
Abstract
Abstract
Background:
Clostridioides difficile infection (CDI) is a common and sometimes life-threatening illness. Patient-, care-, and room hygiene-specific factors are known to impact CDI genesis, but care provider training and room topography have not been explored. We sought to determine if care in specific intensive care unit (ICU) rooms asymmetrically harbored CDI cases.
Patients and Methods:
Surgical intensive care unit (SICU) patients developing CDI (July 2009 to June 2018) were identified and separated by service (green/gold). Each service cared for their respective 12 rooms, otherwise differing only in resident team composition (July 2009 to August 2017: green, anesthesia; gold, surgery; August 2017 to June 2018: mixed for both). Fixed/mobile room features and provider traffic in three room zones (far/middle/near in relation to the toilet) were compared between high-/low-incidence rooms using observation via telecritical care video cameras.
Results:
Seventy-four new CDI cases occurred in 7,834 consecutive SICU admissions. In period one, green CDI cases were almost double gold cases (39 vs. 21; p = 0.02) but were similar in period two in which trainee service allocation intermixed. High-incidence rooms had closer toilet-to-intravenous pole proximity than low-incidence rooms (7.7 + 1.8 feet vs. 3.9 + 1.5 feet; p = 0.02). High-incidence rooms consistently housed mobile objects (patient bed, table-on-wheels) farther away from the toilet. Although physician time spent in each zone was similar, nurses spending more than 15 minutes in-room more frequently stayed in the far/middle zones in high-incidence rooms.
Conclusions:
Distinct SICU room features relative to toilet location and bedside clinician behaviors interact to alter patient CDI acquisition risk. This suggests that CDI risk occurs as a structural aspect of ICU care, offering the potential to reduce patient risk through deliberate room redesign.
Escalating healthcare costs in the United States and other resource-replete nations drives efforts at containment while ensuring care quality and value. Low-value care that spans diagnostic and therapeutic interventions is scrutinized by a host of medical professional societies under the auspices of the American Board of Internal Medicine's Choosing Wisely campaign [1]. Indeed, purposively modifying care plans to reduce cost, and at least maintain if not improve value and quality, appears as part of antimicrobial stewardship programs (ASP) to reduce the driving pressure for multi-drug–resistant organism genesis [2]. A key consequence of inappropriate intensity or duration antibiotic prescription—as well as culture-driven therapeutic courses—is Clostridioides difficile infection (CDI). Ranging from asymptomatic carriage to fulminant life-threatening colitis, CDI engenders substantial health system costs, and may have persistent patient consequences if surgical rescue is required [3,4]. Although efforts to reduce antibiotic distortion of a patient's normal microbiome reduce the likelihood of CDI as a result of therapeutic intervention, ASP practices do not address environmental factors that lead to CDI acquisition during inpatient care.
Clostridioides difficile infection is readily acquirable from residual spores found in care spaces after routine between-patient cleaning has been completed [5]. This observation suggests that more careful or more intense efforts at room disinfection could achieve spore eradication [6]. Accordingly, facilities pursue a variety of disinfection interventions to reduce the spore burden in the care environment, including ultraviolet light-based sanitization [7,8]. Nonetheless, de novo CDI acquisition persists in critically ill patients who require care in the intensive care unit (ICU). Closely related to the fecal transmission of CDI is the hospital in-room toilet and its utilization for disposal of waste. Because most ICU toilets are lidless, evidence exists implicating flushing as a vector in dissemination of spores because of the unrestricted plume that is enabled when lidless toilets are flushed, promoting dispersion of particles and contaminants in the surrounding surfaces of the room [9].
In a quality improvement initiative, certain ICU rooms were found to have housed most CDI cases cared for in a nine-year period. This unexpected finding led the authors to investigate whether there were specific team composition elements, structural room features, or clinician behaviors that were associated with de novo CDI acquisition.
Patients and Methods
This multi-part study was driven by ICU quality improvement discussions and followed sequential discussions and questions that were raised by bedside ICU providers. This began with nurses raising the concern that CDIs appeared to occur more frequently in specific ICU rooms and preferentially in one of the two surgical intensive care unit (SICU) services. In these discussions CDI acquisition was explored incrementally to determine potential causative elements. These processes led to the study's sequential four-phase approach: de novo CDI identification and incidence determination; structural feature assessment of rooms based on CDI incidence; mobile care in-room device traffic patterns; and visitor and clinician traffic patterns. This study was approved by the University of Pennsylvania Institutional Review Board (IRB; protocol #813837) with specific note of waiver of informed consent for telemedicine assessment supporting quality improvement activities.
We first utilized retrospective ICU database analysis to review all healthcare-onset CDI cases (Bristol scale 5–7 stool specimen positive for Clostridioides difficile toxin A/B by immunoassay) obtained after hospital day three for a period of nine years and determined the patient's room and ICU service. Once it was confirmed that certain rooms harbored more CDI cases than others, high-frequency rooms (empirically defined as the top three or five rooms in CDI cases of the 24 ICU rooms) were compared with low-frequency rooms (lowest three or five rooms with CDI infections) in how their immutable structural attributes (floor dimensions, window/wall sizes, curtain length, etc.) differed. The last two parts of the study utilized in-room observation through telemedicine cameras and sought to evaluate traffic patterns of movable furnishings (wheeled table, bed, etc.) and traffic patterns of personnel and the patient within the rooms of the two groups.
Setting
The Hospital of the University of Pennsylvania (HUP) is an urban, 776-bed, quaternary care center with a 24-bed SICU that cares for mixed surgical patients other than after cardiac or neurosurgical interventions. The 24 beds are allocated equally to two ICU teams that are equally staffed in terms of numbers of clinicians (intensivists, trainees including fellows, advanced practice providers [APP], doctors of pharmacy, respiratory therapists; Fig. 1). Nurse assignment is random and not connected with admitting team specialty, acuity, or specific intervention competency. Attending intensivists are rotated on a weekly basis by alternating training specialty between surgery and anesthesia and also originate from the same pool for both services. Patients are randomly allocated to each ICU, and therefore, service (green service, rooms 5001–5012; gold service, rooms 5013–5024; Fig. 1) without regard to originating service or acuity. A high-acuity unit, the SICU, cares for an average of 210 unique patients per month. Each room is filled with equal frequency and the entire SICU is routinely filled to capacity.
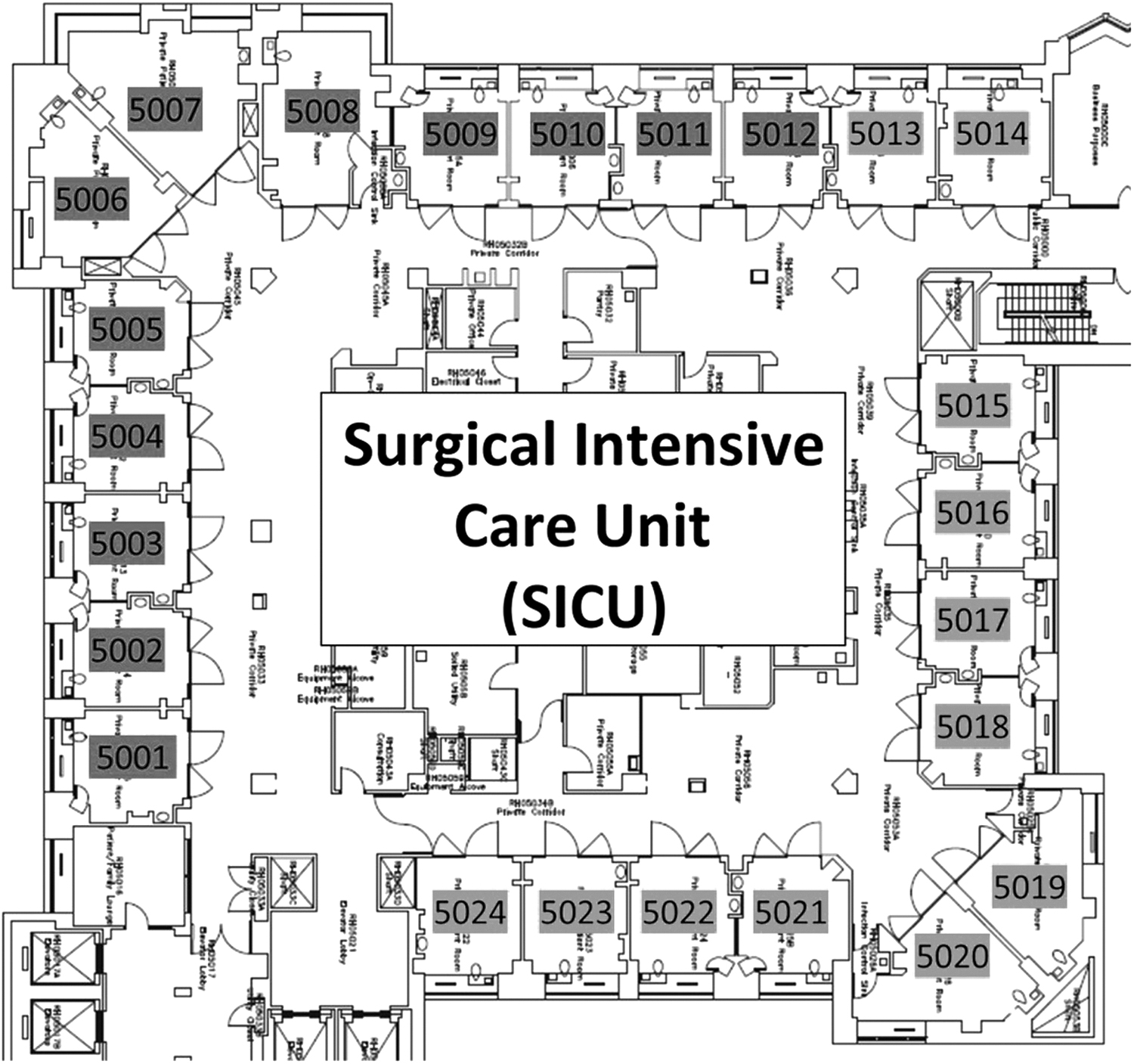
Geography and topography of the surgical intensive care unit (ICU) at the Hospital of the University of Pennsylvania (HUP). Shading indicates service allocation (dark gray and light gray service rooms).
Room cleaning and disinfection practices followed strict guidelines from the U.S. Centers for Disease Control and Protection (CDC) and the Occupational Safety and Health Administration (OSHA) using Environmental Protection Agency (EPA)-approved disinfectants per hospital policy. This included such practices as one daily cleaning and two (morning and evening) daily “Refreshings” and one weekly floor burnishing. Utilization of 1:10 dilution of 5.25% sodium hypochlorite (bleach) wipes was routine throughout the study period but standard utilization of terminal cleaning with ultraviolet wavelength C germicidal irradiation (UVGI) was initiated in January 2014.
De novo CDI case identification and incidence determination
All patients with CDI were identified using the hospital's infection control database (July 1, 2009 to June 30, 2018). Included patients received care in the SICU and had the first-ever CDI diagnosed (Clostridioides difficile toxin by immunoassay) after SICU admission (de novo infection); those admitted to the SICU for ongoing CDI care were excluded. Specifically, patients with a positive immunoassay had to have been physically present in the SICU when the sample was obtained, not in the emergency department or ward prior to transfer to the SICU.
Patients with de novo CDI were parsed by SICU service (green vs. gold; Fig. 1). Between July 1, 2009 and August 31, 2017, green service beds were staffed using anesthesia trainees, whereas gold service beds were staffed using surgery trainees from different parent training pathways (i.e., general surgery, vascular, plastic and reconstructive, orthopedic, obstetrics-gynecology, oral and maxillofacial surgery, as well as emergency medicine). Unrelated to this study or other clinical outcomes, trainees were thereafter randomly allocated to either team (September 1, 2017 to June 30, 2018). The frequency of CDI during the study period was further parsed by the specific room in which de novo CDI occurred to define high- or low-frequency rooms as defined above. Additionally, the care of a prior patient with CDI in each room in which a de novo infection was identified was captured.
Topographical and structural features of SICU rooms
The topographical dimensional relations of high- and low-incidence rooms were assessed using a laser distance and length measuring device (Model GLM 20, Robert Bosch LLC, Farmington Hills, MI). Topographical room elements included room dimensions, distances between fixed elements, and distances between fixed elements (i.e., the toilet) and routinely placed mobile elements such as the bed or intravenous pole(s) (Table 1). Between-group comparisons sought to identify common or disparate findings between high- and low-CDI incidence rooms.
High- and Low-Incidence Rooms: Topographical and Organizational Factors
CDI = Clostridioides difficile infection.
Mobile element traffic: Telecritical care camera observation
Within-room mobile furnishing traffic was assessed by a dedicated author (April 6, 2020 to May 28, 2020) in 51 separate 90-minute sessions using pre-existing in-room telecritical care (TCC) cameras. Assessments were a convenience sample that reflected the assessors schedule and were confined to typical business hours. No more than three observation sessions were conducted per patient per room. During each session, the observer documented where moveable room furnishings (i.e., chairs, hospital bed, and table-on-wheels) were found or moved in relation to the toilet during the same observation period.
Telecritical care cameras are part of a network-wide TCC platform that are used in a pre-established performance-improvement–driven institutional policy that allows video recording of ICU bedside care to observe in-room behaviors and patterns [10,11]. The cameras are located above the foot of the patient's bed, mounted on the wall close to the ceiling. Although clinicians and patients are apprised of the TCC approach and are informed that assessment and recording may occur at any time, routine care is not interrupted during video evaluations. Consent for recording is obtained as part of a global ICU consent form within the context of quality improvement activities.
The toilet was utilized as a fixed point of reference against which other mobile furnishings were assessed. The distance between toilet and furnishing was defined a priori using circumferential zones centered on the toilet location. Each room was divided into three zones (near, <4.5 feet; middle, 4.5–9 feet; and far, >9 feet; Fig. 2). Zones were defined based on flush-driven bioaerosol generation of particles in the 2- to 3-mcm range that reach at least 3.3 feet away from a toilet and up to 2.7 feet above the bowl [12,13]. Each zone was measured in-person and then digitally marked and superimposed on room footage using fixed camera coordinates to ensure accuracy and reproducibility between assessments.
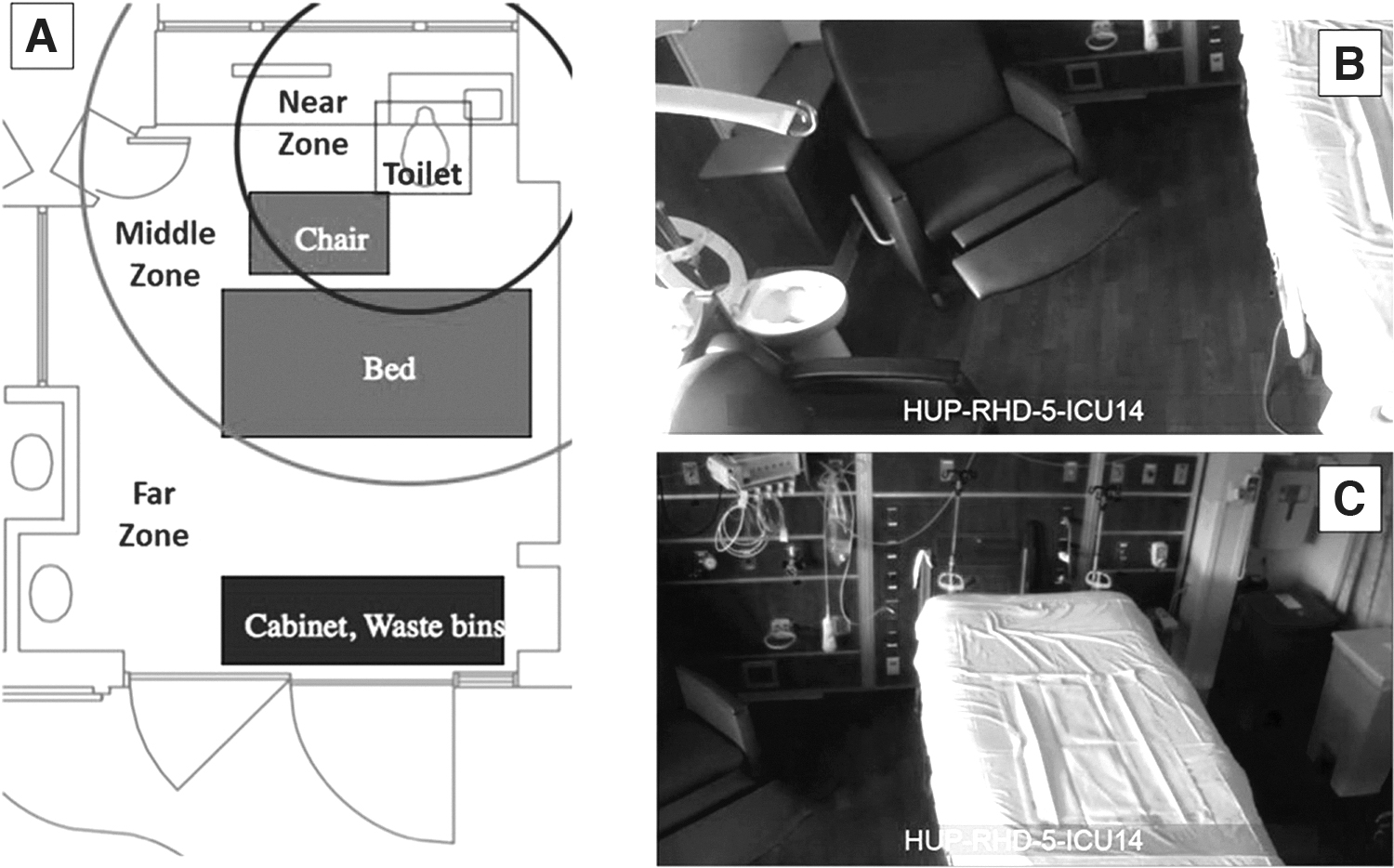
Each room was divided into three radial zones by distance to the lidless toilet (
Visitor and clinician traffic: TCC camera observation
Utilizing the same recordings detailed above, visitors or clinician in-room time and specific zone location was assessed as defined above. Clinician room time spent in each specific zone was separately documented. Clinician traffic in each zone was defined as short (<3 minutes), moderate (3–15 minutes), or long term (>15 minutes) to facilitate analysis. Each observation period began the moment a hospital provider entered a patient's room and were concluded once 90 minutes had elapsed.
Statistical analysis
Univariable evaluation of CDI incidence by the ICU team was conducted using χ2 analysis. Independent univariable analysis using two-tailed t-test and Fischer exact test was conducted as appropriate for comparisons between high- and low-CDI incidence rooms with respect to mobile furnishing and human traffic. A p value of <0.05 was considered statistically significant. All analyses were conducted using SPSS Statistics, version 26 (IBM Corp, Armonk, NY) and RStudio 2020 (RCore Team, Boston, MA).
Results
De novo CDI incidence
Eighty-five cases of CDI infection were identified in patients after SICU admission and developed while in the unit, nine of whom were excluded because they had a previously positive test. This left a total of 74 de novo CDI cases among 7,834 SICU patients (July 2009 to June 2018). Of all CDI cases in the study period, 49 were males and 25 females (66% males vs. 34% females; p < 0.01). This ratio was similar in high- and in low-CDI incidence rooms (p = 0.47). From July 2009 to August 2017, CDI cases in green service rooms were twice that in gold team rooms (Fig. 3A; green vs. gold, 39/3328 vs. 21/3246; relative risk [RR], 1.8; 95% confidence interval [CI], 1.0624–3.056; p = 0.03). This difference was lost in the subsequent time period during which resident specialty was no longer driven by discipline (Fig. 3B). During the first eight-year period, green team rooms housed more male than female CDI patients (green, 23 vs. gold, 9; 72% vs. 28%; p < 0.01) whereas the gold team patients were not different by gender (9 vs. 4; p = 0.17). Additional demographic analysis revealed no relation between increased CDI incidence and patient age or month and season of admission.

Impact of trainee specialty allocation on Clostridioides difficile infection (CDI) incidence (cases per 1,000 patients).
Preceding CDI patient stays within six months of de novo infection for a given room clustered in high incidence rooms. In the three highest incidence rooms, seven of the 17 total cases were preceded by a CDI infected (range, 1–2) patient within the prior six months. Of the highest incidence rooms, one of the cases was immediately preceded by a CDI case in the same room. The highest incidence room (room 5011) saw three cases in the span of six months. In contrast, the three lowest incidence rooms rendered care to zero preceding CDI patients in the prior six months.
Topographical and structural features of SICU rooms
Comparing high- (three highest incidence rooms) and low- (three lowest incidence rooms) incidence rooms demonstrated that high-incidence rooms housed closer toilet-to-intravenous pole proximity compared with low-incidence rooms (7.67 feet +1.82 feet vs. 3.87 feet +1.48 feet; p = 0.02) and increased height of privacy curtains (9.01 feet +0.09 feet vs. 8.67 feet +0.17 feet; p = 0.04; Table 1). There was no observed difference in door curtain surface area and length between groups. No room had a lidded toilet. All rooms featured sliding closable glass doors.
Mobile element traffic
In-room traffic assessment via TCC camera was conducted in high- and low-CDI incidence rooms. Mobile furniture distribution was different between high- and low-incidence rooms. High-incidence rooms positioned the bed (33.3% vs. 3.7%; p = 0.01) and table-on-wheels (over-the-bed table) (89.5% vs. 53.3%; p = 0.02) consistently in the middle/far zones compared with low-CDI incidence rooms. Patient power lifts demonstrated a similar, but not statistically significant, distribution pattern (75.0% vs. 48.1%; p = 0.08; Fig. 4). Zone presence of the moveable bedside (not over-the-bed) table, supply cabinet, in-room computer/keyboard, and biologic or non-biologic waste bins did not show differences between high- and low-incidence rooms (Table 2).

Percent time the movable object/furnishing was in far/middle zones. Fraction indicated on histograms indicate number of times seen over total number of observations taken. Vertical axis indicates percent of time observed in the far/middle zones. Low Clostridioides difficile infection (CDI) incidence rooms, mean for the three of 24 surgical intensive care unit (SICU) rooms with lowest CDI cases in the eight-year study period. High-CDI incidence rooms, mean for the three of 24 SICU rooms with highest CDI cases in the eight-year study period.
Time Spent by Mobile Objects in Far/Middle Zones for High- and Low-Incidence Rooms
Clinician in-room traffic
Human traffic in the different zones of high- and low-incidence rooms was observed with TCC cameras and analyzed with regard to zone dwell time. Visitor presence was sufficiently infrequent, as was patient location outside of the bed, that these data could not analyzed in a meaningful fashion. In assessing long-term (>15 minutes) in-room visits by bedside clinicians, the proportion of time nurses spent in far and middle zones was greater in high-(77.3%) than low- (67.9%) incidence rooms (p < 0.01; Fig. 5A). The proportion of long-term physician visits spent in each zone was similar in high- and low-incidence rooms (Fig. 5B). The mean in-room nurse time did not differ between high- and low-incidence rooms.
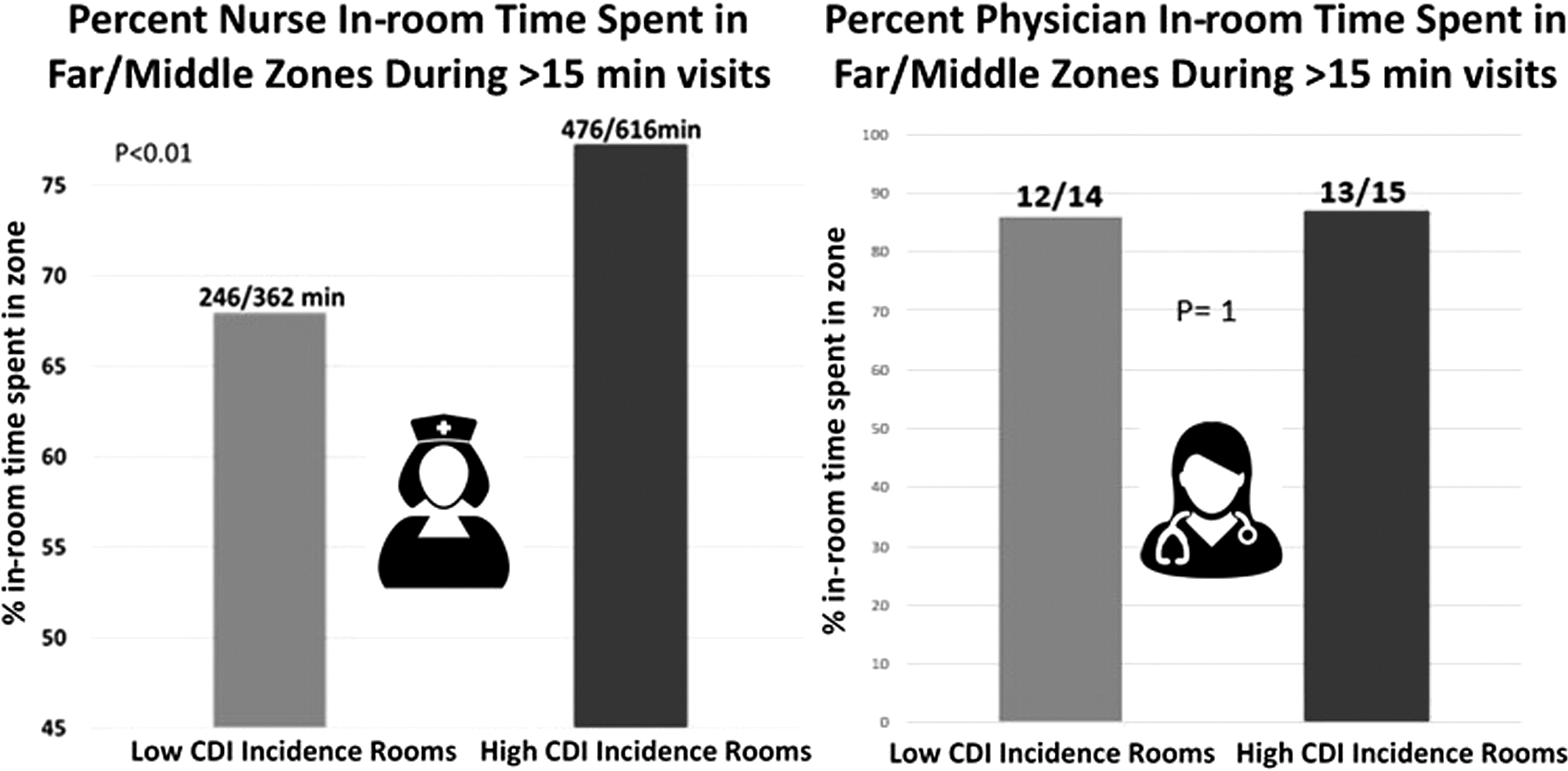
Percent time spent by nurses and physicians in far/middle zones for long-term (>15 minutes) visits. Low Clostridioides difficile infection (CDI) incidence rooms, mean for the three of 24 surgical intensive care unit (SICU) rooms with lowest CDI cases in the eight-year study period. High-CDI incidence rooms, mean for the three of 24 SICU rooms with highest CDI cases in the eight-year study period.
Discussion
Patients in ICUs not only face higher mortality rates from CDI [14], but also have prolonged length of stay [15,16] and increased care cost [17]. Deploying appropriate preventive measures could save approximately $3.8 billion in CDI-related care according to a CDC estimate [18]. This health system cost spurred the articulation of a variety of guidelines and best practices to reduce both inpatient and outpatient CDI incidence. Despite guideline dissemination and standard precaution practices, critically ill or injured patients remain at risk of developing CDI as a result of empiric or therapeutic antibiotic courses with native microbiome distortion. All of our ICU rooms are single occupancy, eliminating the transmission risk imposed in dual-occupancy spaces [19]. Nonetheless, additional risk flows from the environment of care even in the absence of concomitant antibiotic therapy. That is to say, in our academic tertiary center, patients admitted for non-CDI care were more likely to develop CDI in certain rooms than in others. The chance finding that certain hospital rooms harbor recurrent CDI in a given ward cared by a homogeneous group of care providers is not new and has been reported before [20]. Our dual team ICU structure offered a unique setting in which to explore factors that exacerbate do novo CDI acquisition risk.
Regarding the study period, our two SICU teams were identically staffed except for the parent training discipline of rotating trainees. This allowed for a unique opportunity to focus an evaluation of trainee allocation on de novo infection risk. Prior studies have only assessed heterogeneous clinician groups. Our findings noted that during most of the study when one service was exclusively staffed using anesthesia trainees, that service (green) demonstrated almost double the incidence of de novo CDI compared with the other team staffed by surgery and emergency medicine trainees (gold). Importantly, this observation vanished when trainees were randomly allocated to each team. Of note, other aspects of patient allocation to one team or the other, nurse staffing, APPs staffing, attending rotation, fellow allocation, and other clinician allocation, as well as sanitization practices, were consistent throughout.
Superficially, the data suggest that CDI is strongly tied to trainee allocation. Potential explanations, none of which were the subject of this study, could include asymmetric hand hygiene, standard precaution compliance, Clostridioides difficile testing threshold, or antimicrobial stewardship practices. Although some of these may be operative, major decision-making occurs at the attending level, a factor unassociated with CDI risk in our study. Furthermore, some antibiotic practices are driven by the admitting team and not the ICU team and therefore should not be linked to a specific trainee set. Heterogeneity of trainees might plausibly support improved infection control, especially if the trainee group is more likely to include intern-level clinicians, and therefore garner additional oversight or attention from seasoned clinicians to support guideline and best-practice adherence. Alternatively, intra-group guidance might have also informed guideline and best-practice adherence or could have impacted testing frequency. Clearly other elements or coexisting attributes of each resident group (age, gender, seniority distribution, etc.) were not tracked and one group may have had different coexisting attributes that may have contributed to these differences. Nonetheless, the current study underscores the notion that clinician behavior and interface with room features offer modifiable elements that impact de novo CDI acquisition risk. Although this study was not designed to assess clinician behaviors, it did investigate whether the CDI risk asymmetry reflected structural differences tied to room topography or room use.
To determine if the high-risk CDI rooms (primarily on the green service) were themselves discrete risk factors for increased incidence, we assessed room organization and topography. Eradicating Clostridioides difficile spores is problematic even when utilizing terminal sanitization approaches including, hand cleaning and ultraviolet light [21]. Furthermore, variability in custodial practices including effort intensity in covering all surfaces with sporicidal agents remain inconsistent, supporting spore persistence for months [22]. Accordingly novel approaches have emerged including using aerosols or vapors of sporicidals such as hydrogen peroxide to access interstices and difficult to reach areas in rooms exposed to CDI [23]. Other approaches include a combination of probiotics and bacteriophages on accessible surfaces [24]. Sanitization practices are optimal during patient transitions when the room is unoccupied but may be less ideal during intercurrent care.
Current ICU room standards include in-room toilets that are minimally enclosed and are routinely lidless. Yet toilets aerosolize waterborne particles when flushed and create a bioaerosol that may transmit bacteria and spores in droplets that are as small as 2- to 3-mcm in diameter. Bioaerosolization after toilet flushing and plume dispersal has been implicated in CDI transmission [9]. Indeed, after flushing of fecal matter, Clostridioides difficile has been recovered from more than 25 cm above the toilet surface and remains present on contact surface for longer than 60 minutes, and in the toilet basin after more than 24 sequential flushes [9,25]. Indeed, aerosolization of Clostridioides difficile allows spores to travel and land on surrounding surfaces, creating numerous sources of further contamination.
Recognizing that Clostridioides difficile is not the only pathogen subject to bioaerosolizaton, room privacy curtains are routinely changed as they are a high-touch surface whose presence is modifiable. Kim et al. [26] reported that Clostridioides difficile spores can survive on high contact surfaces for more than five months. Separately, we also found that almost one-half of CDI cases in the high-incidence rooms were preceded by a previous CDI case in that same room whereas none of the low-incidence room CDI cases were preceded by a CDI case in the preceding six months. Taking together previous and current findings, it stands to reason that in ICU rooms, objects located within close range to toilets may harbor endospores and enhance CDI contamination risk in certain parts of the room despite seemingly adequate sanitization practices [21].
We observed that rooms with greater CDI incidence had significantly closer toilet-to-intravenous pole distances compared with rooms with lower incidence. Although intravenous poles were clearly changed between patients when rooms were turned over and intravenous poles may have been added or removed even within one patient's stay, the fact that the location of where intravenous poles were located was closer in high-risk rooms questions how the placement of room elements might influence contamination risk. Intravenous poles are another high-contact surface particularly for nursing staff. Importantly, during TCC observations it was noted that although intravenous poles are mobile, hospital staff infrequently relocated them. With respect to fixed geography furnishings, higher incidence rooms had taller privacy curtains located at the room's entrance that were more likely to nearly reach the floor compared with lower incidence rooms. Although this difference was statistically significant, curtains of different sizes were available, and this difference may have coincidentally occurred on the day of observation. Moreover, curtain length is not a constant as curtains are routinely exchanged in random fashion regardless of length.
Evaluating furniture and staff movement in rooms using video observations revealed a seemingly opposite yet more consistent relation with mobile objects. We observed that the bed and wheeled table were consistently farther away from the toilet in higher incidence rooms. The most common position of the ceiling-mounted patient lift seemed to follow the same distance trend although this failed to reach significance. On the other hand, in no instance was any moveable furnishing more commonly far from the toilet in low-incidence rooms compared with high incidence rooms. Although mean room square footage in high- and low-incidence rooms were similar, geography was not identical. Therefore, our findings perhaps suggest that room navigability may be more important when evaluating potentially contaminated but traffic accessible space.
In parallel, certain in-room movement of bedside caregivers also showed the same farther relation in high-incidence rooms. Live observations of staff traffic revealed that long nursing staff visits were spent a greater time in farther zones from the toilet in high-incidence rooms. These results suggest that rooms with more open and navigable space may traffic Clostridium difficile endospores to more locations, some of which may be difficult to clean, despite adherence to best practice infection control and sanitization protocols. As a corollary, CDI may not be unique in this respect and it remains unknown if the same relations exist with other fecal or water-borne pathogens of clinical significance such as Acinetobacter, multi-drug–resistant gram-negative enteric bacteria, vancomycin-resistant enterococcus, and others.
Linking data from trainee allocation asymmetry with CDI incidence and room topography and traffic data highlights how these features interact to influence de novo CDI acquisition risk. We found that in high-incidence rooms, seven of 17 de novo CDI cases were preceded by prior CDI cases within the previous six months. Conversely, none of the de novo CDI cases in low-incidence rooms were preceded by prior infections in a six-month time period. The transmission of Clostridioides difficile by prior room occupants has also been reported previously [19]. Relatedly, certain rooms may be constructed with features that make the complete elimination of endospores during terminal room cleaning more difficult and therefore inadvertently increase a subsequent room patient's risk of developing CDI. Although this study did not identify such characteristics—and a later study should focus on these elements—increasing trainee allocation heterogeneity exerted a beneficial effect even in high-incidence rooms.
Although leveraging a unique structure that allows team-based evaluation informed by room topography and clinician traffic, this single-center study has important limitations. First, inclusion of patients in the study required CDI immunoassay positivity if and only if the sample of stool was obtained while the patient was physically in the SICU, i.e., not on the ward or emergency department prior to transfer to the SICU. Clearly certain patients may have been positive for CDI prior to arriving to the SICU without anyone sending a test before their transfer and as such these patients would have been included despite CDI acquisition prior and outside the SICU.
Second, during the time period in which the data collection took place, HUP's protocol for CDI detection and diagnosis changed. However, given that this protocol change impacted all SICU rooms equally, this should not have resulted in asymmetric differences.
Third, we did not classify CDI by clinical severity to gauge clinical impact, and instead used a binary approach as our focus was de novo acquisition. Variations in CDI clinical severity may represent underlying differences in bacterial strains and the presence or absence of virulence factors thereby contributing to risk of infection. Similarly, some patients are at increased risk of developing CDI because of age, use of antibiotic agents, use of proton pump inhibitors, and a number of other factors that were not accounted for in this study. Additionally, patient mobility may have also contributed to a patient's risk related to their potential to reach and high-contact objects.
Fourth, no observations were made on use of in-room toilets and sinks, either by the patient or nurse disposing of patient waste. It would have been interesting to know if nurses used toilets and sinks differently to dispose of body fluids when nearer to the bed as opposed to a sink.
Fifth, the study did not assess environmental contamination with Clostridioides difficile, nor observe and compare adequacy of terminal room cleaning, and provider compliance with hand hygiene or personal protective equipment. Sixth, we did not assess trainee behaviors, room entry frequency by diagnostic equipment or their operators, nor did we assess length of stay ICU or hospital length of stay, elements undoubtedly related to room risk of infection and contamination.
Last, the telemedicine observation sessions occurred during the coronavirus disease 2019 (COVID-19) pandemic when the SICU only provided care to patients confirmed to be infected with severe acute respiratory syndrome coronavirus-2 (Sars-CoV-2). For this reason, no APPs and visitors were not observed in any of the rooms as the policy at the time was that only attendings and nurses be allowed in the rooms as this was at the height of the first wave of the pandemic, potentially missing this influence on CDI acquisition risk. Thus, it is possible that the moveable object and bedside provider traffic patterns were those during COVID-19 practices and not necessarily representative of movement during prior episodes of care.
Conclusions
The results of this study reveal that previously unexplored factors such as room structure, organization, staff movements, and trainee specialty may play a role in a patient's risk for developing CDI while requiring critical care. Surgical ICU rooms uniquely staffed by clinicians from one specialty had higher incidence of CDI compared with rooms staffed by residents from more heterogeneous training backgrounds. Higher incidence rooms contained significantly closer toilet-to-intravenous pole distances, and mobile objects that were more often farther away from the toilet. Further investigation is needed to identify differences in bedside traffic patterns and de novo CDI acquisition risk during an episode of critical illness. These data should inform ICU room renovation as well as plans for new ICU space construction.
Footnotes
Funding Information
None of the authors declare any financial support.
Author Disclosure Statement
No competing financial interests exist.