
Abstract

To the Editor:
F
A 44-year-old female presented to the department of otorhinolaryngology with right nasal congestion of one-month duration. She denied history of infectious diseases. Prior to this admission, she was suspected of nasopharyngeal cancer. Nasal endoscopy showed her nasal septum was deflected to the right, nasal ridges were visible, the right inferior turbinate was partly attached to the nasal septum, bilateral inferior turbinates were swollen, smooth new creature could be seen on the top wall of the nasopharynx, and white pseudomembranes could be seen on the surface of the new creature that can cause bleeding when touched.
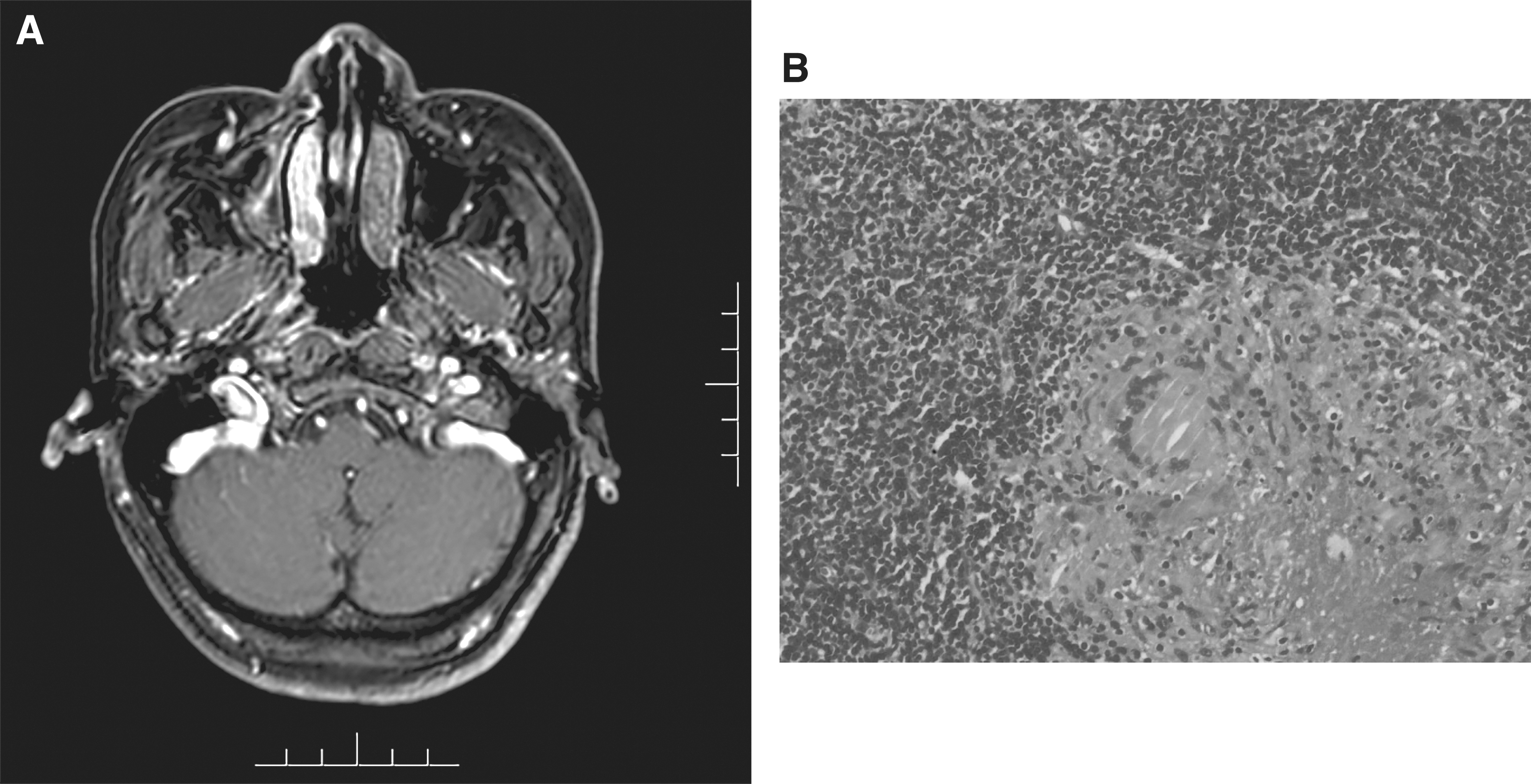
Human immunodeficiency virus (HIV)-1 antibody was positive, magnetic resonance imaging (MRI) showed the mucosa on the right side of the nasopharynx was slightly thickened, enhanced scan showed homogeneous enhancement (Fig. 1A). The patient underwent a biopsy of the new creatures in the right nasopharynx, histopathology showed chronic inflammation with large amounts of inflammatory exudate necrosis and granuloma with caseous necrosis (Fig. 1B), Mycobacterium tuberculosis DNA detection was positive.
(
These findings supported the diagnosis of nasal TB and acquired immune deficiency syndrome (AIDS). The patient was transferred to the department of infectious diseases for treatment. Her HIV viral load was 20,100 copies/mL, CD4+ T cells were 355 cells/mm3, chest and abdominal computed tomography were normal, and no evidence of TB was found in other organs. The patient was given lamivudine, tenfovir, and efavirenz for antiretroviral therapy. The anti-tuberculosis treatment regimen was rifampicin (R), isoniazid (H), pyrazinamide (Z), and ethambutol (E) for two months and then HR for four months at which time she had no ongoing symptoms. At a six-month follow-up, her nasal TB was cured, and her CD4+ T cells were 452 cells/mm3.
The rarity of nasal TB can be explained by the protective function provided by the bactericidal properties of the nasal secretions, the ciliary action of the nasalmucosa, and the protective mechanisms of nasal vibrissae [3]. The differential diagnosis for nasal TB includes carcinoma, fungal infection, Wegner granulomatosis, sarcoidosis, rhinoscleroma, and leprosy. Imaging examination of the nose may not distinguish between benign and malignant lesions, so biopsy of the pathologic tissue and Mycobacterium tuberculosis-related tests should all be strongly recommended.
The treatment of nasal TB usually follows the general guidelines established for the treatment of extrapulmonary TB; surgery is not required when the disease is localized in the nose [4]. In case of significant nasal obstruction, reconstructive plastic surgery for perforation of the nasal septum may be required [5]. This case showed that the possibility of nasal TB should be kept in mind during the differential diagnosis of patients with chronic nasal lesions, particularly in HIV-infected individuals.