
Abstract
Background:
Infection is a common complication after tissue expander placement. Previously, we have demonstrated that a single dose of peri-operative antibiotic agents is sufficient to achieve an adequately low infection rate for implant exchange procedures. In this follow-up study, we evaluate the efficacy of a similar course of antibiotic prophylaxis regimen for tissue expander placement procedures.
Patients and Methods:
This is a retrospective study of patients who underwent mastectomy and immediate tissue expander-based reconstruction from July 2011 to April 2021. The primary outcome was breast infection. Student t-test and χ 2 tests were used to compare cohorts and complication rates. Multivariable regression analysis was used to identify risk factors for infection.
Results:
In a 10-year-period, 307 patients (529 breasts) underwent immediate tissue expander reconstruction. Infection occurred in 80 breasts (15.1%). There was no difference in infection rates across pre-pectoral, dual plane, or total submuscular approaches (p = 0.705). Once infection occurred, patients in the dual-plane cohort were more likely to be admitted for intravenous antibiotic treatment (p = 0.007). On multivariable regression analysis, mastectomy skin flap necrosis (p = 0.002), post-operative radiation therapy (p = 0.007), and active smoking (p = 0.007) were significant risk factors for subsequent infection.
Conclusions:
A short course of peri-operative antibiotic prophylaxis is sufficient for an adequately low infection rate. Mastectomy skin flap necrosis, post-operative radiation therapy, and active smoking placed patients at higher risk for infection. Our results advocate for the conservative use of antibiotic agents while achieving an adequate low infection rate.
Introduced in the 1960s, prosthetic implant-based breast reconstruction was established as a single-stage process in which permanent implants were placed at the time of the reconstruction. It has since then evolved into a multi-stage process, consisting of tissue expanders during initial reconstruction before the final exchange for permanent implants. Two-stage reconstruction with tissue expanders offers many benefits, such as skin envelope stretching and avoidance of wound contracture while allowing patients direct control over the size of their reconstruction. 1
In a two-stage reconstruction, the tissue expander can be placed using a pre-pectoral, dual-plane, or total submuscular approach. Although pre-pectoral breast reconstruction was the original mainstay approach, the frequency of complications, including implant extrusion, caused a major shift toward the submuscular approach.2,3 With this new approach, either dual-plane or total submuscular, the additional layer of muscular coverage was able to alleviate many of the consequences that came with placement in the pre-pectoral plane. Despite the improvements, submuscular breast reconstruction is not without its drawbacks, such as pectoralis muscle repositioning, increased post-operative pain, lengthened recovery time, and animation deformities. 4
Over the past 30 years, several improvements and technological advancements have attempted to address issues specific to each reconstructive plane. 5 However, even with these efforts, infection still remains one of the more challenging complications to manage. Common symptoms include breast pain, swelling, erythema, and fever. If not treated properly, infection can lead to poor wound healing, re-operation, and need for explantation. Increased healthcare expenditure is also a major concern, with one study estimating infection-related costs to be almost $4,100 per patient in the United States. 6
According to the U.S. Centers for Disease Control and the Surgical Care Improvement Project, for a clean surgical case such as breast surgery, the antibiotic recommendation is a maximum of 24 hours of peri-operative antibiotic agents. 7 Although breast surgery is considered a clean surgical case, rates of infection after tissue expander-based reconstruction have been documented to be as high as 35%, unlike the typical 3%–4% during the second-stage implant exchange procedure.8–13 Because of these markedly higher rates of infection, most plastic surgeons provide prolonged antibiotic regimens after tissue expander-based reconstructions. In a 2009 survey study, 72% of plastic surgeons prescribed an antibiotic regimen continuing for a least one week after breast reconstruction or until drain removal. 14
One of the major concerns of prolonged antibiotic use is organism resistance and more severe infections. 15 Antimicrobial resistance can lead to a delay in administration of effective antibiotic agents resulting in prolonged infections. Moreover, these resistant organisms necessitate the use of more potent and toxic drugs because of their side-effect profiles. In a randomized controlled trial conducted by Phillips et al., 16 individuals who received antibiotic agents until drain removal were found to have higher rates of requiring intravenous antibiotic agents and tissue expander loss compared with individuals receiving only 24 hours of antibiotic agents.
There is a contradiction between the continued trend of prolonged antibiotic regimens post-discharge and the evidence in the literature suggesting the lack of beneficial effects. In this study, our first aim is to investigate the utility of a short 24-hour course of peri-operative antibiotic agents for immediate tissue expander-based reconstruction. In addition, we aim to analyze post-operative complications, particularly infection rates and necrosis, across the three reconstructive planes, and identify risk factors for infection.
Patients and Methods
This study was approved by the Weill Cornell Medicine Institutional Review Board as a retrospective review of a consecutive series of adult female patients who underwent mastectomy and immediate reconstruction with tissue expanders from July 2011 to May 2021 at a single tertiary care institution by the senior author. This cohort included all patients who underwent tissue expander placement as the first stage of reconstruction, followed either by implants or delayed autologous reconstruction.
Electronic medical records were reviewed for patient demographics, comorbidities, and smoking status. Each patient's oncologic regimen was reviewed, including timing of chemotherapy, radiation therapy, and hormone receptor blocker therapy. Special emphasis was placed on the plane of reconstruction: pre-pectoral, dual plane, or total submuscular. Peri-operative and post-operative antibiotic data were also extracted. Peri-operative antibiotic use was defined as antibiotic agents administered from start of surgery up to 24 hours post-operatively. Post-operative antibiotic use was defined as antibiotic agents given after 24 hours from start of procedure as either prophylactic or therapeutic doses.
The primary clinical outcomes of interest were breast or tissue expander infection and subsequent explantation prior to second-stage reconstruction. Breast infection was defined as erythema or other signs of surgical site infection requiring intervention such as therapeutic antibiotic agents, drainage, operative washout, or explant. Mastectomy skin flap necrosis is defined as any skin compromise requiring any topical wound care or excision post-operatively. Our definition included both partial-thickness and full-thickness necrosis. Infections occurring in the setting of concurrent skin necrosis is defined as cases in which the infection occurred either along with or after skin necrosis has demarcated.
Statistical analysis
All statistical analyses were performed in R Version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were used to characterize the patient population. Patients were separated into three cohorts based on reconstructive planes: pre-pectoral, dual plane, or total submuscular. Kruskal-Wallis and Student t-tests were used to compare quantitative variables across the three cohorts. Pearson χ 2 test, or Fisher exact test (if n < 5), were used for categorical variables such as breast infection and explantation rates. Univariable regression analysis was performed for all variables to compute associations between independent variables and outcomes of interest.
Variables found significant on univariable regression analysis were included in multivariable regression analysis. A p value of <0.05 was used as the threshold to determine statistical significance.
Results
Between July 2011 and May 2021, 307 patients (529 breasts) who underwent immediate first-stage reconstruction using tissue expanders were included in this study. Immediately prior to the first surgical incision, all patients received a single 2-g dose of cefazolin. In cases of penicillin allergy, dose-equivalent clindamycin or gentamicin was administered instead. All operative times were under five hours, therefore no peri-operative re-dosings were given. Based on risk profile, a select few patients received additional 2-g doses every eight hours post-operatively. These criteria included prior history of surgical site infection, immunocompromise (including neoadjuvant therapies), and surgical course, such as thinned mastectomy skin flaps. No patients received antibiotic agents beyond 24 hours since start of procedure and no additional doses were prescribed at discharge.
The mean patient age was 50 years (range, 22–83 years) and the mean body mass index was 24.5 kg/m 2 (range, 16.3–63.3 kg/m 2 ). Fifty-three patients had hypertension and 12 patients had diabetes mellitus, and 11 patients were active smokers. Sixty-three patients received neoadjuvant chemotherapy, 87 patients received adjuvant chemotherapy, and 57 patients received post-operative radiation therapy. All adjuvant treatments were begun approximately three weeks post-operatively.
Of the 529 breasts, 226 breasts (42.7%) were reconstructed using the pre-pectoral approach, 286 breasts (54.0%) were reconstructed using the dual-plane approach, and 17 breasts (3.2%) were reconstructed using the total submuscular approach. The patients in each of the three cohorts were comparable in age, body mass index, smoking status, medical comorbidities, and oncologic regimen (p > 0.05; Table 1).
Patient Characteristics Across Reconstructive Planes
SD = standard deviation; BMI = body mass index.
Infection rate
Of the 529 reconstructions, 80 breasts (15.1%) developed an infection, and mastectomy skin flap necrosis occurred in 82 breasts (15.6%). Of note, in the 447 breasts without concurrent skin necrosis, infection occurred in 56 breasts (12.5%). There was no statistically significant difference in breast infection rates across the three reconstructive planes: 35 infected breasts (15.5%) in the pre-pectoral plane, 44 infected breasts (15.4%) in the dual-plane approach, and one breast (5.9%) in the total submuscular approach. Similarly, mastectomy skin flap necrosis occurred in similar rates across the three cohorts: 38 breasts (16.8%) in the pre-pectoral cohort, 42 breasts (14.7%) in the dual-plane cohort, and two breasts (11.8%) in the total submuscular cohort (Table 1).
On culture, coagulase-negative staphylococcus and Staphylococcus aureus (methicillin-sensitive) were the most common organisms (Table 2). Of the 67 patients who were infected, one patient in the dual-plane cohort was lost to follow-up after infection and 25 patients (37.3%) were admitted for intravenous antibiotic treatment. Patients in the dual-plane cohort had substantially higher rates of hospital admission for intravenous antibiotic treatment (53.7%; p = 0.007; Fig. 1). Explantation rates across the three cohorts were comparable (p = 0.349).
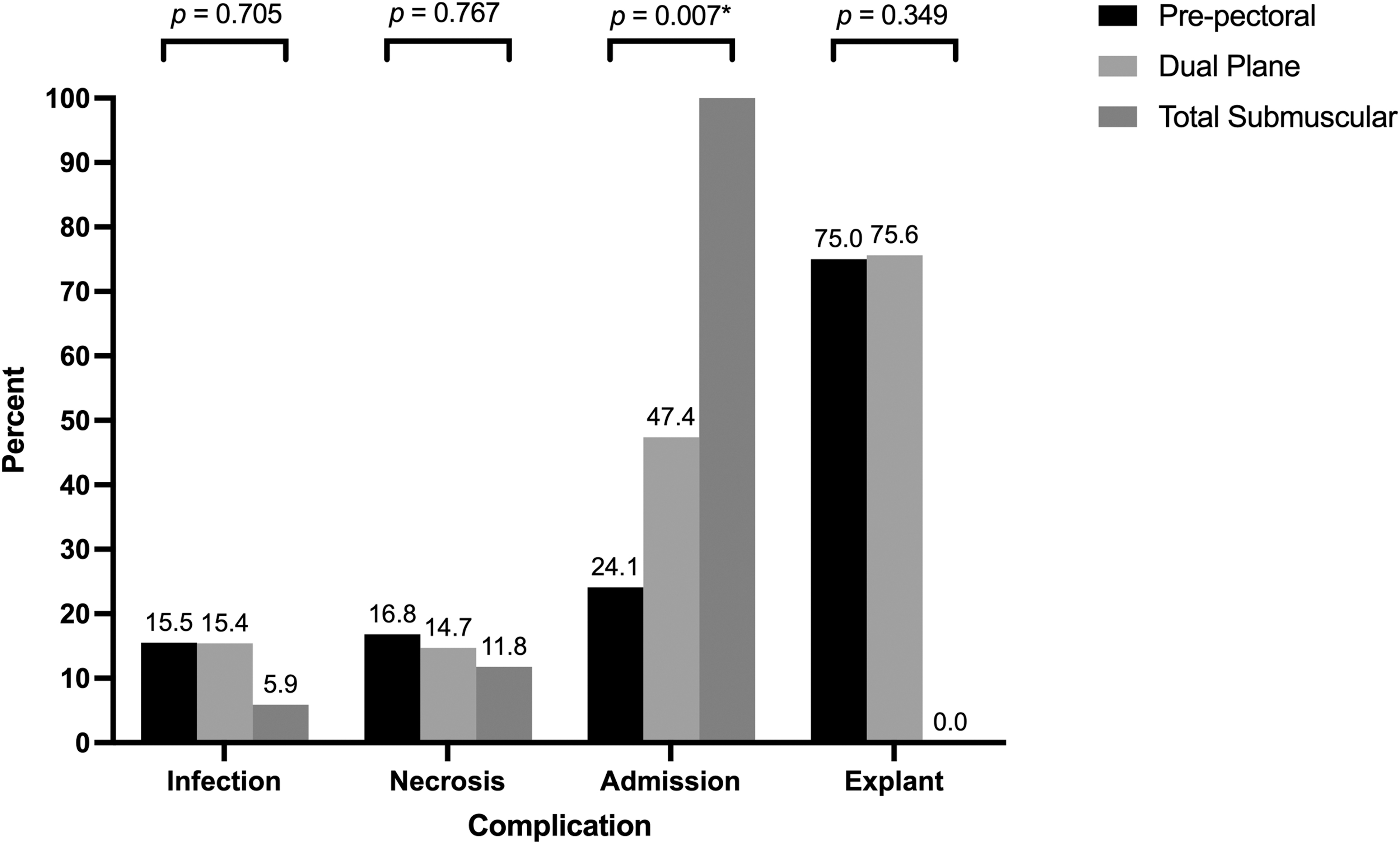
Complications between reconstructive planes.
Culture Results
Culture results not mutually exclusive.
MSSA = methicillin-sensitive Staphylococcus aureus.
Risk factors for infection
Table 3 shows all the patient attributes used for univariable analysis. Infections occurred more frequently in patients with concurrent mastectomy skin flap necrosis (26.1% vs. 12.3%; p = 0.008), patients who received post-operative radiation therapy (29.4% vs. 15.9%; p = 0.021), patients who received adjuvant chemotherapy (41.2% vs. 25.5%; p = 0.015), and patients who are active smokers (8.7% vs. 2.1%; p = 0.019). There was a trend toward significance noted for patients who received neoadjuvant chemotherapy (p = 0.063). On multivariable regression analysis, concurrent mastectomy skin flap necrosis (odd ratio [OR], 2.936; p = 0.002), post-operative radiation therapy (OR, 2.458; p = 0.007), and active smoking (OR, 6.326; p = 0.006) remained as risk factors for post-operative infection after immediate tissue expander reconstruction (Table 4).
Comparison of Patients with and without Infection
Statistically significant.
Multivariate Regression Analysis of Risk Factors for Infection
OR = odds ratio; CI = confidence interval.
Statistically significant.
Discussion
In our previous study of patients undergoing placement of permanent implants during second-stage breast reconstruction, we demonstrated that a single dose of peri-operative antibiotic prophylaxis was sufficient to achieve an adequately low infection rate; our infection rate was 3.2%, comparable to the national average. 13 At our institution, for patients undergoing immediate first-stage reconstruction with tissue expanders, we also only administer a single dose of peri-operative antibiotic agents prior to the first surgical incision as infection prophylaxis. In all patients, antibiotic agents were stopped within 24 hours from start of procedure. No patient received any antibiotic prophylaxis at discharge on post-operative day 1. In this follow-up study, our aim is to assess whether this short course of peri-operative antibiotic prophylaxis is also sufficient to achieve an adequately low infection rate in immediate tissue expander reconstructions.
Unlike second-stage implant exchange surgery, those undergoing immediate tissue expander placement during first-stage reconstruction are at a much higher risk for infection. 17 Immediately after the mastectomy, the breast pocket is vascularly compromised without adequate perfusion and circulating immune cells. This results in the higher infection rates seen with tissue expander reconstructions compared with autologous reconstructions in which tissue perfusion is preserved. 18
In our 10-year institutional cohort, the overall infection rate was 15.1%. Although the infection rate after immediate tissue expander placement is highly variable, the 15.1% rate found in this study is within the range reported in the literature (2%–35%).8–10,15,16,19 Our definition of post-operative infection included any patient started on any therapeutic oral antibiotic regimen after developing breast erythema, thus broadening the definition and likely contributing to the overall infection rate seen in our cohort. Although this definition is broad, it assures us of not underestimating the significance of breast infections. This is in contrast to other cases in the literature in which infection was more narrowly defined to within the first month post-operatively or to only include those re-admitted for therapeutic treatments.20,21
Nevertheless, even with a broader definition, our infection rate remains comparable, therefore supporting the practice of conservative antibiotic stewardship. In recent years, antibiotic resistance has increased because of widespread use, with emerging organisms resistant to nearly all available drugs. 22 For example, a 2016 study found no improvement in infection rates in immediate tissue expander reconstructions even when post-operative antibiotic agents were prescribed. 15 In the same study, when an infection occurred, there was a trend of increased resistance to the peri-operative and post-operative prophylactic antibiotic regimen over time, further emphasizing the risks with increased antibiotic use. Similarly, in a 2022 study, longer antibiotic regimens (greater than 14 days) did not protect against infection occurrence. In fact, a long course of post-operative antibiotic agents placed patients at higher risk of infection, possibly due to the emergence of resistant organisms.
Our analysis also found no association between rates of infection and reconstructive plane. To our knowledge, this is the first study comparing infection rate across reconstructive planes for tissue expander placements. Previous studies investigating infection rate across reconstructive planes have focused on second-stage permanent implant exchange procedures. Even in those studies, there was no significant difference in infection rates between placing permanent implants in the pre-pectoral plane and using a dual-plane approach.23–26 Interestingly, our analysis did find a significant difference amongst the three cohorts with regards to admission for intravenous antibiotic treatment, with the dual-plane cohort having higher admission rates. Despite this finding, explantation rates across the three cohorts were similar. Our results confirm that once the orral therapeutic antibiotic agents failed, admission for intravenous antibiotic agents was not sufficient for saving the tissue expander. In fact, it may be more prudent to remove the tissue expander as an in-office procedure when feasible rather than admission for intravenous antibiotic agents.
In our analysis, concurrent mastectomy skin flap necrosis placed patients at almost three times higher risk for developing subsequent infection (OR, 2.936). Previous studies have postulated that the necrotic skin flap increases bacterial infiltration into the breast pocket. 19 In our cohort, after excluding this group of high-risk patients, our infection rate lowered from 15.6% to 12.5%. Studies have also shown that even when an extended course of antibiotic prophylaxis was originally prescribed prior to skin necrosis occurring, the prolonged dose of antibiotic prophylaxis did not lower the infection rate after necrosis occurred. 19 Instead, surgeons should promptly excise the necrotic area to prevent infection from developing. Additionally, in our cohort, there was no difference in necrosis rates across the three reconstructive planes.
Our results concur with previous studies, including our own, that showed that a pre-pectoral approach is just as safe as dual-plane and total submuscular approaches.26,27 At our institution, regardless of the plane of reconstruction, we utilize intra-operative laser angiography in all immediate tissue expander reconstructions to assess skin flap viability. 28 When filling defects are noted, we proceed to apply nitroglycerine paste over the entire breast until discharge to improve perfusion. We currently do not prescribe an extended course of antibiotic prophylaxis against infections in case necrosis develops. Our results demonstrate that this approach yields an adequately low infection rate.
Our analysis also identified post-operative radiation therapy and active smoking as major risk factors for infection. Although the breast skin often remains intact throughout the course of radiation therapy, major trauma to the breast skin itself and the underlying breast pocket still occurs. In our practice, patients who are undergoing radiation therapy often present with radiation-induced burns and are at 2.5 times higher risk for infection (OR, 2.458). Although the exact mechanism is unclear, our results align with previous studies showing that post-operative radiation therapy is a risk factor for any post-operative complication.29–31 Similarly, tobacco use is known to cause a myriad of post-operative complications. Our previous propensity score-matched analysis of the National Surgical Quality Improvement Program (NSQIP) database identified smoking as a risk factor for all plastic surgery post-operative complications, and our results in this study concurs for the infectious complications: patients who are active smokers are at a 6.3 times higher risk for infection (OR, 6.326). 32
With the upward trend in bacterial resistance associated with prolonged antibiotic usage, our study supports the practice of conservative antibiotic regimens. In our 10-year experience, this protocol has served us well: we did not record a single case of methicillin-resistant Staphylococcus aureus infection on culture results after culturing drainage from every single case of post-operative breast erythema. In fact, the most common organisms are coagulase-negative staphylococcus and methicillin-sensitive Staphylococcus aureus, which are common skin flora. However, once mastectomy skin flap necrosis occurs, patients are at higher risk for infection. Similarly, the risk for infection increases in patients who are undergoing post-operative radiation therapy and those who are active smokers. In these patients, it may be prudent to continue with an additional course of post-discharge prophylactic antibiotic regimen to minimize infection risk, given that some attributes raise the risk of infection by more than six-fold.
In our practice currently, we begin a therapeutic course of antibiotic agents for all patients who develop breast erythema under the presumption of breast infection. This approach has also served us well, with 89.2% of breast erythema resolving after a therapeutic course and successfully saving the tissue expander. In recent years, we have shifted to a pre-pectoral approach for tissue expander placement without the use of acellular dermal matrix. This approach by default excludes red breast syndrome as a possible cause of breast erythema. In the literature, red breast syndrome is described as a retrospective diagnosis of breast erythema recalcitrant to antibiotic agents and after serial assessments have excluded infectious etiologies, likely caused by the hypersensitivity reactions to solutions used during acellular dermal matrix manufacturing process. 33 By eliminating acellular dermal matrix use, we have excluded one possible cause of breast erythema, thus further supporting our use of therapeutic course of antibiotic agents for post-operative breast erythema without worrying about overuse.
This study has several limitations. The retrospective nature of our study precluded us from fully collecting data if they were not recorded in patient charts. Also, the retrospective nature precluded us from a direct comparison to patients who received extended course of post-operative antibiotic agents. The single-surgeon, single-institutional nature of the study may limit its applicability, although our academic medical center serves a diverse patient population. Nonetheless, this study fulfills our goal of contributing to best practices and antibiotic stewardship to the literature.
Conclusions
This investigation describes our 10-year experience with a short peri-operative course of antibiotic prophylaxis for mastectomy and immediate tissue expander breast reconstruction. We are able to achieve an adequately low infection rate with a conservative prophylaxis regimen. For patients who experience breast skin necrosis, are undergoing radiation therapy, or are active smokers, an extended course may be warranted because of the much higher risk for infection.
Footnotes
Acknowledgments
The authors would like to gratefully acknowledgement the Division of Plastic and Reconstructive Surgery and the Department of Surgery at Weill Cornell Medicine and NewYork-Presbyterian Hospital for providing the staff support to compile our patient database.
Authors' Contributions
Conceptualization: Wang, Valenti, Otterburn. Methodology: Wang, Qin, Valenti, Otterburn. Investigation: all authors. Formal analysis: Qin. Data curation: Wang, Qin. Writing (original draft): all authors. Writing (review and editing): Wang, Valenti, Huang, Otterburn. Supervision: Otterburn. Project administration: Wang, Otterburn.
Funding Information
No funding was received for this article.
Author Disclosure Statement
None of the authors has a financial interest in any of the products, services, or drugs mentioned in this manuscript.