
Abstract
To the Editor:
Actinomyces are gram-positive facultative anaerobic filamentous bacilli commensal to orodigestive and urogenital tracts. Actinomyces turicensis infections are rare and reported in both immunocompromised and immunocompetent adults [1]. Necrotizing soft tissue infections (NSTIs) caused by Actinomyces turicensis are rare, and thus clinicians should report them. This is the first report of Actinomyces turicensis implicated in Fournier gangrene.
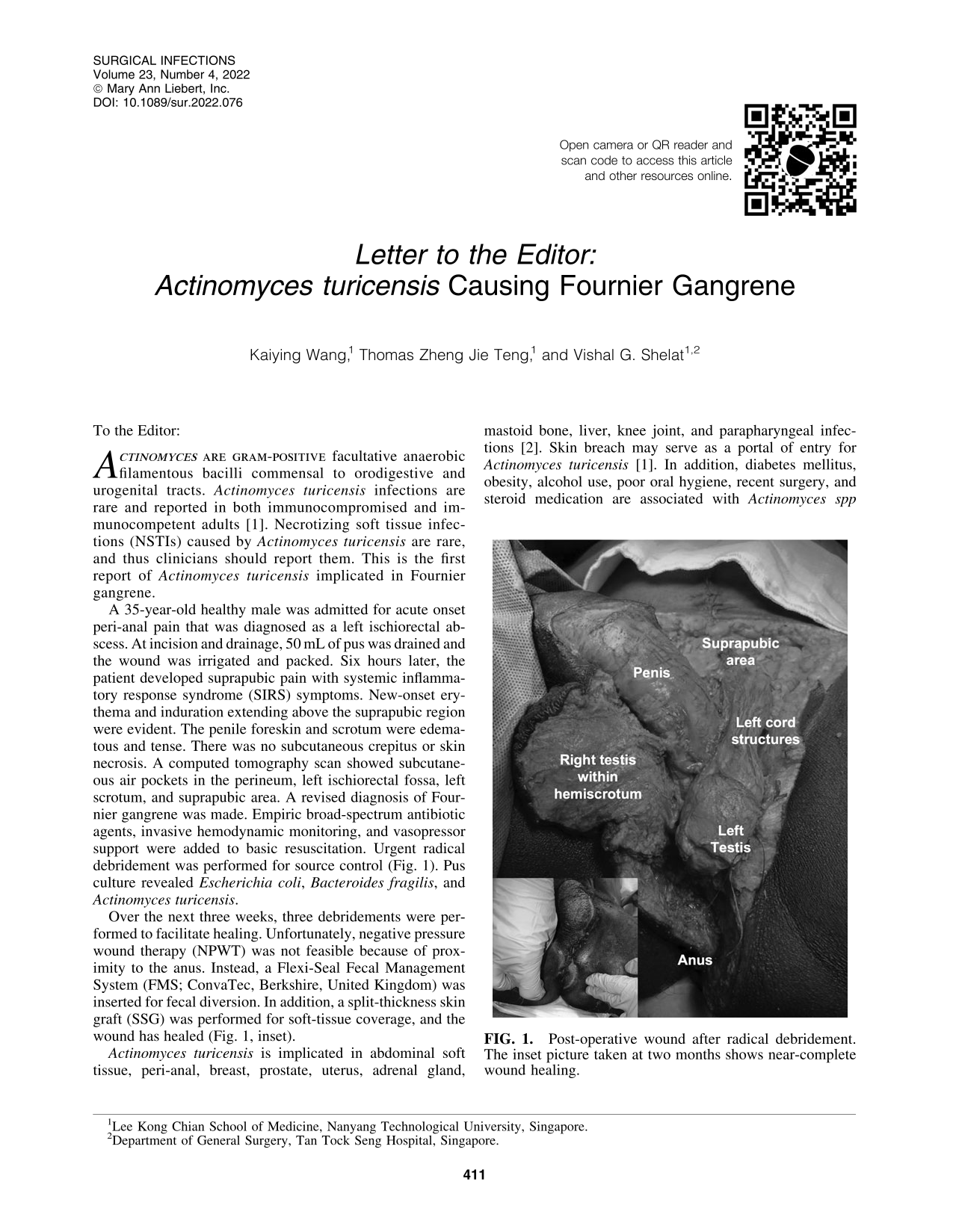
A 35-year-old healthy male was admitted for acute onset peri-anal pain that was diagnosed as a left ischiorectal abscess. At incision and drainage, 50 mL of pus was drained and the wound was irrigated and packed. Six hours later, the patient developed suprapubic pain with systemic inflammatory response syndrome (SIRS) symptoms. New-onset erythema and induration extending above the suprapubic region were evident. The penile foreskin and scrotum were edematous and tense. There was no subcutaneous crepitus or skin necrosis. A computed tomography scan showed subcutaneous air pockets in the perineum, left ischiorectal fossa, left scrotum, and suprapubic area. A revised diagnosis of Fournier gangrene was made. Empiric broad-spectrum antibiotic agents, invasive hemodynamic monitoring, and vasopressor support were added to basic resuscitation. Urgent radical debridement was performed for source control (Fig. 1). Pus culture revealed Escherichia coli, Bacteroides fragilis, and Actinomyces turicensis.

Post-operative wound after radical debridement. The inset picture taken at two months shows near-complete wound healing.
Over the next three weeks, three debridements were performed to facilitate healing. Unfortunately, negative pressure wound therapy (NPWT) was not feasible because of proximity to the anus. Instead, a Flexi-Seal Fecal Management System (FMS; ConvaTec, Berkshire, United Kingdom) was inserted for fecal diversion. In addition, a split-thickness skin graft (SSG) was performed for soft-tissue coverage, and the wound has healed (Fig. 1, inset).
Actinomyces turicensis is implicated in abdominal soft tissue, peri-anal, breast, prostate, uterus, adrenal gland, mastoid bone, liver, knee joint, and parapharyngeal infections [2]. Skin breach may serve as a portal of entry for Actinomyces turicensis [1]. In addition, diabetes mellitus, obesity, alcohol use, poor oral hygiene, recent surgery, and steroid medication are associated with Actinomyces spp infection [2]. A recent review of peri-anal Actinomyces spp. Infection that included 53 patients, reported that it is three times more common in females and has a 39.6% chance of mixed growth [3]. However, our patient did not have any risk factors.
Necrotizing soft tissue infection involving external genitalia and perineum is almost always polymicrobial and bears the eponym of Fournier gangrene. It is broadly grouped as urogenital or anorectal, and rapid hemodynamic compromise with organ dysfunction is a hallmark [2]. Therefore, urgent source control with radical debridement is critical for good clinical outcomes [4].
Culture-directed antibiotic therapy is integral, and we prescribed a three-week course of intravenous carbapenems. In addition, post-operative wound care is essential for optimal wound healing to facilitate definite wound coverage by reconstructive surgery [5]. In our patient, NPWT was attempted but was not feasible, and thus we resorted to simple wound dressings and fecal diversion using Flexi-Seal FMS. We managed to avoid diverting colostomy.
In conclusion, Fournier gangrene caused by Actinomyces turicensis is rare. Early diagnosis, appropriate resuscitation, urgent source control, high-quality post-operative wound care, and early reconstructive surgery are integral for good outcomes.