
Abstract

To the Editor:
T
A 49-year-old female underwent ascending aorta replacement, recovered well, and was discharged. However, the patient was re-admitted because of sternal wound infection with Pseudomonas aeruginosa. Vancomycin and piperacillin-tazobactam were prescribed post-operatively. However, on the twelfth day after the incision debridement, the patient's platelet count decreased rapidly from 141 × 109/L to 2 × 109/L, accompanied by obvious needle-like bleeding points throughout the body. Platelet, gamma globulin, and glucocorticoid shock therapy were performed each day. However, the therapy was not effective and the platelet count was still low. On the sixteenth day, the patient's white blood cell count gradually decreased and returned to normal; vancomycin and piperacillin-tazobactam were discontinued. Surprisingly, we found the platelet count had increased from 1 × 109/L and stabilized at 20 × 109/L within one day.
On the eighteenth day, the patient again developed a fever and vancomycin and piperacillin-tazobactam were again prescribed. Immediately, the platelet count decreased to 1 × 109/L. After discussion, on the twenty-second day, the platelet count gradually increased and returned to normal when the antibiotic was changed from vancomycin and piperacillin-tazobactam to ceftazidime and amikacin (Fig. 1).
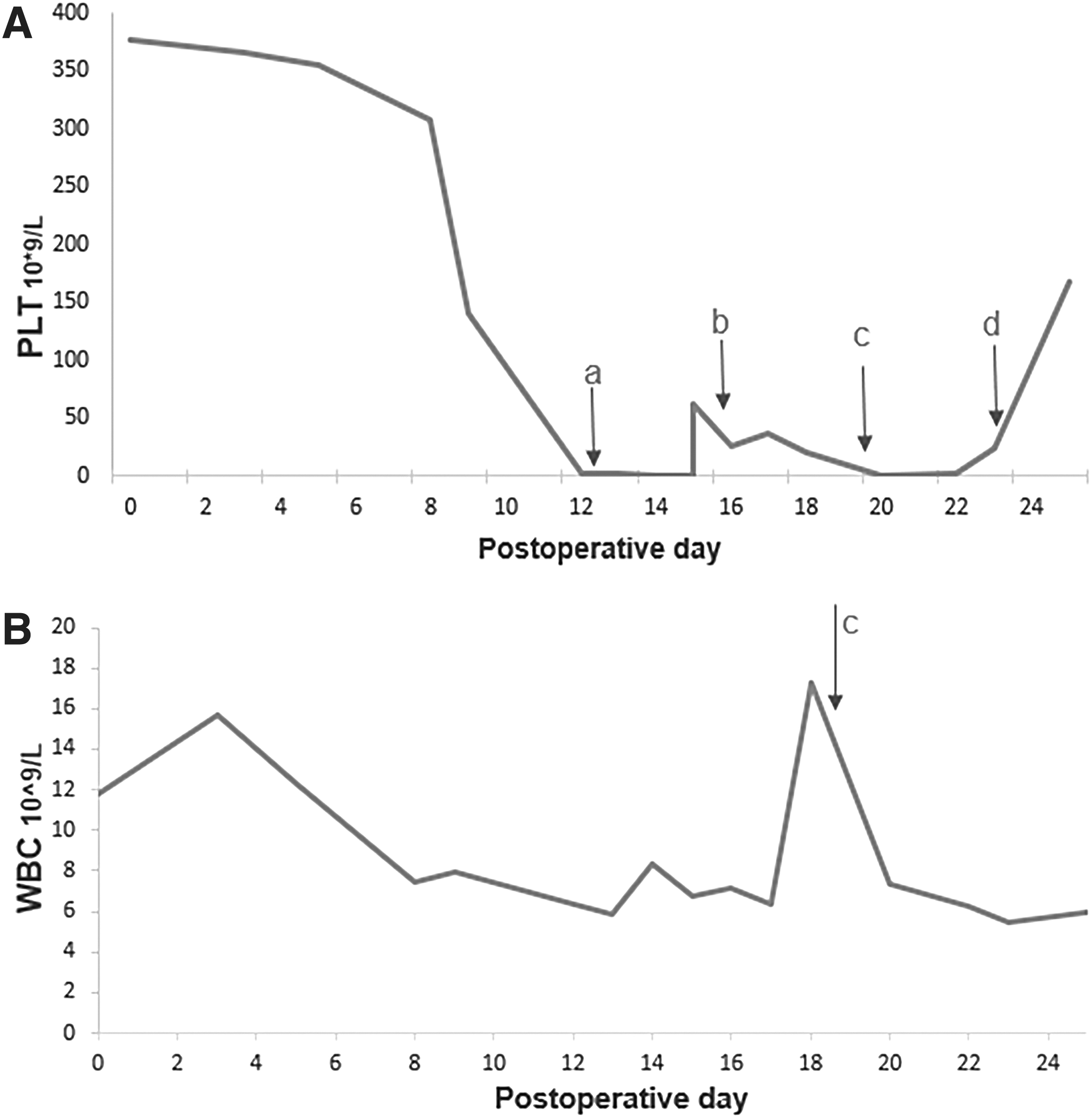
The changes to PLT (
There are several reasons to suspect the development of thrombocytopenia: acute pleural hemorrhage; artificial blood vessels or thrombosis; Pseudomonas aeruginosa infection; drugs; and chronic or acute lesions of the blood system.
First, repeated examination of chest computed tomography (CT) found that pleural effusion decreased continuously, and the encapsulated hematoma of the left chest wall faded away. Second, there was no thrombosis of artificial blood vessel or other sites through imaging examination. Third, the patient was persistently infected by Pseudomonas aeruginosa. Fourth, no abnormalities were found in the hematologic indicators and immune results. Reviewing the whole of medical history, we found that thrombocytopenia occurred twice when the patient was exposed to vancomycin and piperacillin-tazobactam twice, and after withdrawing them, platelet counts improved gradually. Finally, we determined that the antibiotic agents may be the most possible cause of thrombocytopenia in this patient. This indicated that vancomycin and piperacillin-tazobactam–induced thrombocytopenia is reversible.
We considered several reasons for the patient's thrombocytopenia. Finally, we found a clear relations between thrombocytopenia and the use of vancomycin and piperacillin-tazobactam. However, the identified mechanism of the adverse reaction remains undetermined. Usually, the sharp decrease of platelets is considered as abnormal bone marrow or immune system, but the inhibitory effect of antibiotic agents is often ignored. So, inappropriate antibiotic use should therefore be considered as part of the cause in clinical practice.