
Abstract
Background:
In trauma, direct pulmonary injury and innate immune response activation primes the lungs for acute respiratory distress syndrome (ARDS). The inflammasome-dependent release of interleukin-18 (IL-18) was recently identified as a key mediator in ARDS pathogenesis, leading us to hypothesize that plasma IL-18 is a diagnostic predictor of ARDS in severe blunt trauma.
Patients and Methods:
Secondary analysis of the Inflammation and Host Response to Injury database was performed on plasma cytokines collected within 12 hours of severe blunt trauma. Trauma-related cytokines, including IL-18, were compared between patients with and without ARDS and were evaluated for association with ARDS using regression analysis. Threshold cytokine concentrations predictive of ARDS were determined using receiver-operating curve (ROC) analysis.
Results:
Cytokine analysis of patients without ARDS patients (n = 61) compared with patients with ARDS (n = 19) demonstrated elevated plasma IL-18 concentration in ARDS and IL-18 remained correlated with ARDS on logistic regression after confounder adjustment (p = 0.008). Additionally, ROC analysis revealed IL-18 as a strong ARDS predictor (area under the curve [AUC] = 0.83), with a threshold IL-18 value of 170 pg/mL (Youden index, 0.3). Unlike in patients without ARDS, elevated IL-18 persisted in patients with ARDS during the acute injury phase (p ≤ 0.02). Other trauma-related cytokines did not correlate with ARDS.
Conclusions:
In severe blunt trauma, IL-18 is a robust predictor of ARDS and remains elevated throughout the acute injury phase. These findings support the use of IL-18 as a key ARDS biomarker, promoting early identification of trauma patients at greater risk of developing ARDS. Timely recognition of ARDS and implementation of advantageous supportive care practices may reduce trauma-related ARDS morbidity and costs.
Post-traumatic acute respiratory distress syndrome (ARDS) in traumatic injury results from both direct tissue injury and indirect insult from inflammatory mediators [1]. The pathogenesis of ARDS is associated with pulmonary contusions [2,3], severe injury (injury severity score [ISS] >25) [3,4], substantial orthopedic trauma [4], intracranial injury [5], and large volume resuscitation requirements [3,6]. The presence of ARDS denotes increased morbidity and resource utilization in trauma patients. Standardized hospital costs for post-traumatic ARDS are increased fourfold compared with patients who do not develop ARDS ($434,000 vs. $96,00, respectively) [7]. Moreover, daily hospital costs increase with worsening ARDS severity [7]. Although patient outcomes have improved through a better understanding of ARDS pathophysiology and tailored supportive care measures, reliable predictors for ARDS development in the trauma patient are limited [8].
Inflammasome-mediated interleukin-18 (IL-18) activation was recently found to be correlated with the pathogenesis of ARDS, providing a link between the innate immune response and underlying lung pathology [8,9]. Additionally, elevated plasma IL-18 in patients with ARDS may function as a potential biomarker for disease severity [8,10]. Interleukin-18, a member of the IL-1 pro-inflammatory cytokine family, is synthesized as an inactive precursor constitutively present in healthy cells. Activation is dependent on processing by the intracellular cysteine protease, caspase-1, which cleaves the precursor into its biologically mature and secreted form [11]. Functional caspase-1 requires processing and assembly, and in injured tissues this is inflammasome-mediated.
Inflammasomes, described initially as caspase-1–activating complexes [12], are intracellular multiprotein complexes that provide a platform for the oligomerization and activation of the caspase-1 cascade. In particular, the NLRP3 inflammasome has been the most studied in tissue damage. With inflammasome-mediated induction of the caspase-1 cascade, IL-18 undergoes subsequent maturation to its active proinflammatory state. Tissue injury stimulates inflammasome assembly by means of endogenous danger signaling molecules, otherwise known as damage-associated molecular patterns (DAMPs) that are released after cellular injury or stress. Damage-associated molecular patterns bind cytoplasmic pattern recognition receptors, which initiates subsequent inflammasome assembly [8,9,13,14]. Increasing evidence suggests the inflammasome-mediated response to cellular injury, with release of mature IL-18, promotes an exaggerated systemic and organ-specific proinflammatory condition, perpetuating further tissue injury [14].
In trauma, the pulmonary system is particularly vulnerable to inflammasome-mediated activation of the innate immune system given exposure to DAMPs both from direct mechanical injury and from systemic blood carrying circulating DAMPs of remotely injured tissues, together initiating the inflammatory cascade underlying ARDS [9,13]. Inflammasome-mediated elevation of plasma IL-18 mRNA transcripts and IL-18 cytokine concentrations have been noted in patients with ARDS, with studies demonstrating a correlation between ARDS severity and elevated levels of plasma IL-18 mRNA and IL-18 [8,10]. However, little is known regarding the ability of IL-18 plasma levels to predict ARDS development in trauma patients. We hypothesized that initial plasma IL-18 level, within the first 12 hours of traumatic injury, is a diagnostic predictor of ARDS in severe blunt trauma.
Patients and Methods
Data were obtained from the Inflammation and the Host Response to Injury Large Scale Collaborative Program (www.gluegrant.org) through the National Institute of General Medical Sciences (NIGMS). The program was designed as a multicenter prospective cohort study with the objective to characterize the genomic and proteomic response after blunt traumatic injury with hemorrhagic shock. Study design and criteria have been described previously in detail [15]. The Institutional Review Board of each participating center approved the original prospective study.
In brief, the study cohort consists of trauma patients ≥16 years old admitted to one of nine level 1 trauma centers over an eight-year period (2003–2010). Inclusion criteria required a blunt mechanism of injury, arrival at the trauma center within six hours of injury, elevated base deficit and/or hypotension (systolic blood pressure [SBP] <90 mm Hg, base deficit [>6 mEq/L]) within 60 minutes of arrival to the study center, red blood cell (RBC) transfusion within the first 12 hours, and an abbreviated injury score (AIS) of two or more for any body region excluding the head. Patients younger than 16 or older than 90 years of age and those with isolated traumatic brain injury (TBI) or cervical spinal cord injury were excluded.
To minimize variability in treatment practices, standard operating procedures were implemented across all study centers. These procedures included early goal-directed resuscitation, glycemic control, venous thromboembolism prophylaxis, low tidal volume ventilation, ventilator-associated pneumonia management, and restrictive transfusion guidelines [15–19].
Clinical data were validated and entered in the trauma-related trial database by trained research nurses. Data integrity was maintained via ongoing curation and external data review [20]. De-identified data were included in the Glue Grant investigator-accessible Trauma Related Database for secondary analysis.
All patients with an initial serology specimen that included plasma IL-18 levels were included in our secondary analysis. Plasma cytokine concentrations were measured using the bead array assay kit from Linco Research (St. Charles, MO). The assay panel measured the following cytokine concentrations: granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), eotaxin, IL-1A, IL-1B, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-17, IL-18, monocyte chemoattractant protein-1 (MCP-1), interferon-gamma–induced protein 10 (IP-10), interferon-gamma (IFN-γ), and tumor necrosis factor-α (TNF-α). Cytokine concentrations were measured using a quantitative sandwich enzyme-linked immunosorbent assay (ELISA) with monoclonal antibody specific to the cytokine of interest and reported in picograms per milliliter. Concentrations of the individual analytes were determined using the MiraiBio software package (Hitachi, San Francisco, CA). Per study protocol, peripheral blood samples were centrifuged at 22°C for 10 minutes within one hour of collection time. Samples were frozen (−80°C) for storage at the Inflammation and the Host Response to Injury Sample Collection and Coordination Site [15].
The main outcome of interest was development of ARDS, defined by the database as acute onset bilateral pulmonary infiltrates, partial pressure of oxygen in the alveolar gas/fraction of inspired oxygen (PaO2/FiO2) < 200 regardless of positive end-expiratory pressure and no evidence of left atrial hypertension or congestive heart failure (these criteria had to be met within a 24-hour period). Based on this definition of ARDS, patients with initial cytokine IL-18 measurements were subsequently divided into non-ARDS versus ARDS groups. Admission IL-18 cytokine concentrations (obtained within 12 hours from injury) were analyzed between groups. Interleukin-18 plasma cytokine concentrations were trended over patient hospital stay and compared between the two study groups. Additionally, because the array measured a panel of cytokines (G-CSF, GM-CSF, eotaxin, IL-1A, IL-1B, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-17, MCP-1, IP-10, IFN-γ, and TNF-α), these were also analyzed for differences between the two groups. Plasma specimens were grouped according to the following intervals from time of injury: 0–12 hours, 12–48 hours, 48–120 hours, 5–10 days, 10–20 days, 20–25 days, and >25 days. Serology samples belonging to the same patient within a given time interval were averaged.
Patient data reviewed included age, gender, mechanism of injury, body mass index, time from injury to admission and specimen collection, injury severity score (ISS), Acute Physiology And Chronic Health Evaluation (APACHE) II score, admission base deficit and lactate, admission white blood cell count (WBC), total 12-hour crystalloid infusion volume, total 12-hour blood infusion volume, major procedure requirement, pulmonary injury (International Classification of Diseases-9 codes 861.2-861.3), ventilator days, intensive care unit (ICU) and hospital length of stay (LOS), tracheostomy requirement, nosocomial and surgical site infections (SSI), ventilator-associated pneumonia (VAP), and mortality.
Data analysis was conducted using the R Project for Statistical Computing (www.r-project.org). Categorical variables were compared using the χ2 test and continuous variables were compared using Student t-test and Wilcoxon rank sum tests, as applicable. Continuous data are presented as mean ± standard error (SE) or median (interquartile range [IQR]) unless noted. A p value of ≤0.05 was considered significant. Univariable logistic regression analysis was used to evaluate the impact of patient factors on the occurrence of ARDS. A p value of <0.2 for association of a covariable with the outcome of interest was used. Associated covariables were subsequently included in a multivariable regression analysis evaluating the relation of IL-18 to the outcome. Outcomes between groups were analyzed in similar fashion. Multivariable analysis was then used to develop a receiver operator curve (ROC) and critical cutoff values of IL-18 for the outcome of ARDs.
Results
A total of 80 patients met criteria for analysis. Of these, 61 did not meet criteria for ARDS diagnosis and comprised the non-ARDS group and 19 met the criteria and comprised the ARDS group. The median day from day of injury to ARDS diagnosis was day 3 (IQR 1–5 days).
As shown in Table 1, the two groups were similar in terms of age, race, and baseline BMI, but more patients with ARDS were men (31 of 61 versus 15 of 19; p = 0.04). The two groups were also similar with respect to injury characteristics on admission, pulmonary injury, ISS, emergency department lactate, base deficit, and WBC, and need for major procedure. Compared with patients without ARDS, those with ARDS had a lower Glasgow Coma Scale (GCS) on presentation (10.3 ± 0.7 vs. 7.5 ± 1.3; p = 0.04) and had a higher crystalloid volume within the first 12 hours of injury (12.2 ± 0.9 L vs. 17.9 ± 2.5 L; p = 0.009). The groups had a similar volume of blood transfused within the first 12 hours of injury (2.6 ± 0.3 L vs. 2.5 ± 0.6 L; p = 1.0).
Patient Demographics and Clinical Characteristics
Data are shown as mean (standard error) unless otherwise noted.
Diagnosis based on International Classification of Diseases-9 codes 861.2-861.3.
ARDS = acute respiratory distress syndrome; BMI = body mass index; APACHE II = Acute Physiology and Chronic Health Evaluation II; ISS = injury severity scale; IQR = interquartile range; GCS = Glasgow Coma scale; WBC = white blood cell count; RBC = red blood cell count.
Analysis of initial plasma sampled 0–12 hours from injury showed that a higher median IL-18 level was associated with the development of ARDS (125.9 pg/mL [IQR, 71.8–207.0] in non-ARDS vs. 190.9 pg/mL [IQR 109.6–449.1] in ARDS; p = 0.04). However, comparison of initial plasma cytokines G-CSF, GM-CSF, eotaxin, IL-1A, IL-1B, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-17, MCP-1, IP-10, IFN-γ, and TNF-α did not demonstrate an association with ARDS development (all p > 0.05). Mean initial plasma collection time from injury was similar for the two groups (8.3 ± 0.4 hours vs. 8.5 ± 0.7 hours; p = 0.9).
Multivariable regression accounting for age, gender, ISS, 12-hour blood and crystalloid volume, emergency department GCS, and major procedures, showed that higher initial plasma IL-18 concentration was independently associated with development of ARDS (p = 0.008). Receiver operating curve analysis indicated a threshold IL-18 level of 170 pg/mL to best predict ARDS, with an area under the curve of 0.83 (Youden index, 0.3; Fig. 1).
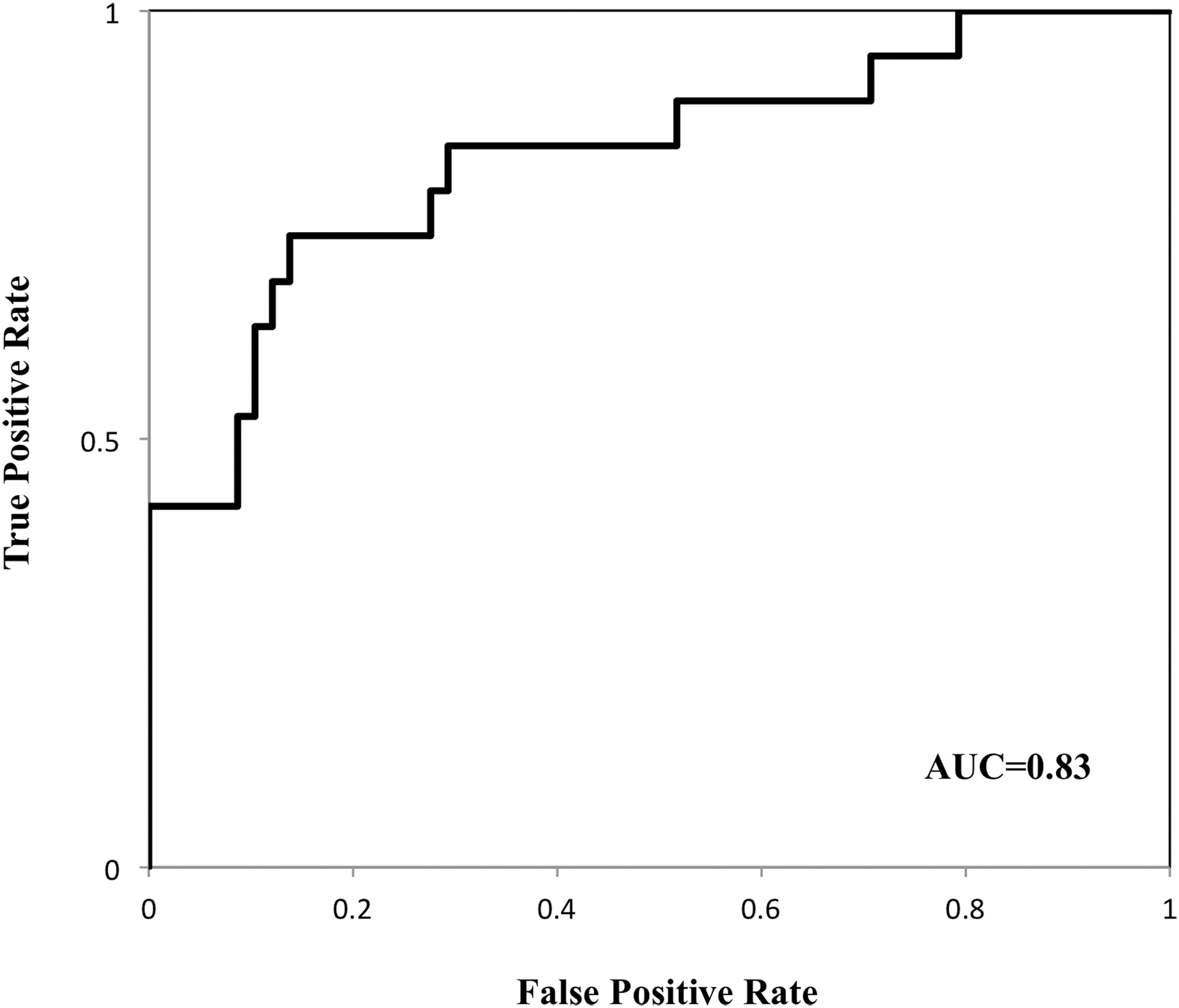
Receiver operator curve analysis of initial interleukin (IL)-18 plasma level and acute respiratory distress syndrome (ARDS) development. Area under the curve (AUC) = 0.83, with a threshold IL-18 value of 170 pg/mL (Youden index, 0.3).
In addition to being increased initially, plasma IL-18 concentration remained elevated in the patients with ARDS compared with patients without ARDS at subsequent time periods of 12–48 hours, 48–120 hours, and 5–10 days (p < 0.05; Fig. 2), after which the concentration was similar between groups.
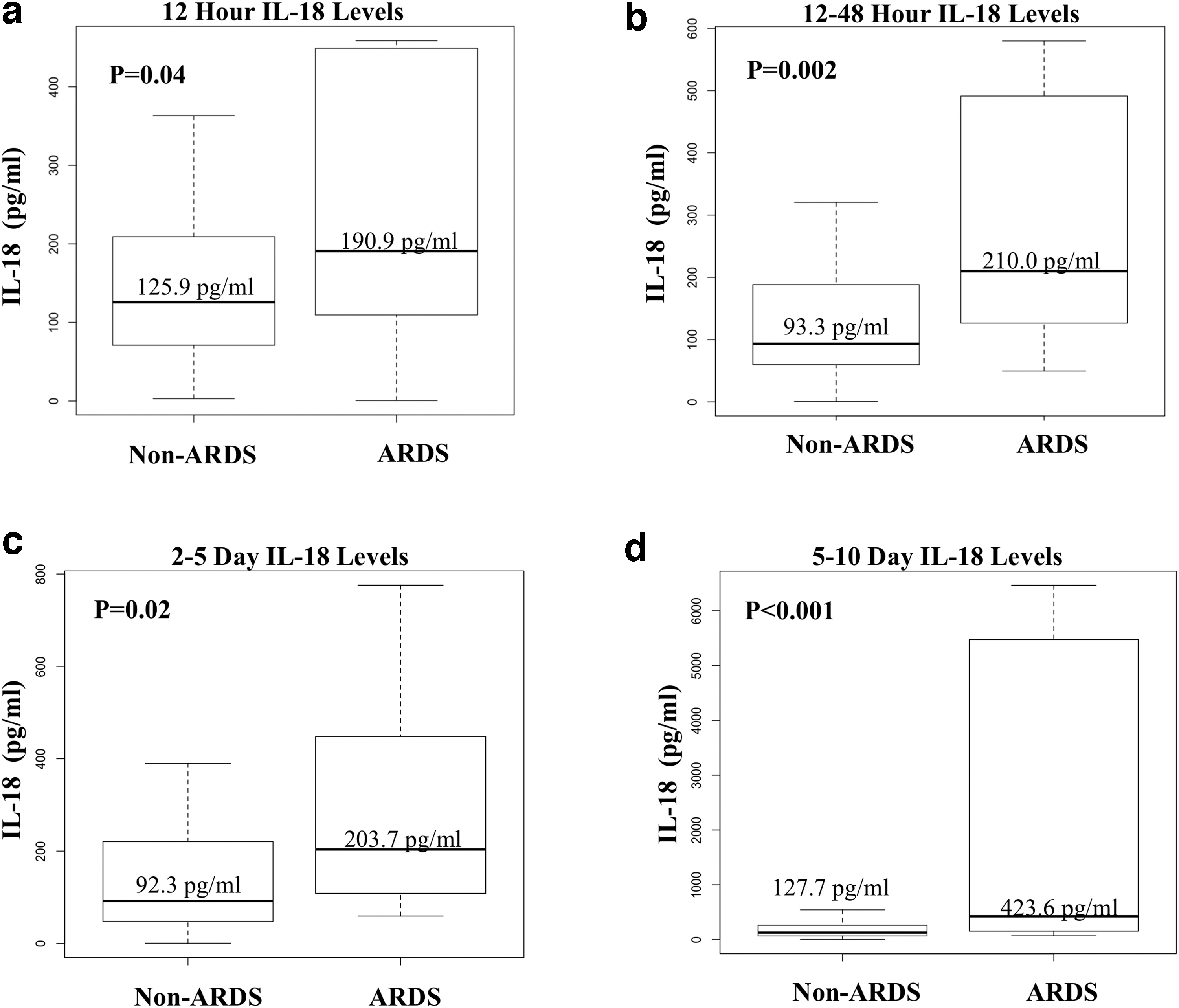
Non-acute respiratory distress syndrome (ARDS) versus ARDS median interleukin (IL)-18 cytokine levels over course of injury. Bolded segment denotes median. Upper and lower box margins denote interquartile range (IQR). Box whiskers denote minimum and maximum. IL-18 concentration in picograms per milliliter (pg/mL). (
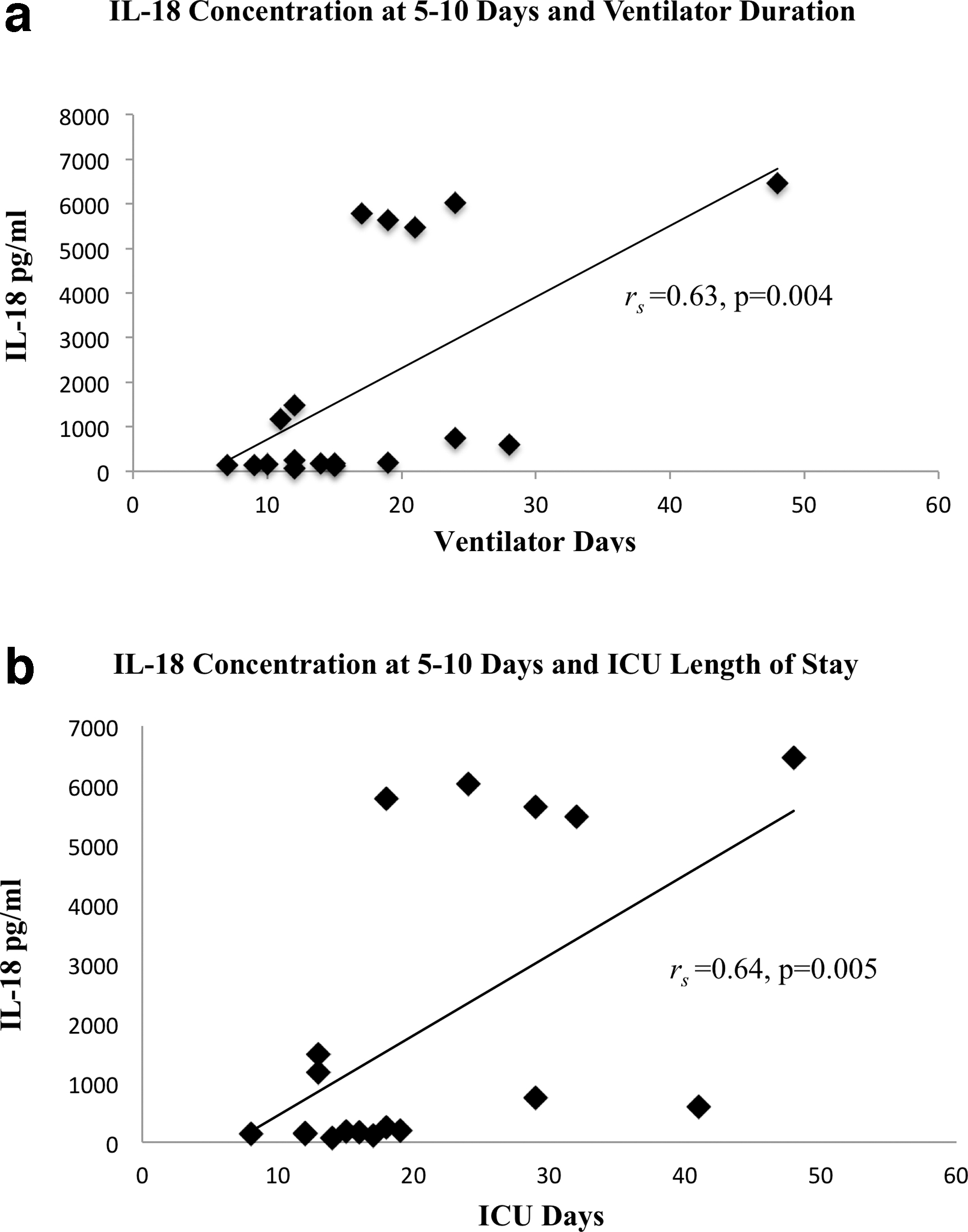
As expected, patients with ARDS had poorer outcomes than patients without ARDS, with longer ventilator days, tracheostomy requirement, development of SSIs, VAP, nosocomial infections, and hospital and ICU LOS (Table 2). Among patients with ARDS, higher IL-18 plasma concentrations at 5–10 days were correlated with longer ventilator day requirements (rs = 0.63; p = 0.004) and longer ICU LOS (rs = 0.64; p = 0.005; Fig. 3). In the ARDS group, multivariable analysis accounting for significant covariables (age, gender, ISS, emergency department GCS, 12-hour blood and crystalloid volume, and major procedures), elevated IL-18 concentrations at 5–10 days remained independently associated with longer ventilation days (p = 0.04). In patients with ARDS, elevated IL-18 concentrations at 5–10 days also remained independently associated with longer ICU LOS in in multivariable analysis accounting for significant covariables (12-hour blood and crystalloid volume) (p = 0.02). Similar analyses comparing elevated IL-18 concentrations with outcome variables for the non-ARDS group showed no correlation (p > 0.05). Elevated IL-18 plasma concentrations among patients with ARDS were not associated with the development of SSI, VAP, nosocomial infections, or longer total hospital LOS (p > 0.05).
(
Clinical Outcomes in Patients without ARDS and with ARDS
Data are shown as mean (standard error), unless otherwise noted.
ARDS = acute respiratory distress syndrome; IQR = interquartile range; SSI = surgical site infection; VAP = ventilator associated pneumonia; ICU = intensive care unit; LOS = length of stay.
Discussion
Severe blunt traumatic injury primes the lungs for the development of ARDS. Aside from direct pulmonary trauma, injured tissue releases local and systemic endogenous biomolecules, DAMPs, which rapidly activate the innate immune response propagating secondary tissue injuries remote from the initial foci of injury. Inflammasomes are highly expressed in immune, parenchymal, epithelial, and endothelial cells, and are activated by DAMP signaling. Inflammasomes are linked to this cycle of tissue damage [21] with lung endothelium being particularly sensitive to inflammatory signaling [21]. Importantly, inflammasome activation and release of mature IL-18 has been identified as a key mediator in the development of acute lung injury [8,9,13,21,22], with early elevation of IL-18 demonstrated in plasma of patients with ARDS. Therefore, we hypothesized that initial plasma IL-18 levels, within the first 12 hours of traumatic injury, are a diagnostic predictor of ARDS in the blunt trauma patient. We found that early elevation of plasma IL-18 in blunt trauma strongly predicts development of ARDS and that the threshold level of IL-18 is 170 pg/mL. Furthermore, in patients with ARDS, plasma IL-18 remains elevated throughout the acute injury phase, and its persistent elevation at 5–10 days is independently associated with increased ventilation days and ICU LOS.
The morbidity and economic cost of traumatic ARDS underscores the need for a predictive marker to identify those at increased risk. The LUNG SAFE trial, a large international observational study evaluating ARDS epidemiology, incidence, and mortality, demonstrated that ARDS remains underdiagnosed, and is commonly associated with a delay in diagnosis, particularly in milder cases [23]. Provider awareness of an earlier predictive marker could result in timely identification of disease onset and more rapid implementation of appropriate supportive care measures such as lung protective ventilation and fluid management.
Interleukin-18 may be able to fulfill this predictive function and even potentially serve as a therapeutic target. Elevated plasma IL-18 has previously been associated with acute lung pathology [8,10,13,24,25]. In mice with ventilator-induced lung injury, IL-18 expression is elevated in lung tissue and plasma. Additionally, IL-18–deficient mice demonstrate reduced pulmonary tissue injury compared with wild-type mice [8]. Furthermore, inhibition of IL-18 by IL-18 binding protein alleviates lipopolysaccharide-induced lung injury, including pulmonary edema, permeability, inflammatory infiltrate, myeloperoxidase activity, and reduces oxygen-free radicals [25]. In pulmonary injury, not only can IL-18 be readily measured as a possible serologic marker, but its inhibition may reduce inflammatory insult and promote intrinsic pathways aimed at mitigating cellular injury.
In humans, studies have focused on patients with sepsis-induced ARDS [8,10,26]. Expression of inflammasome IL-18 mRNA transcripts has been shown to be higher in medical ICU patients with sepsis-induced ARDS compared with those with isolated systemic inflammatory response syndrome [8]. Additionally, IL-18 plasma levels were elevated within 48 hours of admission and remained high in these patients. Although this study focused on sepsis-induced ARDS, the authors validated their findings using an independent cohort of trauma-induced ARDS patients with similar results [8]. Both human and animal studies continue to suggest that IL-18 is a significant mediator in early ARDS pathogenesis, lending to its promise as a predictive marker.
Our study focused solely on ARDS after blunt trauma and sought to determine whether early IL-18 plasma levels could predict the development of ARDS. Our analysis of trauma-associated cytokines, including IL-1A/B, IL-6, IL-8, IL-10, IL-12, IL-18, IFN-γ, and TNF-α, showed that only elevated plasma IL-18 levels demonstrated the unique ability to predict ARDS pathogenesis. Furthermore, IL-18 remained an independent predictor of ARDS after adjustment of possible confounding clinical factors. These results lead us to suggest that plasma IL-18 levels ≥170 pg/mL should alert clinicians to the risk of ARDS development in blunt trauma patients. In findings similar to those in prior studies, we also observed higher IL-18 levels among ARDS trauma patients up to 10 days post-injury. Taken together, our findings suggest that elevated IL-18 plasma levels may identify injured patients at heightened risk for the development of ARDS.
Importantly, we show that differences in IL-18 plasma levels after traumatic injury can rapidly be detected in patients who subsequently develop ARDS. In our study population, this appears specific to IL-18, because other inflammatory cytokines associated with ARDS pathogenesis did not predict ARDS development. A possible reason may be the mechanism by which IL-18 is synthesized and expressed in humans. Interleukin-18 is initially synthesized as an inactive precursor. Maturation to its active form requires enzymatic cleavage, predominately inflammasome-mediated. However, its precursor is constituently expressed in numerous cell types (i.e., epithelial, endothelial, monocytes) [11] and thus can be activated rapidly and released into the plasma.
In our study, surgical site and nosocomial infections were increased among patients with ARDS. As expected, the ARDS group had worse APACHE II scores, as well as longer ICU LOS and ventilator days, suggesting an increased illness severity overall. Although some consider ARDS a marker of trauma severity rather than a complication [27], increasing evidence suggests that simultaneous endothelial, coagulation, and immune dysfunction propagate ongoing tissue injury mediated through continued DAMP signaling and inflammasome activation [21]. Interleukin-18 levels were increased throughout the acute injury phase in our ARDS group. These increased levels support the current findings of persistent DAMP- and inflammasome-mediated tissue injury. The lack of correlation between degree of IL-18 elevation and infectious complications in the ARDS group we analyzed may be related to a maximum level of production beyond which further tissue injury will not contribute to significant rise in cytokine levels [8].
Although our study utilized data from a large multicenter prospective cohort study with the objective to characterize the genomic and proteomic response following severe blunt traumatic injury, it has several limitations. As a secondary analysis it was not designed or powered to definitively study the outcome of ARDS and is limited by its retrospective nature. Furthermore, only a subset of study patients had plasma cytokine measurements performed, and the timing of plasma collection was not based on ARDS development, both of which limit interpretation. Also, the study population includes only severely injured blunt trauma patients and may not be generalizable to other patient types. Despite these limitations, our study findings support an association between elevated IL-18 and ARDS pathogenesis.
Conclusions
To our knowledge this is the first study examining the ability of early plasma IL-18 to predict ARDS after severe blunt trauma. Early elevation of plasma IL-18 predicts development of ARDS in blunt trauma and remains elevated throughout the acute injury phase. As a possible biomarker for ARDS development, IL-18 may provide earlier identification of traumatically injured patients at increased risk of developing ARDS. Earlier ARDS recognition and implementation of appropriate supportive care, such as lung protective ventilation, may reduce ARDS-related morbidity in trauma.
Footnotes
Acknowledgments
We would like to thank Pamela Derish, MA, UCSF Department of Surgery, for her review of this manuscript.
This study was presented as a poster at the 78th Annual Meeting of the American Association for the Surgery of Trauma and Clinical Congress of Acute Care Surgery in Dallas, Texas, September 2019.
Funding Information
No funding was received for this article.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.