
Abstract
Background:
Cystic echinococcosis is a parasitic disease that develops in endemic areas due to the transmission of Echinococcus granulosus. The liver is the organ most affected. The most frequent symptoms include pain, palpable mass, jaundice, and fever. Diagnosis is based on epidemiologic history, examination, imaging, and serologic tests.
Patients and Methods:
We conducted a retrospective study of patients with hepatic echinococcosis diagnosed in our center. We collected data from our patients regarding personal history, cyst characteristics, surgery performed, and post-operative complications.
Results:
Sixteen patients were diagnosed with hepatic echinococcosis, 11 of whom underwent surgery. We found multiple cysts in six patients (37.5%) and a single cyst in 10 (62.5%). In 14 patients the cysts were found only in the right hepatic lobe (87.5%) and in two patients they were found in both lobes (12.5%). Segment 4 was affected in seven cases. The sizes ranged from 2.7 to 20 cm. Endoscopic retrograde cholangiopancreatography was prior to surgery in five patients. The interventions performed were partial cyst-pericystectomies in eight patients, a total cyst-pericystectomy in one case, and drains were placed in two cases of rupture. Post-operative fistulas were evident in five patients, four of which were closed. The fifth, which occurred after emergency surgery for rupture of the cyst, has maintained suppuration. The mean follow-up was 3.5 years. There was no post-operative mortality or recurrence to date.
Conclusions:
We can state that center without highly specialized hepato-biliary surgery units can assume the surgery of hydatid liver cysts excluding those with well-defined characteristics. The establishment of recommendations for the referral of patients with complex hydatid cysts may help in the optimal management of this pathology.
Cystic echinococcosis is a parasitic disease that develops in endemic areas due to the transmission of Echinococcus granulosus. Human beings are an incidental intermediate host, and the hydatid disease is found in rural areas mainly in endemic countries [1,2]. In these countries, the prevalence ranges from 5% to 10% [3]. It occurs in 95% of cases in the liver or lung in a ratio of 2:1 to 3:1 in symptomatic patients. The liver is the most affected organ, demonstrating the existence of a hepatic filter that is a determining element for the localization and the existence of a substantial percentage of patients with cysts in the liver who do not produce disease. The most frequent symptoms of patients with hydatid cysts of the liver include pain, palpable mass, jaundice, and fever. Diagnosis is based on epidemiologic history, physical examination, imaging, and serologic tests. For hepatic hydatidosis, the imaging method of choice is ultrasound, which has the highest sensitivity and specificity. It should be considered for the diagnosis of symptomatic patients, treatment control, and screening of high-risk populations for the detection of asymptomatic patients in association with serology [2–4].
Spain has traditionally been a country with a high incidence of cases but in recent years this has been reduced as a result of technological development, the abandonment of rural areas, and improvements in animal health care in rural areas. Our hospital serves a mainly urban population of 173,000 inhabitants with a low agricultural and livestock activity and therefore a low incidence of cases.
Patients and Methods
We conducted an observational and retrospective study of patients with hepatic echinococcosis diagnosed in our center since its opening with the intention of evaluating our results and establishing management guidelines for this pathology in the future. We requested the necessary permission from the medical management of our hospital center and examined medical records with the diagnoses of hydatid cyst of the liver, obtaining data on gender, age, origin, whether it presented with symptoms and what these were or whether it was a chance diagnosis. We also obtained data on the number of cysts, their size, the lobes and segments affected, whether there were calcifications in the capsule, whether the patient underwent surgery or was kept in observation (watch and wait). We obtained data on the surgical procedure performed, whether a cysto-biliary fistula was identified during the operation and the number of these, whether the operation was urgent or scheduled, whether the cyst ruptured and was operated on because of complications arising from this. We examined data on whether there were extrahepatic cysts, whether endoscopic cholangiopancreatography was performed prior to surgery, whether the patient was treated with albendazole, whether post-operative biliary fistula or other complications occurred, how they were resolved, and the follow-up time.
Regarding the surgical technique, before the operation, the surgical field was sterilized with compresses soaked in 20% hypertonic saline. The interventions performed were partial cyst-pericystectomies in eight patients, in another case a total cyst-pericystectomy, and in one case of rupture with peritonitis and instability of the patient, it was decided to wash the peritoneal cavity and the cyst and place a Kehr tube and drains. Another patient with an abscessed cyst in the lumbar region only underwent drainage while awaiting resolution of the infectious-inflammatory symptoms. In patients with unresected cyst remnants, the rest of the cyst was treated by abrasion of the intra-cystic surface with swabs soaked in hypertonic saline and subsequent fulguration of the exposed surface.
During the operation, we performed a careful inspection of the hepatic surgical bed and the residual internal surface of the cyst after its partial removal to identify fistulas intra-operatively, finding their presence in four patients, one with three and the rest with one, suturing all visible defects. Of these patients, three developed post-operative fistulas (75%). All had a good progression with conservative treatment except for one patient who required emergency re-operation for a poorly tolerated biliary leak and choleperitoneum with emergency right hepatectomy.
Results
From January 1, 2008 to December 31, 2020, 16 patients were diagnosed with hepatic echinococcosis, 11 of whom underwent surgery. There were 11 males and five females ranging in age from 27 to 79 years with a mean of 56 years and a standard deviation of 10.6. Of the 16 patients, six (37.5%) came from regions with a high incidence of hydatidosis, namely Romania and the Maghreb.
Patients were diagnosed by chance in seven patients. These patients were asymptomatic and diagnosed after imaging tests for other reasons, and because of the presence of abdominal pain in nine, one of whom presented with anaphylactic shock caused by cyst rupture; another patient had diffuse peritonitis also caused by rupture. A third had mucocutaneous jaundice caused by extrinsic compression of the biliary tract with cysto-biliary fistula. One patient had a tumor in the lumbar region corresponding to an abscess with fistulization of the cyst in that area.
Of the 16 patients diagnosed, we found multiple cysts in six patients (37.5%) and a single cyst in 10 (62.5%). Of the patients with multiple cysts, four had two; one had three; and one had four cysts. Regarding lobular involvement, the cysts were found only in the right hepatic lobe in 14 patients (87.5%) and in two patients they were found in both lobes (12.5%). There were no cases of patients with unilateral involvement of the left hepatic lobe). In terms of segmental involvement, the most affected segment was segment 4 in seven cases, followed by segment 8 in six, segment 7 in five, segment 6 in four, segment 5 in two, segment 2 in one, and segment 3 in another. The sizes ranged from 2.7 to 20 cm. Calcifications in the cyst capsule were found in 12 patients and only one patient in our series had an extrahepatic cyst associated with the pelvic level. One patient had a cysto-duodenal fistula with endoscopic evidence of purulent drainage into the duodenum (Fig. 1).
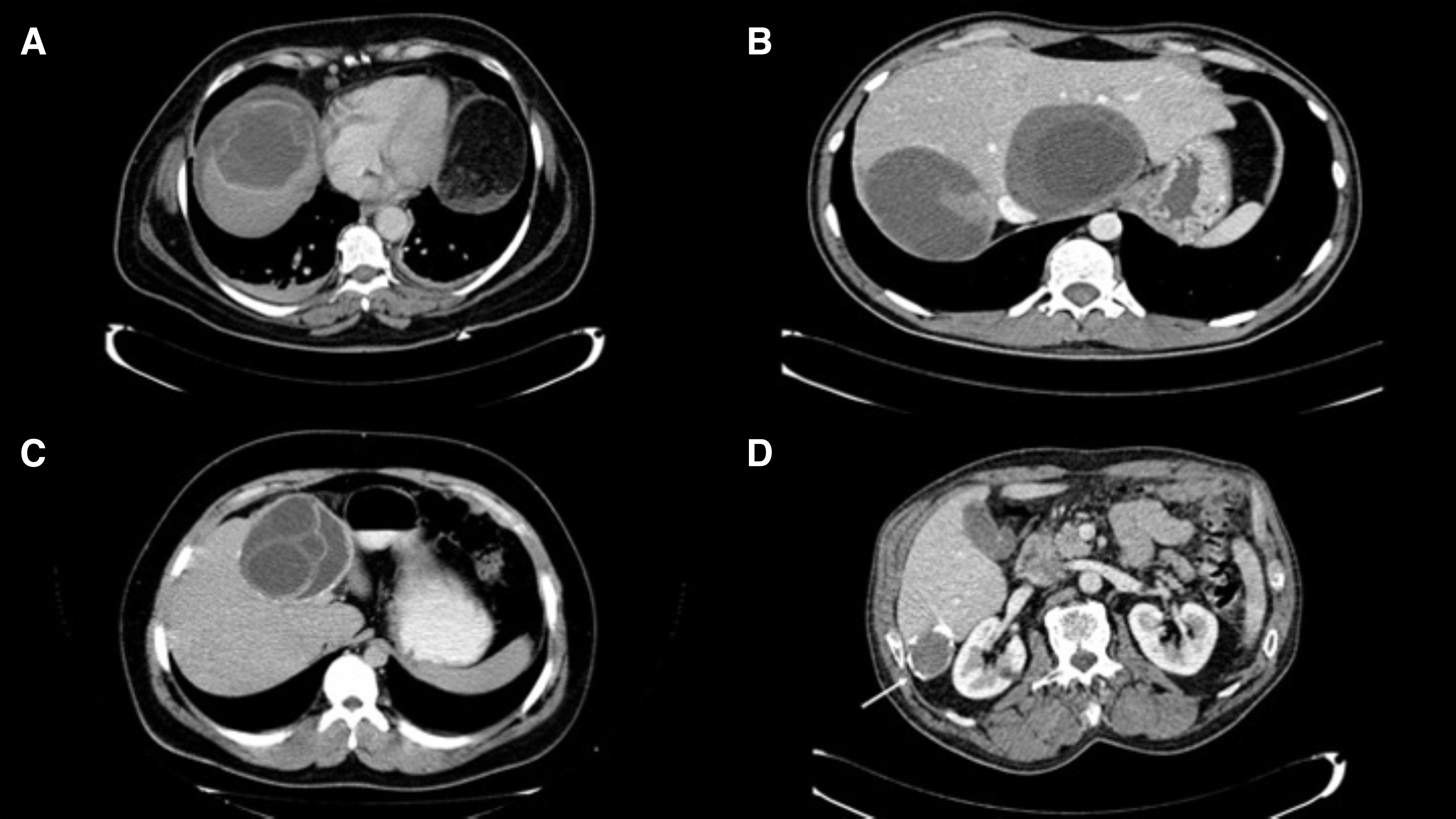
Images of hydatid cysts of the liver with some of the features we have examined in our center. (
Of the total number of patients diagnosed with hepatic hydatidosis, 11 underwent surgery and the rest were managed conservatively either by observation (watch and wait) or with oral albendazole treatment. All patients chosen in our series for this strategy were patients with stage CE4 and CE5 cysts for a follow-up of at least three to five years. In the surgical patients, albendazole treatment was administered pre-operatively between one and three months before surgery at a dose of 400 mg every 12 hours in five patients and was maintained for an additional month. Four patients were only treated post-operatively and two did not receive treatment. With preventive intent for post-operative biliary fistula, an endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy and stent placement was performed prior to surgery in five patients. The stents were removed one month after surgery or after the resolution of the fistula.
Post-operative fistulas were evident by drainage with either a bilious or purulent appearance in five patients, three of whom showed intra-operative fistula and the other two in patients who underwent emergency surgery for a proven rupture of the cyst. Regarding the closure of the fistulas, one patient closed after three months, another after one month, another developed post-operative collections that were resolved at the radiologic control after one year, and in the other two patients who started with rupture, the suppuration has subsided in one of them who is being followed up in outpatient clinics with imaging and serology tests. The other patient maintains intermittent suppuration and is awaiting definitive scheduled surgery. Neither of these two patients underwent the resection of the cyst. Four patients had residual collections in the surgical site, only two required external drainage and one patient had ascites with good evolution with conservative treatment.
All patients were followed up by radiologic controls with ultrasound, computed tomography scan, and serologic analysis. The range of follow-up time at the time of writing this article was between one and 10 years with a mean of 3.5 years. All patients have evolved favorably with the resolution of complications except for two patients with ruptured cysts who have maintained suppuration from the drainage orifice and are awaiting definitive treatment. There was no post-operative mortality in the patients reviewed. In our series, we have had no recurrence to date.
Discussion
Although there is no consensus on the establishment of medical treatment guidelines, in our center we have opted for the most recommended guideline with the administration of albendazole at a dose of 400 mg every 12 hours for one to three months before surgery and maintaining it for an additional month, although we have individualized the guideline according to the characteristics of each patient [5–8].
In our series, the most frequent hepatic involvement was with a single cyst (62.5%), unilateral and specifically of the left hepatic lobe (87.5%), and particularly of segment 4 of the liver (43.75%), this being the most frequent general profile found globally [9].
We have found the presence of post-operative fistulas in cysts as small as 6.5 cm in size. The series consulted report the presence of more morbidity from 9–10 cm [3–6,10], although as a result of the limited number of cases we cannot establish a precise limit from which complications are triggered. However, this limit of 9–10 cm seems well established when predicting the development of post-operative complications and may be one of the criteria when referring patients to a center with a hepato-biliary surgery unit before surgical treatment [6,9–11].
Most of the patients diagnosed are asymptomatic and those who have symptoms present preferentially with pain in the right upper quadrant [3,4]. Of all patients operated on, four were urgent or preferential (36.3%), one for fistula of the cyst to the main bile duct, and three for rupture. Pedunculated cysts dependent on the liver are more likely to rupture, which we have corroborated in our series because two of the ruptured cysts were cysts with this morphology. Furthermore, the frequent presence of calcifications in the cysts of these patients favors the fragility of the cyst and its predisposition to rupture, therefore, we recommend elective surgical treatment of these cysts unless there are obvious contraindications. Rupture of the cyst either into the peritoneal cavity or fistulizing into the main bile duct, the duodenum, or the abdominal wall represents a high percentage of our operations. This leads us to believe that surgical departments without hepato-biliary surgery units and with assistance to patients with urgent pathology should have basic training in interventions of this type to know how to manage these patients, because it is likely that they will face this problem at some point.
The most commonly performed elective surgical intervention was partial cyst-pericystectomy with sterilization of the cystic cavity with hypertonic saline and superficial fulguration of the internal surface of the cyst. We only performed total cysto-pericystectomy or liver resection with margins if the patient's condition or the location of the cyst were favorable for low-risk surgery. Although complete resection of the cyst is the most recommended technique [4,6], we believe that the results obtained with a partial cysto-pericystectomy are equivalent and with less risk and complications than those of radical surgery because we have had no recurrence with this technique. In contrast to central location cysts, peripheral or pedunculated cysts, which extend beyond the hepatic surface, can be undertaken by centers with a low volume of liver surgeries, because we do not consider them to be highly complex operations [3,6]. Although there is no consensus on the subject, we are in favor of placing environmental drains given the high frequency of post-operative fistula, which will facilitate early diagnosis and easier management.
In terms of size, we found a certain association between surgery on larger cysts and the development of post-operative complications, especially biliary fistula. We have corroborated that those patients whose biliary component was not treated developed a biliary fistula more easily and had more problems in its treatment. Therefore, in our department, we recommend pre-operative ERCP with endoscopic sphincterotomy and placement of a biliary stent that will be maintained or replaced until the fistula is resolved. Of the three patients who developed post-surgical biliary fistulas, excluding patients with cyst rupture, two were multiple cysts, all were moderate or large size (>6.5 cm), and in all cases with intra-operative identification of the cysto-biliary fistula and closure of the fistula, as recommended in the literature reviewed [3,12]. We are in favor of direct closure of the cysto-biliary fistula after intra-operative identification and do not believe it necessary to routinely place a Kehr tube or perform a choledochal-duodenostomy, as we believe that performing an ERCP with endoscopic sphincterotomy and placement of a biliary stent is the most practical and least aggressive method to favor the good evolution of a post-operative fistula [3].
In our series we have shown that those patients in whom we found intra-operative cysto-biliary fistulas developed a post-operative biliary fistula, considered to be a high-risk factor in the post-operative development of a biliary fistula. However, we believe that performing an endoscopic sphincterotomy and placing a biliary endoprosthesis pre-operatively facilitates a favorable post-operative evolution with earlier closure of the fistula. Patients with cyst rupture who underwent limited interventions, such as simple drainage, to resolve the urgent complications have maintained suppuration with an external fistula. This fact may lead us to consider the suitability of such a conservative treatment in patients with ruptured cysts and without instability before surgery, although in cases of unstable patients it reduces post-operative morbidity and mortality while awaiting definitive treatment of these patients.
In our series, we found that those patients with cysts in both lobes developed post-operative fistula, and of the patients with multiple cysts, half developed post-operative fistula. This, together with the fact that the literature consulted considers a number greater than or equal to three cysts as high risk for post-operative morbidity, allows us to identify patients with multiple and bilateral cysts as high risk for post-operative biliary fistula formation [3,6,10,11]. This is why we believe that these patients should be considered for referral to centers with hepato-biliary surgery units [13].
We did not find a correlation between patients of advanced age and post-operative complications such as the presence of fistulas or the formation of post-operative collections; the median age of these patients was 57 years. In a systematic review of the existing global evidence, it was found that there was a clear increase in complications for patients older than 61 years, although in several studies there was evidence of an increase in complications after the age of 41 years [3].
We have followed our patients for a mean of 3.5 years, which is within the standards of the clinical guidelines reviewed (between 3 and 5 years), thus following international recommendations [5,6]. We have had no reports of recurrences in our patients and given that most of the surgeries performed in our center were partial cysto-pericystectomies, it leads us to believe that the surgical technique chosen was appropriate with a low rate of complications, most of which were managed conservatively.
The option of observation in a select group of patients, in our case five with follow-ups ranging from 2 to 12 years, seems appropriate in asymptomatic patients with calcified cysts in ultrasound stages CE4 and CE5, given that in our series we did not need to operate on any of them and we have not found clinical or radiologic changes during follow-up [1,14–16]. We believe that the follow-up of these patients can be performed in centers without highly specialized units given the low probability that the patients being followed will need programmed intervention.
Conclusions
The saturation of the national health system leads us to consider performing low-moderate complexity liver surgeries in centers not specialized in hepato-biliary surgery such as ours, with our results being acceptable by international standards. We believe that patients with hydatid liver cysts who present urgent complications such as cyst rupture or cholangitis due to biliary hydatid disease resulting from these cysts should be given adequate care. Based on our experience, we have proposed to identify the characteristics of patients who have presented post-operative complications to assess in the future the appropriateness of performing these interventions in our center or centers such as ours. To this end, we have set out some simple recommendations for the referral of patients at high risk of complications based on literature and our experience (Table 1). In conclusion, we can state that centers without highly specialized hepato-biliary surgery units can assume the surgery of hydatid liver cysts excluding those with well-defined characteristics. The establishment of recommendations for the referral of patients with complex hydatid cysts may help in the optimal management of this pathology.
Recommendations for Referral of Patients with Hydatid Cysts of the Liver to Centers with Specialized Hepato-Biliary Surgery Units
HBSU = hepato-biliary surgery units; MBD = main bile duct; MVS = major vascular structure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.