
Abstract
Background:
Post-sternotomy mediastinitis (PSM) is one of the most feared complications of cardiac surgery. The impact of a multidisciplinary management approach on this pathology is yet unknown.
Patients and Methods:
A multidisciplinary approach based on a co-management model (CMM) of care was initiated in January 2018 because of the incorporation of a hospitalist unit on a cardiac surgery department. An observational retrospective cohort study was designed to evaluate the impact of the CMM of care compared to the standard model (SM) of care in patients diagnosed with PSM. Our primary and secondary outcomes were survival time and treatment failure rate (two or more surgical procedures needed to solve PSM or PSM-related death), respectively. Data related to patient death date were collected from the Spanish National Death Index. A multivariable Cox regression model was created using those variables believed to be clinically relevant.
Results:
Ninety-one patients developed PSM from January 2010 to June 2020. Regarding the pre-operative clinical status, surgical procedure, and PSM severity, both groups had similar baseline characteristics. Patients were followed for a mean of 27.54 ± 30.5 months. A total of 60.3% of the SM group and 11.1% of the CMM group (p < 0.001) died. Treatment failure occurred in 53 patients (72.6%) in the SM group versus 7 (38.6%) in the CMM group (p = 0.007). The CMM independently reduced overall mortality (hazard ratio [HR], 0.11; 95% confidence interval [CI]. 0.01–0.83) and treatment failure rate (HR, 0.01; 95% CI, 0.001–0.183). Gram-positive bacterial infection (HR, 3.73; 95% CI, .6–8.3), and complete osteosynthesis material removal (HR, 0.47; 95% CI, 0.24–0.91) also influenced mortality in our model.
Conclusions:
A co-management care model reduced overall mortality in patients diagnosed with post-sternotomy mediastinitis.
One of the most lethal complications after major cardiac surgery is post-sternotomy mediastinitis (PSM). 1 The incidence of PSM varies from 1% to 7%,2–4 but its elevated morbidity and mortality still remain a challenge for surgeons and clinicians.
Much research has been done to understand the physiopathology and risk factors for the development of PSM,5–7 however, the evidence regarding treatment is limited. Despite the recent implementation of new treatment techniques, such as negative pressure wound therapy (NPWT), 8 mortality still varies between 12% and 41%.3,9 Increasing patient complexity, the rising prevalence of multi-drug–resistant bacteria, and the lack of a general consensus regarding its treatment might explain the lack of improvement in the outcomes of this entity.
Considering the many areas of expertise that are involved in the treatment of PSM, we hypothesized that a multidisciplinary approach might be one of the best methods to reduce mortality related to this complication. The main objective of our project was to determine if a multidisciplinary approach, anchored in hospitalist co-management, may improve PSM outcomes. Co-management is a growing model of hospital care that is based on the creation of multidisciplinary clinical teams formed by a surgeon and a hospitalist specialist. 10 Hospitalists are physicians whose primary professional focus is the general medical care of hospitalized patients. 11 In our country, co-management is still an underused care model 12 and more studies are needed to support the advantages it provides to extend its implementation.
Several studies have shown that the inclusion of a hospitalist in surgical departments, especially those that perform high-risk interventions such as vascular, 13 colorectal, 14 or neurologic surgery 15 results in better morbidity and mortality outcomes. Extending this model to a cardiac surgery department was a logical step, considering the consequences of developing severe complications such as mediastinitis. 16 We believe co-management could be extremely beneficial for these patients.
Patients and Methods
The study was conducted at Hospital Clínico San Carlos (HCSC), a tertiary care 850-bed hospital in Madrid, Spain. In January 2018 an innovative collaboration framework, the first of its kind in Spain, between the cardiac surgery department and the hospitalist service was initiated. Most post-surgical patients who were admitted from the intensive care unit to the cardiac surgery department were cared for by a multidisciplinary team consisting of cardiac surgeon and hospitalists.
To analyze the impact of this new model of care in patients who developed PSM, we designed a retrospective cohort study including all PSM patients diagnosed in our center between January 1, 2010, and June 1, 2020.
Definitions
We defined PSM applying the U.S. Centers for Disease Control and Prevention (CDC) criteria 17 that requires the presence of one of the following: organisms cultured from mediastinal tissue or fluid; evidence of mediastinitis on gross anatomic or histopathologic examination; and at least one of the following signs: fever (>38°C), chest pain, or sternal instability with either purulent drainage from the sternotomy area or suspicious findings on imaging. Patients who developed mediastinitis were identified retrospectively through medical records coding. These records were then checked against the CDC criteria.
The co-management model (CMM) was delineated between the surgeon and the co-managing physician following the Society of Hospital Medicine criteria, 11 in which the hospitalist shares the responsibility and accountability for the medical care of the admitted patient. Those patients not taken care of in the CMM were included in the standard management (SM) care group. The CMM was initiated if any of the following criteria was met: age-adjusted Charlson comorbidity index 18 higher than three; any major complication during surgery, or directly at the cardiac surgeon's request. Patients were co-managed until a consensual discharge agreement was reached by the multidisciplinary team. No patients in the SM group were evaluated by a hospitalist, although other specialists were consulted by the cardiac surgeons as needed.
Late mediastinitis was defined using the 15-day criteria established by El Oakley et al. 19 Treatment failure was established when either two or more surgical procedures were needed to achieve resolution of mediastinitis; or death directly related to PSM occurred. 9 Sternal wires or plastic clips were considered osteosynthesis material indistinctly.
Data collection
Patient's baseline characteristics and surgical procedure details were collected prospectively from the cardiac surgery unit's own medical records coding. Post-sternotomy mediastinitis diagnosis and treatment techniques were collected retrospectively from the hospital electronic health record by two of the authors. They worked independently; but cross-checked their work to detect possible errors. Data related to patient death dates were collected from the Spanish National Death index published by the Health National Ministry.
Surgical protocols
Peri- and post-surgical strategies followed the Enhanced Recovery after Cardiac Surgery document approved by the Spanish Societies of Anesthesia (SEDAR), Cardiovascular Surgery (SECCE), and Perfusionists (AEP). 20 All patients went through Staphylococcus aureus decontamination 24 hours prior to surgery with nasal mupirocin and chlorhexidine soap shower. Cefazoline (2 g) or vancomycin (1 g) plus levofloxacin (500 mg) for low- or high-risk infection, respectively, were used for antimicrobial prophylaxis. Systemic antibiotic agents were initiated during anesthesia induction and continued 48 hours post-operatively. Wound dressings and mediastinal drainages were removed 48 hours after the intervention. All patients were assessed at the outpatient clinic by a cardiac surgeon 14 and 45 days after discharge.
The treatment for PSM followed our institution's established protocol, which is based on American Association for Thoracic Surgery (AATS) guidelines 21 and the recommendations of Sjögren et al. 22 As soon as PSM was suspected, swabs for culture were taken and empirical antibiotic therapy with meropenem and linezolid was initiated because of the high methicillin-resistant Staphylococcus aureus prevalence in our area. Patients then underwent wound debridement and mediastinal irrigation with povidone-iodine solution. Negative pressure wound therapy was initiated as soon as possible in patients in whom delayed sternal closure was anticipated following the American College of Surgeons and Surgical Infection Society guidelines. 23 Primary delayed closure technique and osteosynthesis material removal (OMR) was chosen according to the surgeons criteria.
End points
This study was designed to assess the main hypothesis that patients diagnosed with PSM cared for under the CMM have better outcomes than those cared for under the SM. Our main outcome measure was survival time (regardless of cause of death). Our secondary outcome was treatment failure rate. We also analyzed if early- or late-onset PSM, presence of fluid collection in computed tomography (CT), type of gram and complete OMR during mediastinitis treatment were related to our main outcome to create our Cox-regression model.
Statistical analysis
Categorical variables were represented with their frequency distribution and continuous variables with their mean and standard deviation (SD). The association between categorical variables was evaluated with the χ 2 test or Fisher exact test and Student t-test for continuous variables.
Survival for both groups was expressed and compared with the use of a Kaplan-Meier plot and between-groups comparisons were performed using the log-rank test. The Cox regression model for survival analysis was then applied to obtain independent hazard ratios for the study
All variables believed to have clinical relevance were initially evaluated with univariable logistic regression analysis. Confounding factors were then discarded by comparing β valor with the univariable analysis with a 10% threshold. Assumption of proportional hazards was fulfilled. Final model Harrel C statistic was 0.62. Statistical significance percentage accepted by all tests was 5% (p < 0.05). Data processing and analysis were carried out using the SPSS Statistics, R version 4.0.3 (IBM Corp, Armonk, NY) and R.
Results
From January 1, 2010 through June 1, 2020, 5,450 patients underwent major cardiac surgery. Ninety-one patients developed PSM, with an incidence of 1.89%; mean follow-up was 27.54 ± 30.5 months.
Seventy-three patients were cared for under SM and 18 under CMM. No differences were found between the two care models related to age, gender, and pre-operative cardiac status (Table 1), including logistic EuroSCORE, 24 which was used as our risk cardiac operative risk evaluator. 25 Pre-operative clinical status and surgery techniques were also similar as depicted in Table 2. Regarding surgical technique for sternotomy closure, surgical steel wires were used in 65 patients (71.2%) and plastic clamps were used in 25 (27.5%) patients.
Baseline Patient Characteristics
COPD = chronic obstructive pulmonary disease functional class; LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; EuroSCORE = European System for Cardiac Operation Risk.
Pre-Surgical Condition and Procedure Description
Infection was caused by methicillin-susceptible Staphylococcus aureus (n = 11), methicillin-resistant Staphylococcus aureus (n = 8), coagulase-negative staphylococci (n = 30), methicillin-susceptible coagulase-negative Staphylococcus (n = 2), Enterococci (n = 3), Pseudomonas (n = 6), extended spectrum β-lactamase Enterobacteriaceae (10), carbapenemase-producing Enterobacteriaceae (n = 8), fungus (n = 5), and unknown in two cases. All patients were treated with surgical debridement and 87.9% required NPWT, with a similar therapy duration. Post-sternotomy mediastinitis characteristics, diagnostic techniques, and treatment strategies were also similar between the two groups as shown in Table 3.
Post-Sternotomy Mediastinitis Characteristics and Treatment
PSM = Post-sternotomy mediastinitis; CT = computed tomography; OMR = osteosynthesis material removal; NPWT = negative-pressure wound therapy.
For sternal re-fixation after PSM, 41 patients (45.1%) underwent titanium plate osteosynthesis, 18 (19.8%) pectoral majoris muscular flap and 13 (14.3%) steel wire Robicsek technique. 26 Osteosynthesis material removal was incomplete in 78,4% of the patients and similar between both groups (68.5% vs, 83.3%; p = 0.4). Length of hospital stay was shorter in those patients managed under a CMM compared with the SM model: 27.8 ± 25.3 days versus 55 ± 58.7 (p < 0.05), respectively. Sixty-five percent of the patients needed more than one surgical procedure to resolve PSM with a mean of 1.64 ± 1.01 surgeries needed to completely resolve mediastinitis.
Primary and secondary outcomes
The survival rate in the overall cohort was 49.5% (47 patients with a median survival time of 38.4 ± 11.7 months and a time until treatment failure of 106 ± 12.8 days). Cumulative surviving proportion for the first 30 days, six months, and one year after PSM diagnosis was 95% versus 100%, 63% versus 100%, and 56% versus 93% for SM and CMM groups, respectively (log-rank p value: 0.01).
Our secondary outcome, namely treatment failure, occurred in 53 patients (72.6%) in the SM group and seven (38.6%) in the CMM care group (p = 0.007). Univariable analysis showed that CMM is related to survival and treatment failure rate. Gram-positive infection and complete OMR after PSM were also associated with our main outcome, as opposed to time until PSM, fluid collection in CT, and retrosternal fluid collection (Table 4).
Treatment Failure and Overall Survival Multivariant Models
HR = hazard ratio; PSM = post-sternotomy mediastinitis; OMR = osteosynthesis material removal; CT = computed tomography.
Our Cox regression explicative model demonstrated that CMM reduces overall mortality (hazard ratio [HR], 0.11; 95% confidence interval [CI], 0.01–0.83) and treatment failure rate (HR, 0.01; 95% CI, 0.001–0.183) (Fig. 1). This finding remains true after adjusting model for patient age (HR, 0.13; 95% CI, 0.018–0.97).
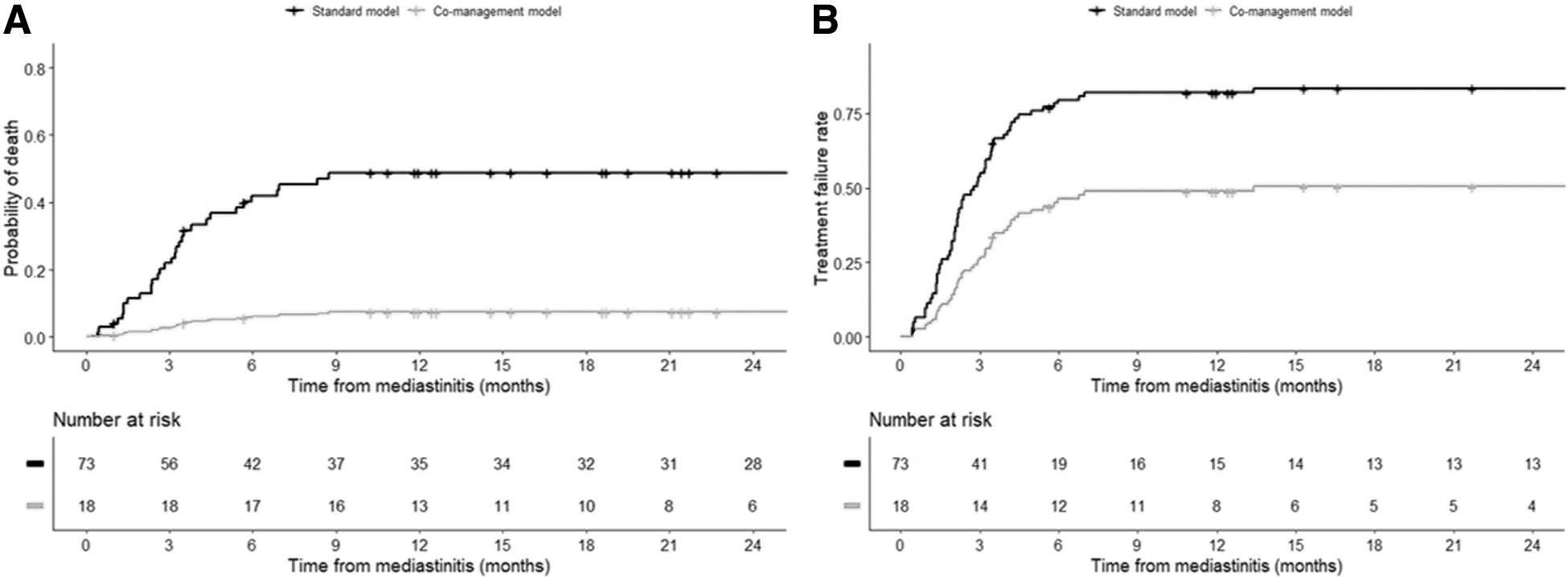
Cox-regression curves for death (
Gram-positive bacterial infection (HR, 3.73; 95% CI, 1.6–8.3) and complete OMR during PSM surgical treatment (HR, 0.47; 95% CI, 0.24–0.91) also influenced mortality in our multivariate model (Table 4). For our secondary outcome, CMM care resulted in less treatment failures (HR, 0.01; 95% CI, 0.001–0.183) as opposed to gram-positive PSM, which resulted in a higher treatment failure rate (HR, 3.73 95% CI, 1.6–8.3) (Table 4).
Discussion
Our results suggest that a hospitalist co-management care model for patients admitted after cardiac surgery leads to improvement in both short- (treatment failure) and long-term (overall survival) outcomes associated with PSM (Table 4). Regarding mortality rate, our results appear to be consistent with those available in the current literature. Although some studies report an in hospital mortality of approximately 14%, 27 when followed long term, mortality increases to 50% as reported by Risnes et al. 28 It also has been reported previously that despite adequate control of sepsis and acute wound management, mediastinitis has a long-term negative influence on survival in relation with secondary effects on cardiac, pulmonary, and renal functions. 27 In fact, congestive heart failure has been described as the first cause of death during the first 18 months after discharge in PSM patients. 27 This is why death by any cause instead of PSM-related death was preferred as our primary outcome. This also eliminated bias derived from cause of death interpretation.
Several studies have shown that multidisciplinary teams lead to better outcomes in other surgical site infections such as hip and knee prosthetic joint infection, 29 ventricular assist device-specific infection, 30 or unspecific osteosynthesis material infection. 31 There is also strong evidence that supports the benefits of hospitalist co-management for surgical patients.13,15 To our knowledge, this is the first study investigating the impact of a multidisciplinary approach on PSM.
It is reasonable to think that a sum of variables may explain our results. Although diagnosis and treatment techniques were similar in both groups (Table 3), it may appear that there is a trend toward a higher CT and NPWT utilization in the CMM group versus SM, respectively. This finding is probably explained by the addition to the care team of a hospitalist specialist with more experience in infectious disease management. It is possible that in the CMM care group, a shorter broad-spectrum antibiotic utilization, and more precise antibiotic de-escalation may also influence our results, however, those variables could not be collected retrospectively. Nonetheless, we believe that a better non-cardiac comorbidity optimization driven by the hospitalist must also play an important role in our results.
Surprisingly, we did not find association in the univariable analysis between time to PSM onset and our end point variables. The same remains true for the presence of sternal fluid collections in CT. Regarding PSM clinical appearance, contrary to what Dessap et al. 9 discovered, we did not find different outcomes between early- and late-onset PSM. Our results may be related to the high mortality of long-standing PSM patients in our sample, possibly because of the large degree of associated deep tissue damage. Computed tomography findings of post-sternotomy mediastinitis have also been controversial in the past. Our results follow the pattern of previous work, 32 showing that mediastinal collections in CT must be interpreted cautiously, especially in the early days after surgery. In our study, we did not find evidence that suggests that the presence of a pre- or retro-sternal fluid collection may influence PSM outcomes.
In the multivariable analysis, gram-type bacteria and complete OMR played an important role in PSM evolution. Worse outcomes in those gram-positive–related PSM could be explained by specific micro-organism-related properties such as higher Staphylococcus virulence because of secretion of procoagulant factors, endothelial adherence, and the bacterial surface display of agglutinins. 33 Our data are in line with other published studies that also observed worse outcomes in those PSM caused by methicillin-resistant Staphylococcus aureus. 9
Complete OMR is well standardized in other surgical site infections such as peri-prosthetic joint infection 34 but there is still little evidence available to guide this decision in PSM patients. 22 The percentage of osteosynthesis material removed during PSM surgical debridement depends on a fragile balance between risks of thoracic instability (lowered ventilatory capacity and descended cardiac output 22 ) and the benefits of assuring an sterile sternotomy before fixation. In our sample, complete OMR was associated with higher survival rate and lower treatment failure. We hope our findings facilitate decision-making for cardiac surgeons in the future.
Some limitations of this study should be considered. First, most of the data were collected retrospectively. Ethical reasons and low incidence of PSM limited the possibilities of a prospective randomized design. Anyhow, we hope that collecting data for our main variable (survival time) from a governmental national database reduced our chances of missing events. Second, this was a single-center study mainly because CMM is unusual in our country and restricted the possibilities of a multicenter design. Third, our study does not account for any potential medical and surgical practice changes over time that could have contributed to our findings. To our knowledge NPWT is one of the few advances in surgical site care that has shown an impact on PSM mortality 35 in recent years, but the utilization of this technique has been similar between groups (Table 3).
We believe these results can be replicated in similar cardiac surgery departments. Considering there is little experience with co-management in our country, 12 we hope our results can be applied in areas with a higher use of collaborative models. Further studies need to be performed to search for similar findings in other areas in which surgical site infection may also lead to disastrous consequences, as is the case with PSM.
Conclusions
Our study showed that a hospitalist co-management care model reduces mortality and treatment failure rate in patients diagnosed with post-sternotomy mediastinitis. Gram-negative infection and complete osteosynthesis material removal also influenced our outcomes. These results support the adoption of a co-management care model in cardiac surgery departments to reduce mortality associated with post-sternotomy mediastinitis.
Footnotes
Acknowledgments
We thank Pilar Ruiz, Elena Sanchez, and the cardiac hospitalization nurse team for their help during the development of this project.
This study was approved by Hospital Clínico San Carlos (Madrid, Spain) ethical committee for clinical investigation on August 18, 2020, and identified with the internal code C.I. 20/545-E.
Authors' Contributions
Conceptualization: Villamor-Jiménez, Carnero-Alcázar, Kisuule, Pérez-Camargo, Giraldo, Reguillo-Lacruz, Villagrán-Medinilla, Maroto-Castellanos, Álvarez-de-Arcaya. Writing–reviewing: Villamor-Jiménez, Kisuule, Pérez-Camargo, Giraldo, Reguillo-Lacruz. Formal analysis: Carnero-Alcázar, Hernandez. Methodology: Carnero-Alcázar, Hernandez. alidation: Carnero-Alcázar, Hernandez, Pérez-Camargo, Giraldo, Reguillo-Lacruz, Montero-Cruces, Torres-Maestro. Supervision: Carnero-Alcázar, Kisuule, Villagrán-Medinilla, Maroto-Castellanos, Álvarez-de-Arcaya. Software: Hernandez. Investigation: Pérez-Camargo, Giraldo, Reguillo-Lacruz, Calleja-Sanz, Campelos-Fernández.
Data curation: Montero-Cruces, Torres-Maestro, Villagrán-Medinilla. Visualization: Calleja-Sanz, Campelos-Fernández.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, David Fernández de Velasco. The data are not publicly available due to ethical restrictions. David Fernández-de-Velasco is the guarantor of the paper, taking responsibility for the integrity of the work as a whole, from incepton to published article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Disclosure Statement
All authors had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this article.