires were excluded. For patients who met the above criteria for an ISSI or a control, the OCA and patient records were used to confirm if an ISSI had been diagnosed before discharge from hospital and to check if any other complications had been identified. Data collection included patient demographics, surgery details, the ASA grade, discharge date, details of ISSI, SF-36 physical component summary (PCS) and mental component summary (MCS) scores, and the patient satisfaction score (PSS). This study was approval by the University of Otago Human Ethics Committee (Health), ethics number HD16/065, and was conducted in accordance with the Declaration of Helsinki [31].
Demographic data were summarized with appropriate statistics, including mean, standard deviation, and 95% confidence intervals for normally distributed continuous variables, median, and interquartile range for other continuous variables. Differences between ISSI and control groups for QOL and PSS scores were compared using the Student t-test. Differences in individual patient satisfaction questions were compared between groups with the Cochran-Armitage test for trends. Separate regression analyses, using general linear models, were performed with the dependent variable being either the PCS, MCS, or the PSS. Independent variables in the models included ASA (1–3) as a measure of the patient's comorbidities, age (continuous variable), and ISSI (yes, no). Data were analyzed with R (version 4.0.0) [32]. A sample size of 100 patients in each group was chosen to provide a reasonable volume of information about issues identified by patients relevant to ISSIs. This was greater than the number of patients required to detect statistically significant changes in the PCS and MCS of the SF-36, and in the PSS, which all required approximately 25 patients in each group.
Results
We identified 115 patients with ISSI and 115 matched controls. There were no differences in patient demographics and procedures (Table 1). The selected folders included patients having surgery between May 2009 and April 2016. Eighty-six percent of procedures were between December 2009 and September 2013. All patients had completed questionnaires and audit data, and 56.5% of patients had a documented telephone interview. The median time from surgery to completion of the questionnaire was 60 days [27] (median [interquartile range]) in the control group and 58 days [21] in the ISSI group. One hundred (87%) ISSI patients were diagnosed for the first time after discharge from hospital. The median LOS was two days in each group [5]. There was only one re-admission in the control group and two in the ISSI group.
Patient Demographics
ISSI = incisional surgical site infection; ASA = American Society of Anesthesiologists.
Quality of life
Incisional surgical site infection was associated with lower SF-36 component scores (Table 2). The mean (95% CI) PCS was 42.9 (95% confidence interval [CI], 41.3–44.8) for ISSI cases and 47.0 (95% CI, 45.1–48.7) for controls (p ≤ 0.001). The mean (95% CI) MCS was 45.8 (95% CI, 43.7–47.9) for ISSI cases and 50.2 (95% CI, 48.0–52.3) for controls (p = 0.01). Regression analysis (Table 3) demonstrated that ISSI (p < 0.001) had a greater impact on QOL than age and ASA for both PCS and MCS. Patients with ISSI also had significantly lower scores in seven of eight SF-36 subgroups (Table 2). The greatest differences were in the Role Emotional and Role Physical subgroups. These patients had less vitality, increased pain, and an ongoing reduction in physical activity. The only SF-36 subgroup that was not different was mental health. Further details of differences are revealed by analysing the responses to individual questions (Table 4). For example, under physical functioning, patients with ISSI had a reduced ability to perform moderate activities and walk a distance of 500 m. Within the mental health subgroup, the only difference was how calm and peaceful patients felt.
Details of SF-36 Quality of Life Scores
SF-36 = 36-Item Short Form Health.
Summary of Regression Analyses
ASA = American Society of Anesthesiologists; PCS = physical component score; ISSI = incisional surgical site infection; MCS = mental component score; PSS = patient satisfaction score.
SF-36 Constituent Questions
SF-36 = 36-Item Short Form Health.
Patient satisfaction
Patients with ISSI reported worse satisfaction ratings across six of the eight questions (Fig. 2) including overall satisfaction with surgery (p < 0.001), pain experienced post-operatively (p = 0.004), quality of pre-operative information provided (p = 0.005), differences in QOL compared with before surgery (p = 0.015), how the patient feels about themselves as a result of surgery (p = 0.032), and current symptoms compared with before surgery (p = 0.04). The quality of hospital care received and how likely a patient would be to undertake surgery again were not different.
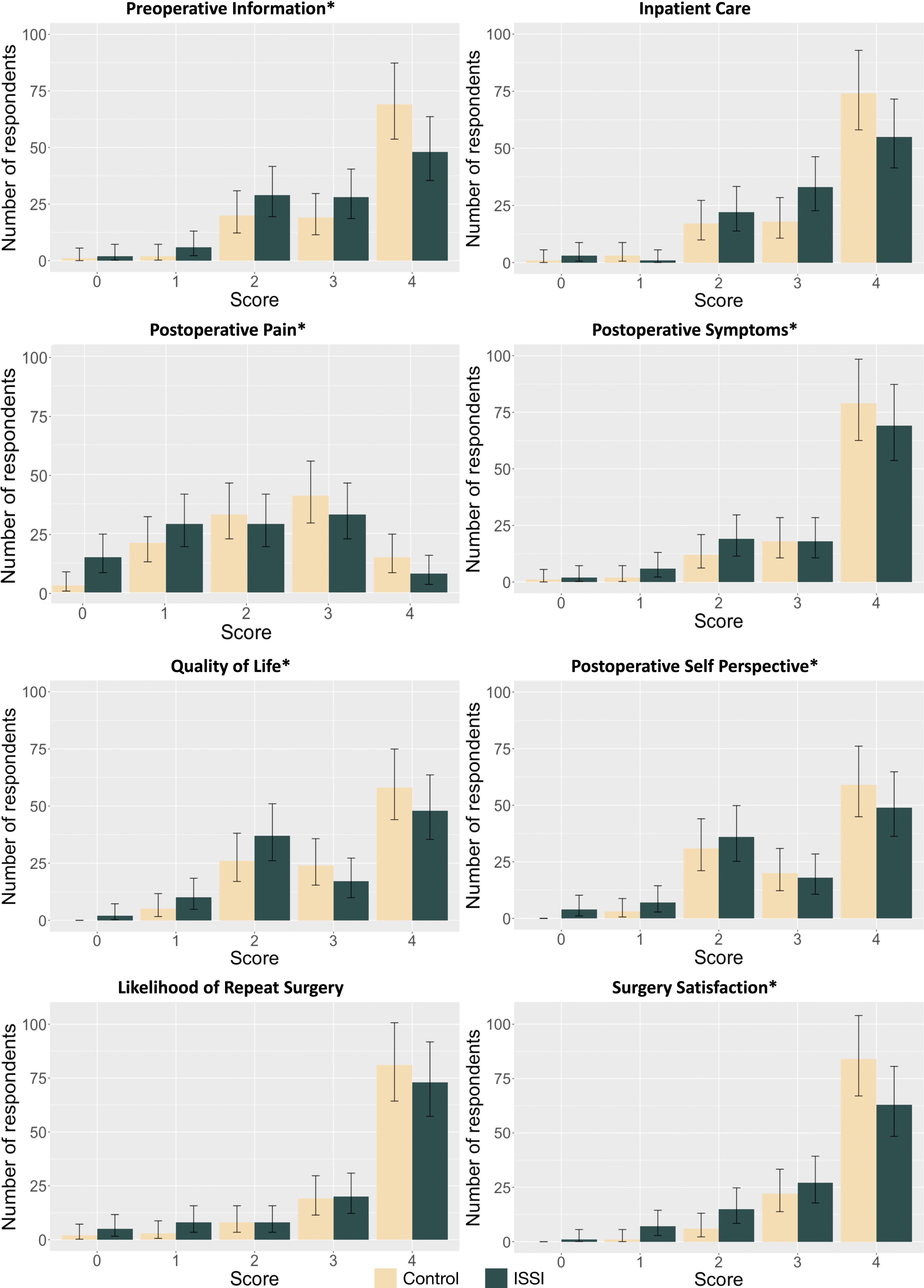
Responses to patient satisfaction survey. Green bars represent responses for patients with ISSI. Error bars show Poisson 95% confidence interval. *Denotes questions where the difference in responses were associated with Cochrane Armitage test, p < 0.05. For consistency between questions, the x-axis order for post-operative pain has been reversed compared to Figure 1, such that 0 is “extremely” and 4 is “not at all.” Color image is available online.
Examining the frequency of each response on the Likert scales (Figs. 1 and 2) provides further detail into the differences in satisfaction between groups. For example, patients developing ISSI believed the quality of pre-operative information was excellent 43% of the time, compared with 62% of controls. Post-operative pain ratings were markedly worse after ISSI, with 38% reporting “extreme” or “quite a bit” of pain compared with 22% of controls. The mean (95% CI) PSS was 82.5 (95% CI, 79.6–85.4) in the control group and 74.1 (95% CI, 71.1–77.0) in the ISSI group (p < 0.001). Regression analysis (Table 3) demonstrated that ISSI (p < 0.001) had a greater impact on the PSS than age and ASA.
Discussion
Incisional surgical site infection was associated with substantial differences in patient function, QOL, and overall satisfaction with their management, which was still present two months after surgery. In comparison to the literature, these findings were in the least severe cases of ISSI. For example, 62% of patients were having hernia, breast, gallbladder, or skin surgery; 87% of infections were diagnosed after discharge from hospital, no other complications were present; and the median LOS in both groups was two days. However, even in these patients, QOL and patient satisfaction were substantially different. This highlights the impact that even relatively minor ISSIs may have on patients. An increased awareness of ISSI morbidity, including for infections diagnosed after discharge from hospital, is therefore important for clinicians.
The impact of ISSI on QOL was seen in both the PCS and MCS scores and in seven of the eight domains of the SF-36. The greatest difference was that patients with ISSIs had difficulty performing defined roles and accomplished less. The reduction in social and physical function, reduced vitality, and increased pain had the combined effect of significantly reducing the physical and social roles (activities and responsibilities) that patients were performing two months after their surgery. Interesting findings included ongoing fatigue, reduced time spent in normal social activities, and a reduced range of physical activities, especially in the categories of vigorous and moderate activities. Fewer patients were able to walk up to 500 m and some difficulties lifting or carrying groceries were observed. The ability to perform normal activities of daily living such as climbing stairs, walking 100 m, bathing, and dressing were not different between groups. These findings highlight the benefit of using a role-based assessment to document the impact of post-operative complications. The importance of ISSI was emphasised by our regression analysis, with ISSI having a greater impact on QOL than factors normally associated with QOL, such as age and medical comorbidities as summarised by the ASA grade. This suggests that lingering symptoms and the slower recovery caused by ISSI resulted in patients achieving less and experiencing a reduced QOL two months after their surgery.
These results make an important contribution to the peri-operative QOL literature. Although some studies have made qualitative observations about the impact of SSI on both the physical and emotional aspects of QOL [26], we found only two that quantified this. The first demonstrated an 11% reduction in QOL (EQ-5D) scores 30 days after surgery in patients with an ISSI [24]. The second study, in which most patients underwent major surgery (for example with >30% cardiac surgery) showed that the reduction in the SF-12 PCS scores was similar between SSI and control groups whereas the reduction in the SF-12 MCS was greater after SSI [6]. The contribution of our study is to demonstrate and quantify the correlation between ISSI and a lower score for almost all aspects of QOL, across the full range of general surgical procedures.
The impact of ISSI on patient satisfaction was demonstrated by differences in the overall PSS and in six of the eight patient satisfaction questions. The reduction in “how happy are you with your surgery” highlights the importance of ISSI for both patients and clinicians. The lower rating about information provided by the surgical team is consistent with patients not being adequately advised about either the likelihood, or the consequences, of developing an ISSI. Other differences highlighted ongoing pain issues after an ISSI and patients with ISSI rating their overall QOL less. The similar rating for the quality of hospital care received may reflect on most ISSIs being diagnosed after discharge from hospital.
These results have important implications for patient care. In terms of communication, we need to understand the problems experienced by patients after discharge to provide correct information when consenting patients. If the clinician believes an ISSI is an uncommon problem which is easily treated, this will contribute to incorrect expectations and reduced patient satisfaction. The frequency of diagnosis of ISSI after discharge with ongoing patient symptoms highlights the importance of quality care being provided immediately after discharge from hospital. For example, both the SF-36 and patient satisfaction questionnaire highlighted problems with pain management. Optimal treatment of pain has the potential to improve QOL, as well as reducing the risk of chronic pain problems. We believe that the greater emphasis on early discharge from the hospital needs to be matched with an equal emphasis on providing better care in the community. A further implication is the importance of good post-discharge surveillance, because accurate measurement of ISSI is essential to determine the effectiveness of future interventions aimed at reducing ISSI.
There are several limitations of this study. Self-reporting of ISSI has been shown to have a positive predictive value of 71% [33]. Information reported by patients may be inaccurate because of misunderstanding or recall errors. Mitigating factors include the questionnaire asking additional questions designed to clarify the underlying nature of any incision problem and our use of medical records and the OCA. Because our study was retrospective, we were unable to contact patients to be clarify specific questions. Another weakness is that QOL data were documented after surgery, with no baseline measurement before surgery. One possibility is that a difference in QOL may have been present before surgery, rather than being caused by ISSI. At least three results suggest that the pre-operative QOL was similar in both groups. The ASA score, which categorizes physical status/comorbidities and is correlated with QOL [34–36], was not substantially different between groups (p = 0.49). The LOS and re-admission rates were the same for both groups. There were differing answers to: “How would you rate your quality of life now compared to before surgery.” This question asks about a comparison to baseline QOL. Those with an ISSI were more likely to have a lower QOL compared with their baseline QOL in comparison to the control group (p = 0.015). Because there was no adverse event in the control group and the only adverse event in the ISSI group was an ISSI, this is strong evidence that the difference in QOL after surgery was contributed to by the ISSI. Although we are not able to say that all of the differences in the SF-36 are the result of ISSI, these three reasons support ISSI being a significant reason for this difference. Last, our study design did not identify the duration of time that QOL and PSS were reduced; this would require a prospective longitudinal study.
In conclusion, this study suggests that an ISSI has an impact on the patient's journey and is correlated with a substantially lower QOL and patient satisfaction score for up to two months after surgery. This study provides, perhaps for the first time, a detailed documentation of the potential impact of ISSIs on patient's QOL after discharge from hospital. This suggests that ISSI is not a short-term, inconsequential complication for the patient, and supports further initiatives to prevent and improve managements of ISSIs. Research with pre-operative and post-operative measurements of QOL is required to confirm these results.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.