
Abstract
Background:
Early debridement improves outcome in necrotizing soft tissue infection (NSTI), but there is no consensus on duration of antimicrobial therapy. We recently changed practice to discontinue antibiotic agents early with a goal of 48 hours after adequate source control. We hypothesized that discontinuing antibiotic agents after a short course is safe in the treatment of NSTI.
Patients and Methods:
This was a prospective study of patients with NSTI comparing short duration of antibiotic agents to a control population after a change in practice. In 2018 we began discontinuing antibiotic agents within 48 hours of source control (absence of cellulitis and no evidence of active infection). Previously, antibiotic duration was at the discretion of the attending surgeon (generally 7–10 days). Patients were excluded from analysis if they were initially debrided at a referring facility, immune compromised, or died prior to source control. Patient characteristics and outcomes were evaluated. The primary outcome was treatment failure requiring antibiotic agents to be restarted with or without further debridement of infected tissue. Secondary outcomes included the duration of antibiotic therapy after source control.
Results:
We evaluated 151 patients; 119 admitted between January 1, 2011 and January 31, 2018 (PRE) and 32 admitted after January 31, 2018 (POST). Patients were not statistically different regarding characteristics, admission physiologic variables, and comorbidities. The median duration of antibiotic agents after source control in the PRE group was 180.3 hours (interquartile range [IQR], 100.7–318.8) versus 48 hours (IQR, 32.3–100.8) in the POST group (p < 0.01). Patients in each group were treated as described above, and treatment failure occurred in seven (5.9%) PRE patients and two (6.3%) POST (99.3% post hoc power at non-inferiority limit 20%, significance p < 0.05). Thirty-day all-cause mortality was not different between groups (6.7% vs. 6.3%; p = 0.94).
Conclusions:
Short-duration (48 hours) antibiotic agents after NSTI source control is as safe and effective as a longer course.
Necrotizing soft tissue infections (NSTIs) are a group of life-threatening soft tissue infections associated with tissue destruction, systemic signs of toxicity, and high mortality. Mortality has been shown to range between 20% and 50% [1]. Historically, NSTIs include necrotizing cellulitis, necrotizing myositis, and necrotizing fasciitis (including Fournier gangrene), with each variation being named for the layer of tissue affected.
Necrotizing soft tissue infections are further divided into type 1 (polymicrobial) or type 2 (monomicrobial). Type 1 infections are most frequently encountered in patients with diabetes mellitus and peripheral arterial disease and usually include a combination of anaerobic species and Enterobacteriaceae. Type 2 infections can occur in otherwise healthy individuals but are often associated with a history of trauma such as surgery, intravenous drug abuse, or water exposure. Type 2 infections are usually caused by group A Streptococcus (GAS), Staphylococcus aureus, or, in the case of water exposure, Vibrio vulnificus (salt water) or Aeromonas hydrophila (fresh water). The water-borne infections are sometimes assigned to a lesser recognized type 3 category [2]. The mainstay of therapy for NSTIs, regardless of the location or type, is early surgical debridement and broad-spectrum antibiotic coverage [3], but the duration of antibiotic therapy has not been well studied.
The Infectious Diseases Society of America has suggested using empiric broad-spectrum antibiotic agents until source control is achieved by surgical interventions, and there is evidence of clinical improvement including the patient remaining afebrile for 48–72 hours, although this was not a formal recommendation [4]. Anaya and Dellinger [5] suggested continuing antibiotic agents until no further debridement was needed and the patient's physiology improved. Because there is no expert consensus regarding antibiotic duration, there is wide variation regarding the practice of antibiotic duration; in one retrospective review, it was shown that although antibiotic agents were started in a timely manner and the total number of operations was similar across three centers, the duration of antibiotic therapy varied greatly between nine days and 16 days [6]. Another retrospective review demonstrated that in patients being treated for Fournier gangrene, when stratified into treatment groups based on antibiotic therapy for seven days or less, eight to 10 days, 11 days to 14 days, or 15 days or more, there was no difference in mortality and no recurrent cases between the four groups [7]. At present, there exist no recommended monitoring techniques or biomarkers available to guide the discontinuation of antibiotic agents used in the treatment of NSTIs [8].
As part of a quality improvement project, we recently changed practice with respect to antibiotic therapy of NSTI. On the basis of our anecdotal experience of excellent outcomes associated with aggressive surgical debridement and shorter courses of antibiotic agents, we began discontinuing antibiotic agents by 48 hours after confirmed adequate source control. The purpose of this project was to evaluate the safety of a short course of antibiotic agents in NSTI, and our hypothesis was that discontinuing antibiotic agents after a short course in the presence of adequate debridement is safe in the treatment of NSTI.
Patients and Methods
After Institutional Review Board approval, we performed a prospective study of patients with NSTI after changing our antibiotic management protocol at Wake Forest Baptist Medical Center in Winston-Salem, North Carolina. Prior to January 2018, antibiotic duration for the treatment of NSTIs was at the discretion of the attending surgeon (generally 7–10 days). Historically, antibiotic agents were continued well beyond source control. It has been our practice for some time to aggressively and repeatedly debride patients until we see appropriate improvement in clinical conditions, usually reflected in hemodynamics and overall clinical picture. This has not changed over time. However, after January 2018, we began discontinuing all antibiotic agents at 48 hours after we had obtained source control. Necrotizing soft-tissue infections were identified grossly by surgeons in their operative notes. Adequate source control was defined as the absence of cellulitis with a clean wound bed noted at subsequent wound examination. We chose 48 hours a priori based on anecdotal experience in which more than 48 hours of antibiotic therapy did not appear to add benefit, assuming source control was adequate.
All patients in this study were prescribed broad-spectrum antibiotic agents as soon as NSTI was suspected and were taken to the operating room as soon as possible. Antibiotic type was chosen at the surgeon's discretion, however, patients were treated with a combination of vancomycin intravenous or linezolid (for methicillin-resistant Staphylococcus aureus [MRSA] coverage), clindamycin (for anti-50s ribosomal activity to interfere with bacterial toxin synthesis), and either piperacillin-tazobactam, cefepime and metronidazole, or meropenem (for broad-spectrum coverage). Once in the operating room, all devitalized tissue was debrided. Afterwards, the patient was maintained on broad-spectrum antibiotic agents until subsequent wound examination. At subsequent evaluation, if source control had not been obtained, the patient was again formally debrided. This process was repeated every 24–48 hours until source control had been obtained. After confirming source control, all antibiotic agents were discontinued within 48 hours. Wound closure strategy was left to surgeon discretion and included various closure techniques as well as healing by secondary intention.
We included patients 18 years and older admitted to our emergency general surgery service with NSTI after 2018 over an 18-month period and compared them with historical controls. Patients were excluded if they were debrided at a referring facility, immune compromised, or died prior to obtaining source control. We also excluded patients who were continued on antibiotic agents beyond 48 hours after obtaining source control for reasons other than wound management such as positive blood cultures or pneumonia. Patient and disease characteristics as well as outcomes were evaluated.
The primary outcome was treatment failure, which was defined as need for further debridement of infected or necrotic tissue after termination of antibiotic agents or need to re-start antibiotic agents after stopping them for wound complications such as cellulitis or evolving wound infection. Secondary outcomes included the duration of antibiotic therapy after source control. We assessed whether or not the Necrotizing Infection Clinical Composite Endpoint (NICCE) had been achieved, which exists to define treatment success for NSTIs. To achieve NICCE, a patient must meet all four criteria, which include: being alive at 28 days, undergoing three or fewer debridements before hospital day 14, undergoing no amputation beyond the first debridement, and achieving a Modified Sequential Organ Failure Assessment (mSOFA) score ≤1 by hospital day 14 [9,10]. Comparison of proportions was calculated using χ2 test [11]. Comparison continuous variables was calculated using Mann-Whitney U test. A post-hoc power analysis performed to compare proportions was calculated using a two-sample non-inferiority calculator [12]. A p value <0.05 was considered significant. Analyses were performed with SPSS Statistics, version 26.0 (IBM Corp, Armonk, NY).
Results
We identified 173 immunocompetent patients diagnosed with NSTI who had not been debrided at a referring facility. We excluded 11 patients who had positive blood cultures and 11 patients who died prior to obtaining source control. One hundred fifty-one patients were included in the study, 119 admitted in the historical group (PRE) and 32 in the short duration group (POST) (Fig. 1). The PRE and POST groups were not different with respect to patient characteristics. Physiologic variables on admission were also not statistically different except for heart rate, where heart rate in the PRE group was slightly less than in POST group. Finally, comorbidities were not different between groups (Table 1).
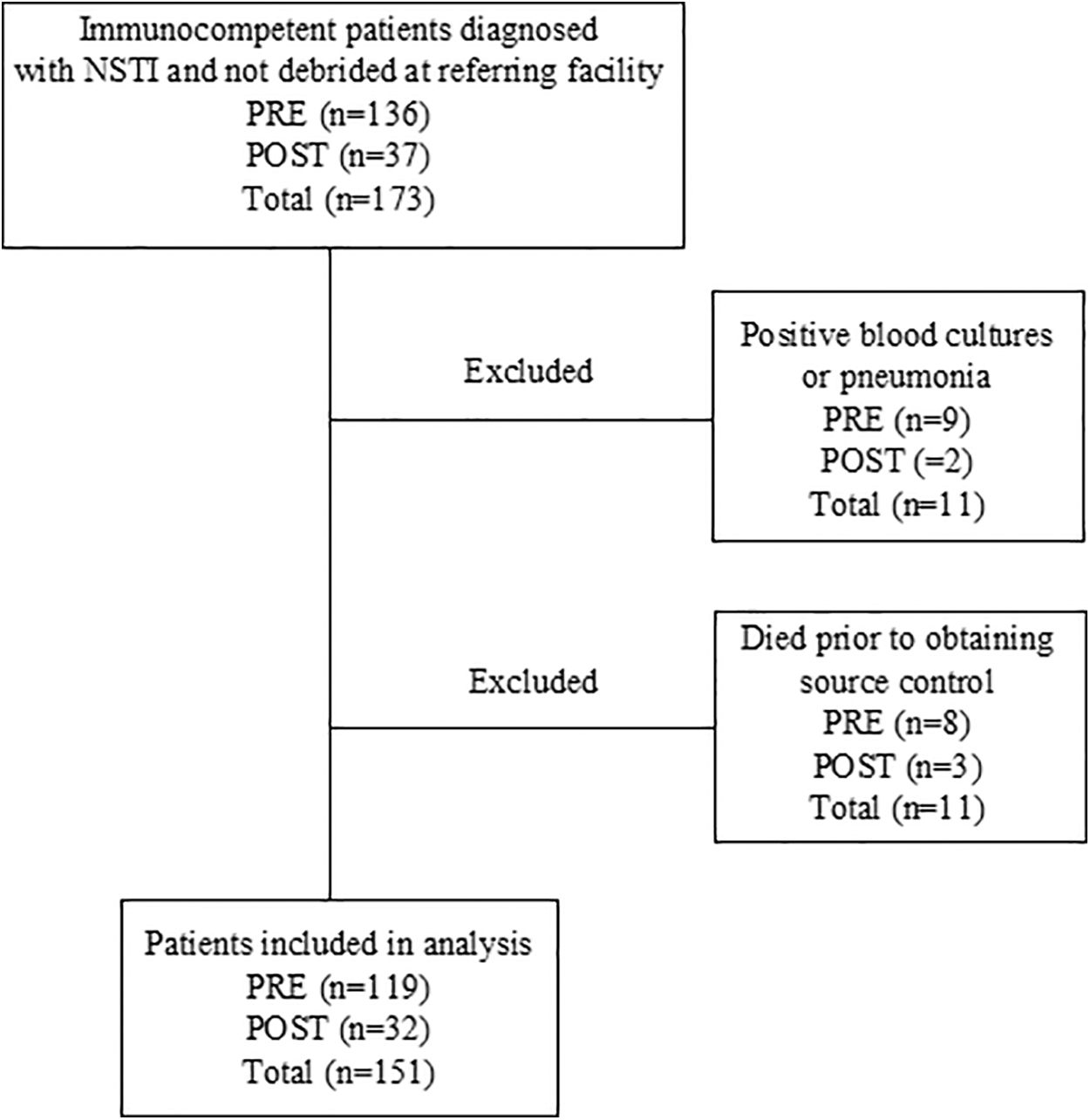
Flowchart of patient inclusion and exclusion criteria. NSTI = necrotizing soft tissue infection, PRE = patients admitted prior to January 2018 (when antibiotic duration was at the discretion of the attending surgeon, generally 7–10 days), POST = patients admitted after January 2018 (when all antibiotics were discontinued at 48 hours after obtaining source control unless otherwise indicated).
Demographics, Physiology, and Comorbidities of Patients with NSTI
SD = standard deviation; APACHE II = Acute Physiology and Chronic Health Evaluation II; WBC = white blood cell count; COPD = chronic obstructive pulmonary disease; BMI = body mass index.
Type 1 NSTIs were more common than type 2 NSTIs overall (85.8% vs. 14.2%, respectively), however, cultures were obtained at differing rates between the PRE and POST groups so it was not possible to compare culture results between the two time periods. The total number of debridements was not different between groups (1.7 ± 1 in PRE group vs. 2.1 ± 1.4 in POST; p = 0.07). Necrotizing soft-tissue infection anatomic location was variable but the majority of patients in both groups had Fournier gangrene, which was defined as an NSTI involving the genitals, perineum, or peri-anal areas. Such infections frequently extended to the thighs and buttocks. Amputation rates were not statistically different between the groups (5.9% in PRE group vs. 6.3% in POST; p = 0.93).
Treatment failure, our primary outcome, was the same between groups and occurred in the PRE group in 5.9% of patients compared to 6.3% in the POST group (p = 0.93). The median duration of antibiotic agents in the PRE group was 180.3 hours (interquartile range [IQR], 100.7–318.8) versus 48 hours (IQR, 32.3–100.8) in the POST group (p < 0.01). The percentage of patients who achieved NICCE in the PRE group was 85.7% (versus 84.4% in the POST group; p = 0.85). And finally, 30-day all-cause mortality in the PRE group was 6.7% (versus 6.3% in the POST group; p = 0.94) (Table 2). Because treatment failure was our primary end point and our results showed no difference between groups, we performed a post hoc power analysis. This analysis showed 99.3% power (1-β at 20% non-inferiority margin (δ) where α = 0.05.
Infection Characteristics, Treatment Variables, and Outcomes of Patients with NSTI
SD = standard deviaton; IQR = interquartile range; NICCE = Necrotizing Infection Clinical Composite Endpoint.
Discussion
The purpose of this project was to evaluate the safety of a short course (48 hours) of antibiotic agents in NSTI, and our hypothesis was that discontinuing antibiotic agents after a short course is safe in the treatment of NSTI. The mainstay of therapy for NSTIs, regardless of the location or type, is early surgical debridement and broad-spectrum antibiotic coverage. Although early debridement is clearly associated with better outcomes, there is no expert consensus regarding antibiotic duration. After January 2018, we began discontinuing all antibiotic agents at 48 hours after we had obtained source control, which we defined as the absence of cellulitis with a clean wound bed noted at subsequent wound examination. We then compared data we collected over an 18-month period with historical controls. We found that early discontinuation of antibiotic agents is safe and effective.
Necrotizing soft-tissue infection remains a condition with high morbidity and mortality and prompt and effective treatment is of paramount importance. Risk factors for mortality include age >75, multifocal NSTI, severe peripheral vascular disease, hospital-acquired infection, severe sepsis, and septic shock on hospital admission [13]. Early debridement (within 12 hours of presentation) greatly improves mortality [14,15], and it is also advised to return to the operating room to re-inspect the wound bed to confirm source control is obtained [16]. Bulger et al. [9] defined NICCE to define treatment success for NSTIs. To achieve NICCE, a patient must meet all four criteria, which include: being alive at 28 days, undergoing three or fewer debridements before hospital day 14, undergoing no amputation beyond the first debridement, and achieving a mSOFA score ≤1 by hospital day 14 [10]. Despite all these criteria, NICCE does not include antibiotic therapy goals. We hoped to better define the needed antibiotic duration after successful debridement. We became interested in this topic given our group's ongoing interest in the importance of antibiotic stewardship in the modern era of medicine when antimicrobial resistance to otherwise treatable infections is continually on the rise.
Of our groups, the PRE group was a historical control group that included patients with NSTI on the emergency general surgery service who did not meet exclusion criteria. The POST group were patients admitted after we changed our NSTI antibiotic protocol to discontinue all antibiotic agents 48 hours after we had obtained source control. Patient demographics were the same between groups, as was physiology on admission. Interestingly, a minority of patients in each group presented with signs of sepsis (systemic inflammatory response syndrome [SIRS] criteria met plus source of infection present) [17] at admission, which highlights the necessity to always maintain a high index of suspicion for NSTI whenever a new and painful wound is encountered in the emergency department. To the extent that bacteremia is a marker of more severe infection, we may have had lower than expected rates of severely ill patients in our study population. We excluded patients with positive blood cultures (since they were inevitably kept on antibiotic agents longer for bacteremia treatment) and those who died prior to obtaining source control, so our two groups may not have been as critically ill overall. Ultimately, nine patients with positive blood cultures were excluded in the PRE group and two were excluded in the POST group. Including these patients would have made it harder to parse out if antibiotic agents were continued beyond 48 hours for positive blood cultures or for the NSTI. Eight patients who died prior to source control were excluded in the PRE group and three were excluded in the POST group. Proportionally this was a similar number in each group based on size (hypothetically 6.2% vs. 8.6%), but our goal was to examine outcomes with differing duration of antibiotic therapy in those who survived.
We did not pre-operatively risk-stratify patients with the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC). The LRINEC, while once thought to be promising, has performed poorly in external validation as it has been shown to have a high false-positive rate when determining NSTI risk stratification in confirmed cases of cellulitis and a high false-negative rate in cases of confirmed NSTI [18]. Furthermore, our institution does not routinely collect C-reactive protein (CRP) values at admission, which is a significant part of calculating LRINEC scores. Of the remaining variables used in calculating LRINEC score that would indicate an increased risk for NSTI (white blood cell count ≥15 × 103/mcL, hemoglobin ≤13.5 g/dL, sodium ≤135 mmol/L, creatinine >1.6 mg/dL, and glucose >180 mmol/L), both groups of patients on average would have had an increased risk for NSTI in each of these categories (except for creatinine in the POST group), however, this risk would have been borderline without calculating a C-reactive protein.
The comorbidities we noted are consistent with standard literature. Of note, most patients in both the PRE and POST group had diabetes mellitus, and the second-highest comorbidity was hypertension requiring medication. On average, each group's average Charlson comorbidity index was between three and four with a wide standard deviation, suggesting an estimated overall 10-year survival of 53%–77% [19].
Treatment failure, our primary outcome, which was defined as need for further debridement after termination of antibiotic agents or need to restart antibiotic agents after stopping them for wound complications such as cellulitis or evolving wound infection was not different between groups. In the PRE group this was 5.9% and in the POST group it was 6.3%.
Necrotizing Infection Clinical Composite Endpoint was achieved at similar rates between the two groups, although the reasons for failure between the two were different. The PRE group included some patients who had amputations beyond the first debridement. In the POST group the two reasons for failure to achieve NICCE were deaths before 28 days and patients undergoing more than three debridements by hospital day 14.
Finally, mortality between the two groups was not different. Mortality in the PRE group was 6.7% and mortality in the POST group was 6.3%. This suggested that despite vastly different antibiotic durations (with the PRE median duration of 180.3 hours and IQR, 100.7–318.8), the POST group did not have an increased number of deaths. This should be reassuring to surgeons hesitant to adapt a shorter duration of antibiotic agents in the treatment of NSTIs.
There were limitations to our study. First, while this study was adequately powered, this assessment is based on a post-hoc power analysis showed which 99.3% power (1-β at 20% non-inferiority margin (δ) where α = 0.05. To achieve this level of power in non-inferiority testing we needed to decrease our non-inferiority margin to 20% to demonstrate non-inferiority between the outcomes of the POST group compared with the PRE group with regards to our study's primary outcome, treatment failure. To decrease this non-inferiority margin or to show superiority would require many more patients in the sample size. Second, between each group the patients were overall not statistically different but there were some subtle differences. The types of NSTIs encountered over time on the emergency general surgery service evolved to involve fewer lower extremity NSTIs and more Fournier gangrene.
Using historical controls does have the risk of inherent biases, especially selection bias and systematic difference among groups that can affect final outcome. Furthermore, as practice patterns change over time there is a risk of time trends bias. Finally, assessment bias and the lack of blinding may affect the subjective evaluation of endpoints. Although we cannot control everything, we tried to keep the same inclusion/exclusion criteria between the PRE and POST groups, attempted to minimize our reporting of data that were missing, and we performed a post hoc power analysis.
Conclusions
In summary, we conclude that 48 hours of antibiotic agents beyond NSTI source control is as safe and effective as a longer course. A randomized controlled trial with greater patient enrollment should be undertaken to better support our findings, and it would allow for the creation of a larger, more comprehensive database to further explore this disease and help define therapeutic guidelines for this problem. Other important clinical end points such as time to wound closure and long-term outcomes could be considered in future trials. We also suspect that since we have established safety with 48 hours of antibiotic agents in this study, using 24 hours or less of antibiotic agents after source control may be appropriate for a future study.
Funding Information
No funding was received.
Footnotes
Author Disclosure Statement
For all authors, no conflicts are declared.