
Abstract
Background:
Surgical site infections (SSIs) remain a challenge for the healthcare system. During the last 30 years, the literature has shown an increase of gram-negative bacterial strains in multiple infectious sites and that cephalosporins have replaced penicillin as the gold standard in peri-operative antibiotic prophylaxis. This study aims to examine the recent bacterial spectrum in orthopedic early SSIs and to compare it with a historical cohort.
Patients and Methods:
Patients in a level 1 trauma center with an SSI within six weeks after open fixation of a fracture were analyzed in two adjacent periods from 2007 to 2012 (data pool 1; DP1) and 2013 to 2017 (data pool 2; DP2), retrospectively. The detected microbiologic pathogens and the associated resistograms from both time periods were compared.
Results:
Six hundred eighty-one smear tests and respective pathogens from the wounds of 463 patients (mean age, 62.6 ± 20 years) with SSIs were analyzed. The following pathogens were found most frequent: Staphylococcus epidermidis (DP1, 20.6%; DP2, 26.3%), Staphylococcus aureus (DP1, 27.1%; DP2, 16.5%), Enterococcus faecalis (DP1, 13.7%; DP2, 11.1%), Bacillus sp. (DP1, 3.0%; DP2, 5.3%), Escherichia coli (DP1, 5.1%; DP2, 4.1%), Pseudomonas aeruginosa (DP1, 3.7%; DP2, 2.5%). In DP2, there were lower primary early infection rates with Staphylococcus aureus than in DP1 (p = 0.002). In DP2, Staphylococcus epidermidis showed an oxacillin resistance in 90.6% and an increased resistance (79.8%; p = 0.069) to several classes of antibiotic agents compared to DP1.
Conclusions:
No bacterial shift toward gram-negative species was observed in this investigation. However, Staphylococcus epidermidis showed an increased antibiotic resistance in the more recent patient cohort. The incidence of SSIs with Staphylococcus aureus decreased substantially.
Healthcare systems need to balance medical evidence-based decisions and optimize patient comfort versus effectiveness and resource efficiency [1]. Surgical site infections (SSIs) represent a particular challenge for physicians, patients, and the entire healthcare system. Physicians must develop and execute a made-to-measure treatment concept consisting of surgical, antibiotic, nursing, and physiotherapeutic therapy that is individually tailored to each patient but based on scientifically developed guidelines. The design of a successful treatment concept takes time and impacts human and financial resources. Surgical site infections can result in pain and anxiety and extend hospital stays [2]. Currently, the average infection rate for closed fractures ranges between 1% and 5% [3]. In open fractures, especially with a serious soft tissue defect, SSI occur in up to 30% of patients. [4,5] Wounds can be contaminated in the pre-, intra-, and post-operative setting. Pathogens proliferate most efficiently in devitalized tissues containing coagulated blood and necrotic bone [6]. Staphylococcus aureus, coagulase-negative staphylococci, and aerobic gram-negative bacteria are the most frequently detected pathogens in SSIs [7,8].
Patient-specific risk factors for an SSI predominantly described in the literature are advanced age, existence of manifest diabetes mellitus [9], arterial hypertension, nicotine abuse [10,11), and peripheral vascular disease [4,12–14]. Since the discovery of antibiotic agents and their incorporation into surgical infection prevention, the recommendations for peri-operative antibiotic prophylaxis have been modified. Until 1955, penicillin and its derivates were the most commonly chosen treatment for peri-operative antibiotic prophylaxis [15,16]. From 1974 onwards, cephalosporins replaced penicillins. For more than three decades, large clinical studies formed the foundation of peri-operative antibiotic prophylaxis, which nominated cephalosporins as the new gold standard [16,17]. However, this gold standard must be examined and verified on a regular basis because pathogen spectra and related antibiotic resistance change over time [18]. From 2007 to 2012, staphylococci represented the majority of all SSI pathogens with predominant Staphylococcus aureus resistant to methicillin. In subsequent years, multi-resistant gram-negative pathogens were detected with increasing frequency in different locations [12,19]. The aim of this study was to investigate the pathogen distribution after operative fracture fixation to validate the reported increase of gram-negative pathogens.
Patients and Methods
Patients
Retrospective microbiologic data of 463 patients from Leipzig University Hospital were analyzed during the time period from 2007 to 2012 (n = 303; data pool 1; DP1) and from 2013 to 2017 (n = 160, data pool 2; DP2). Between 2007 and 2017 the internal standard for peri-operative antibiotic prophylaxis was cefuroxime 1.5 g intravenous or, in cases of indigestibility or allergy against penicillin, clindamycin 600 mg intravenous. All positive microbiologic samples from trauma patients who had developed an SSI based on U.S. Centers for Disease Control and Prevention (CDC) criteria within 6 weeks after fracture fixation were included in this investigation [20].
Microbiology
The pathogen detection and minimal inhibitory concentration (MIC) value determination was conducted by the Institute for Medical Microbiology and Epidemiology of Infectious Diseases according to DIN EN ISO 20776-1. The assessment of the resistance value was performed in accordance with the European Committee on Antimicrobial Susceptibility Testing (EUCAST) 10.0 criteria [21] and each sample was incubated aerobically and anaerobically at 37°C for at least 48 hours according to previously published protocols [22].
Data evaluation
A database was established using Access 2018 (Microsoft, Seattle, WA). It included the following information: date of birth, gender, age, personal risk factors (obesity [body mass index >30 kg/m2], nicotine or alcohol abuse), admission and discharge dates, date of surgery, hospitalization (total, pre- and post-surgical), Orthopedic Trauma Association/Arbeitsgemeinschaft für Osteosynthesefragen (OTA/AO) classification of the fracture [23], whether the fracture was open or not, surgical procedure, administered peri-operative antibiosis, microbiologic data, cultured pathogens, and the corresponding MIC against antibiotic agents.
SPSS Statistics, version 25 (IBM Corp, Armonk, NY) was used for statistical analysis. Quantitative values were tested for normal distribution using Shapiro-Wilk test. Dichotomous data were compared using Pearson χ2 test (for n > 5) or Fisher exact test (for n < 5). For the detection of differences in means of continuous data, Student t-test was applied for normally distributed parameters and Mann-Whitney U test for non-normally distributed values. If applicable, results were Bonferroni-adjusted. In accordance with the specifications of the EUCAST, version 10.0, MIC values were divided into the groups sensitive and resistant and consecutively displayed graphically. Intermediate results were counted among the resistant pathogens due to our clinical standards.
Results
Study cohort
From a total of 463 patients (mean age, 14–98 years ±20.26) with SSI, 681 samples with one or more detected pathogens were documented and analyzed. Data acquisition was performed in two data periods, termed DP1 and DP2. In the first period (2007–2012) almost twice as many patients could be included as in the second period with nDP1 = 303 and nDP2 = 160.
In both cohorts, female patients were older than their male counterparts (p ≤ 0.001; DP1 mean male, 55.1 ± 18.7 years, female, 71.4 ± 18.7 years; DP2 mean male, 52.4 ± 18.5 years, female, 70.2 ± 18.2 years). Nicotine abuse (21.8%) and obesity (25.7%) were significantly (p < 0.0001) more frequent in cohort DP1 than in cohort DP2 (nicotine abuse, 7.5%; obesity, 9.4%). Alcohol abuse (DP1, 11.2%; DP2, 10.6%; p = 0.846) and diabetes mellitus (DP1, 26.1%; DP2, 26.9%; p = 0.852) were similarly distributed in both cohorts. The average length of hospital stay was 29.2 ± 24.3 days in cohort DP1 and 32.6 ± 3.3 days in cohort DP2 (p = 0.790; Table 1).
Overview of Patients Investigated in the Respective Time Periods DP1 and DP2
χ2 test was performed for n > 5 patients or Fisher exact test for n < 5. Mann-Whitney U test was performed for mean time of stay and age.
DP1 = period between 2007 and 2012; DP2 = period between 2013 and 2017; SD = standard deviation.
Most pathogens in both time periods were identified in wounds of patients who underwent surgery for fractures of the lower extremity (femur: DP1, n = 139; 32.0%; DP2, n = 69; 28.4%; lower leg: DP1, n = 93; 21.4%, DP2, n = 58; 23.9%; Table 2). There were 36 open and 274 closed fractures in DP1 compared with 32 open and 128 closed fractures in DP2.
Respective AO Regions of Fracture and Their Prevalence in DP1 and DP2
AO = classification of the German Arbeitgemeinschaft für Osteosynthesefragen; DP1 = period between 2007 and 2012; DP2 = period between 2013 and 2017; SD = standard deviation.
Pathogen spectrum
A total of 678 different pathogens were cultivated. Among those, the most frequent were Staphylococcus epidermidis (22.6%; 153), Staphylococcus aureus (23.3%; 158), Enterococcus faecalis (12.7% 86), Bacillus sp. (3.8%; 26), and Escherichia coli (4.7%; 32), which collectively accounted for 67.1% of the total pathogen spectrum (Figs. 1 and 2). One hundred thirty-seven (19.9%) of the 678 pathogens were gram-negative. Three hundred thirty-one samples (48.8%) were found to carry a single pathogen and 347 (51.2%), mixed infections (200/435 DP1; 147/243 DP2). Staphylococcus aureus was found to be more common in the lower body region than in the remaining regions (p < 0.0001). Staphylococcus epidermidis caused more infections of the upper leg (p = 0.002).

Pie chart showing the respective pathogen prevalence during data pool 1 (DP1).
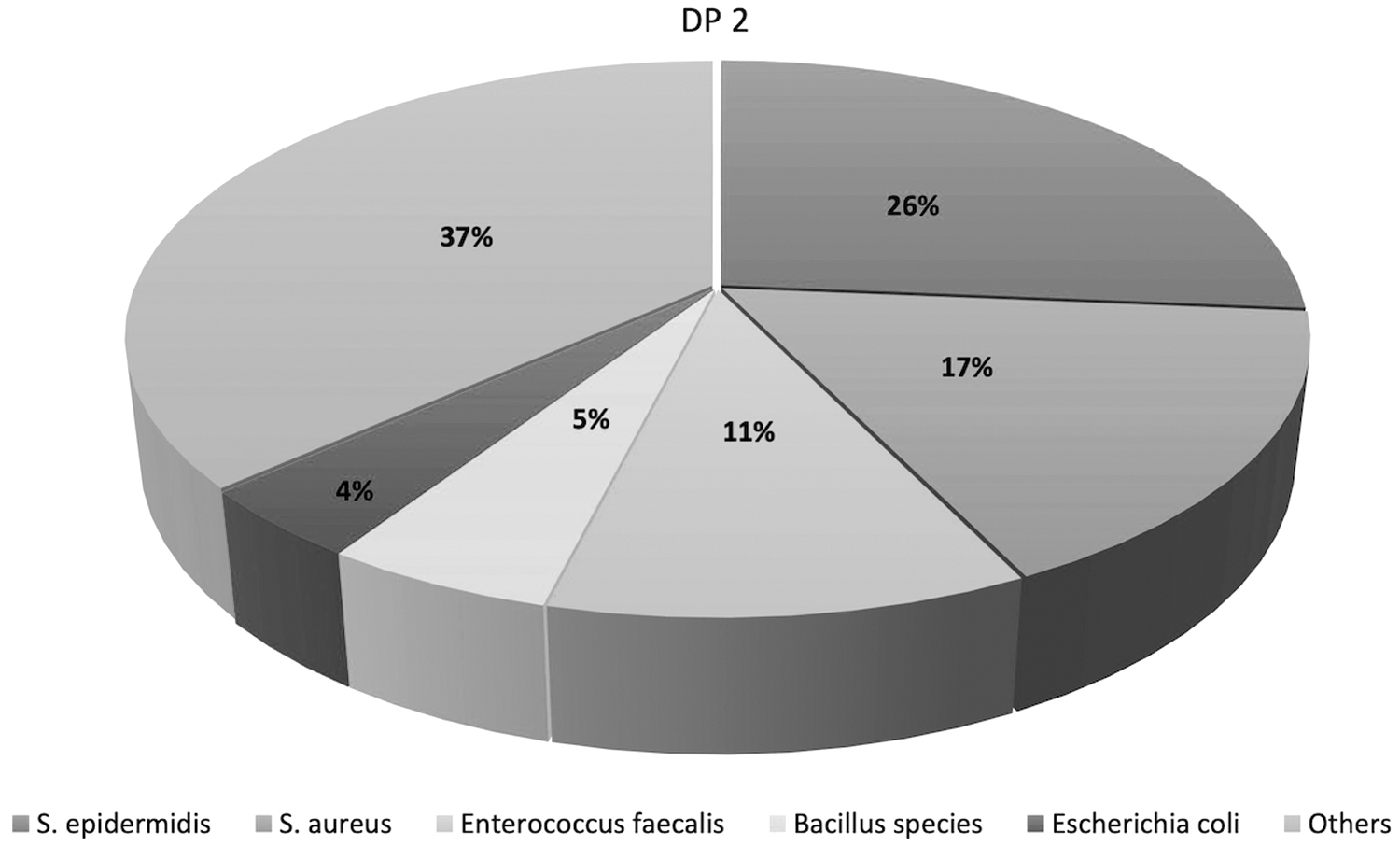
Pie chart showing the respective pathogen prevalence during data pool 2 (DP2).
Multi-resistant pathogens
Methicillin-resistant Staphylococcus aureus occurred in DP1 in 12.9% and in DP2 in 5.0% of the cases (p = 0.002). Staphylococcus epidermidis showed a 90.5% resistance to cefuroxime in DP2 in comparison to 79.8% resistance in DP1 (p = 0,069; Figs. 3 and 4). The gram-negative pathogen spectrum did not show multi-drug resistance for Escherichia coli and Pseudomonas aeruginosa in DP2 (DP1 multi-drug–resistant Escherichia coli, 18.2%; metallo-β-lactamase-producing [MBL] Pseudomonas aeruginosa, 6.25%). Enterococci were vancomycin-resistant in 3% of the cases in DP1 and DP2. The three most frequent pathogens in both cohorts were Staphylococcus aureus (DP1, 27.1%; DP2, 16.5%), Staphylococcus epidermidis (DP1, 20.6%; DP2, 26.3%), and Enterococcus faecalis (DP1, 13.7%; DP2, 11.1%) (Figs. 1 and 2).
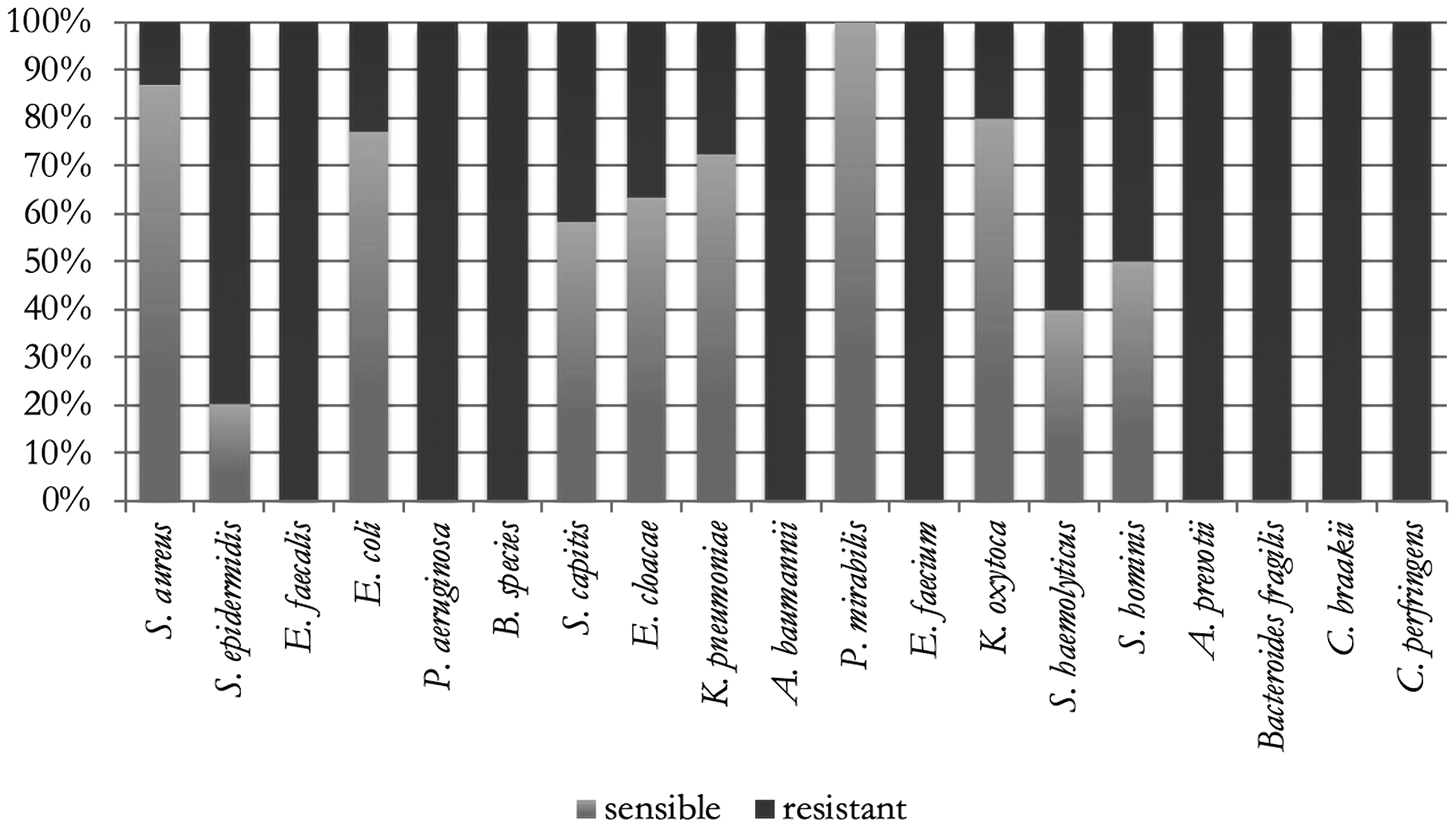
Bar chart showing the respective bacteria and their susceptibility to cefuroxime during data pool 1 (DP1).
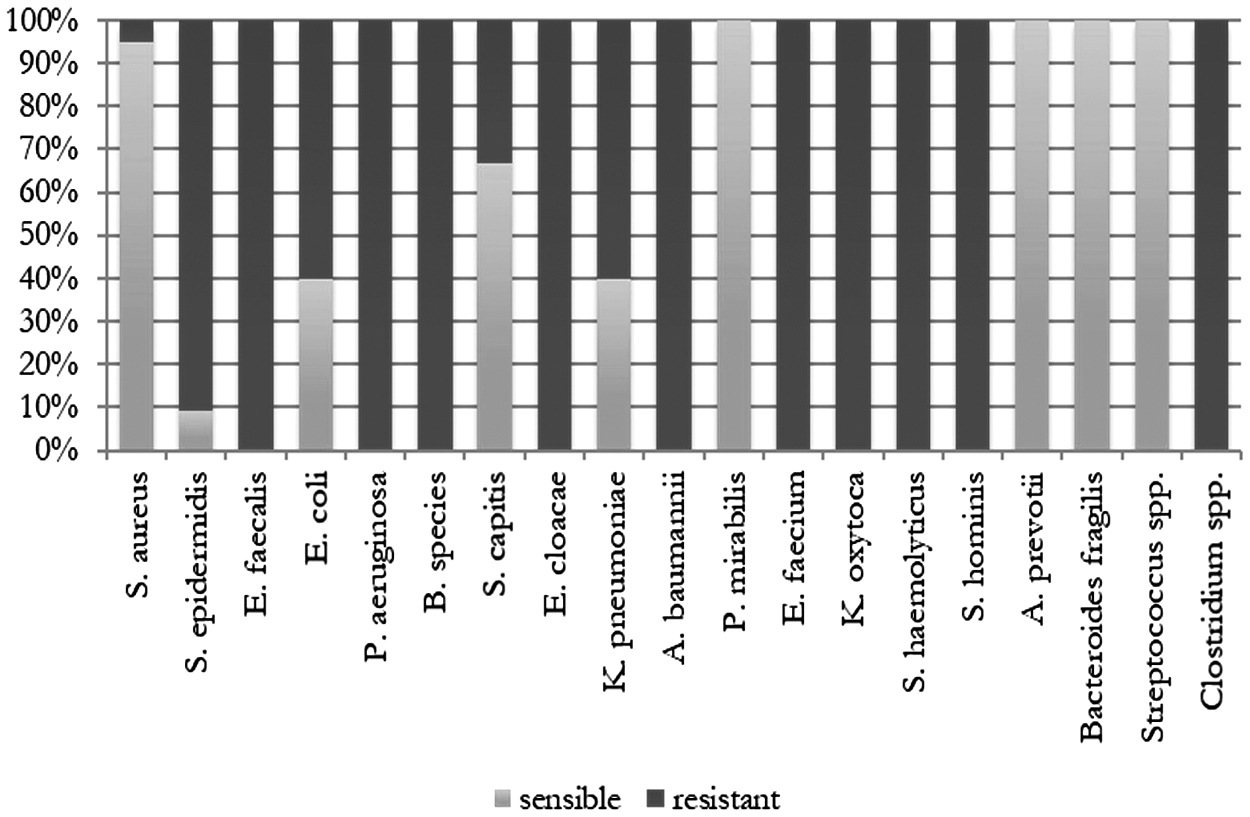
Bar chart showing the respective bacteria and their susceptibility to cefuroxime during data pool 2 (DP2).
Discussion
The aim of this study was to investigate whether there has been a change in pathogen distribution toward gram-negative pathogens in trauma surgery during recent years. Two successive time periods, DP1 (2007–2012) and DP2 (2013–2017), were examined. Patients who developed an SSI within six weeks after open reduction and internal fixation of a traumatic fracture were included. The microbiologic data analyzed for this purpose was obtained from swabs and samples, which were obtained intra-operatively.
Most common pathogens in both periods were Staphylococcus aureus (DP1, 27.1%; DP2, 16.5%), Staphylococcus epidermidis (DP1, 20.6%; DP2, 26.3%), and Enterococcus faecalis (DP1, 13.7%; DP2, 11.1%). In DP1 (2007 to 2012), significantly more site infections with Staphylococcus aureus occurred than in DP2. The proportion of SSI caused by Staphylococcus epidermidis did not increase significantly. Staphylococcus aureus was found to be more common in the lower extremities than in the remaining regions and Staphylococcus epidermidis caused more infections of the thigh.
For many years, published data suggested that post-operative infection rates declined internationally and have now seemed to remain on a plateau for the last few years [24,25]. This can be partly attributed to updated hygiene concepts [26] that have been established in pre-, peri-, and post-operative concepts. Data pool 2 included fewer patients than DP1. This can be partly attributed to an updated hygiene concept (especially rectal smears for multi-resistant pathogens [MRE] detection and early patient isolation), which was introduced at the authors' institution in 2011 after an increased incidence of a highly virulent, multi-drug–resistant gram-negative pathogen [27]. Among other measures, this led to the implementation of the new antibiotic surveillance concept beginning in 2013. The new concept implemented improved hygiene strategies (e.g., multi-drug-resistant pathogens [MRD] screening, isolation concepts) and revised the antibiotic scheme [28]. In the past, early infections mostly showed evidence of highly virulent Staphylococcus aureus and late infections of less virulent Staphylococcus epidermidis [29].
Our data from the past 10 years show that not the entire pathogen spectrum but the prevalence of individual species has changed substantially. Staphylococcus epidermidis is found more frequently in SSIs, whereas strains of Staphylococcus aureus were found. In this context, it should be mentioned that Staphylococcus epidermidis has a clear selection advantage under cefuroxime therapy because of the more frequent resistance to methicillin [30,31]. Only two methicillin-resistant Staphylococcus aureus (MRSA) strains and no vancomycin-resistant Enterococcus sp. strains could be detected in DP2. In DP1, multi-drug–resistant pathogens declined with time. This decrease of MRSA has been described previously in the literature [25,26,32]. The fraction of gram-negative pathogens was 21.8% in DP2, and thus, did not differ significantly from the fraction of gram-negative pathogens in DP1 (22.1%).
We attribute the low influence of gram-negative infections on both groups to the fact that an infection of this bacterial spectrum is found rather less frequently in trauma surgery cases because the pathogens are more likely to be found in the intestinal flora. The relevant bacteria with high occurrence are the gram-positive germs, which are found especially on the skin flora of humans [33].
Outside the dermatologic pathogen spectrum, however, several meta-analyses could prove an increase in gram-negative pathogen strains [12,25,26,34,35]. In the period between 2007 and 2012, a resistance against cefuroxime was detected in 70% of the cases versus 90% in the period between 2013 and 2017. In the 1970s, Staphylococcus epidermidis strains were still almost 100% sensitive [16]. This can be explained by the civilization-induced development of resistance. Today, almost every species has had contact with an antibiotic at some point, which has resulted in the development of resistances over the years [16,36,37].
In 2016, Probest et al. [38] compared implant infections from over a decade and found not only a shift in the pathogen spectrum from Staphylococcus aureus to Staphylococcus epidermidis and Enterococcus sp., but also an increasing resistance to cefuroxime during this period. They reported that between 2005 and 2009, 33% of SSIs after fracture fixation were associated with cefuroxime-resistant pathogens versus 80% in a reference cohort from 2010 to 2014. Because Staphylococcus epidermidis was resistant in 90.5%, therefore representing a major part of multi-drug–resistant pathogens, increased attention needs to be paid to this frequent occurrence and the resistance situation with respect to current peri-operative antibiotic prophylaxis [38].
Once interpreted as a commensal when found in wound swabs, Staphylococcus epidermidis has changed toward a serious pathogen in SSIs. It has collected a variety of mechanisms, not only to settle down near medical implants, but to form the pathway for a more dangerous potential combination of pathogens, namely the biofilm. The ability to form biofilm by itself, the production of exoenzymes and the virulence gene reservoir function, an ability to exchange immune and antibiotic resistance factors to other bacterial species makes Staphylococcus epidermidis an increasing pathogen in SSI today and in the near future [39]. Surgical site infection caused by Enterococcus faecalis and Pseudomonas aeroginosa [40] mostly show a high resistance to cephalosporins and some other β-lactams such as isoxazolylpenicillins (e.g., oxacillin) because of the so-called penicillin binding protein (PBP). The PBP is a specific enzyme produced by several bacteria, which is involved in murein synthesis and is also capable of binding penicillins and other β-lactam antibiotic agents [41]. Overall, we were able to consider a 10-year period, which was only interrupted by a 10-month exception because of missing MIC values.
The findings showed an increase in Staphylococcus epidermidis isolates and a decrease in Staphylococcus aureus isolates. Patients who are treated post-trauma have accompanying soft tissue damage, vascular damage, or perfusion failure in the traumatized tissue more often than the orthopedic elective patient. These two accompanying injury patterns impede the healing of the bone and the involved soft tissues. The difference to open fractures is even greater, as they additionally provide a considerably larger surface for pathogens to invade [5].
Conclusions
Our findings suggest an increase in methicillin-resistant Staphylococcus epidermidis (MRSE), however, no overall increase of gram-negative pathogens was detected, which is contrary to recent literature findings. The peri-operative antibiotic prophylaxis with third-generation cephalosporins is the most commonly performed approach to prevent post-operative wound infection. However, the increased occurrence of MRSE strains leads to the problem that we cannot cover this group of pathogens with cephalosporins.
In the future, more studies, preferably prospective studies, will be needed to investigate further the development of resistance and the pathogen spectrum to achieve the best possible antibiotic prophylaxis and to reduce the number of post-operative wound infections to a minimum.
Footnotes
Funding Information
This study received no funding.
Author Disclosure Statement
None of the authors listed have any commercial associations or financial disclosures that might pose or create a conflict of interest with the methods applied or results presented in the article. This study was reviewed by the Ethics Committee of the University of Leipzig under file number 349/17-ek and approved without restriction on October 11, 2017.