
Abstract

To the Editor:
S
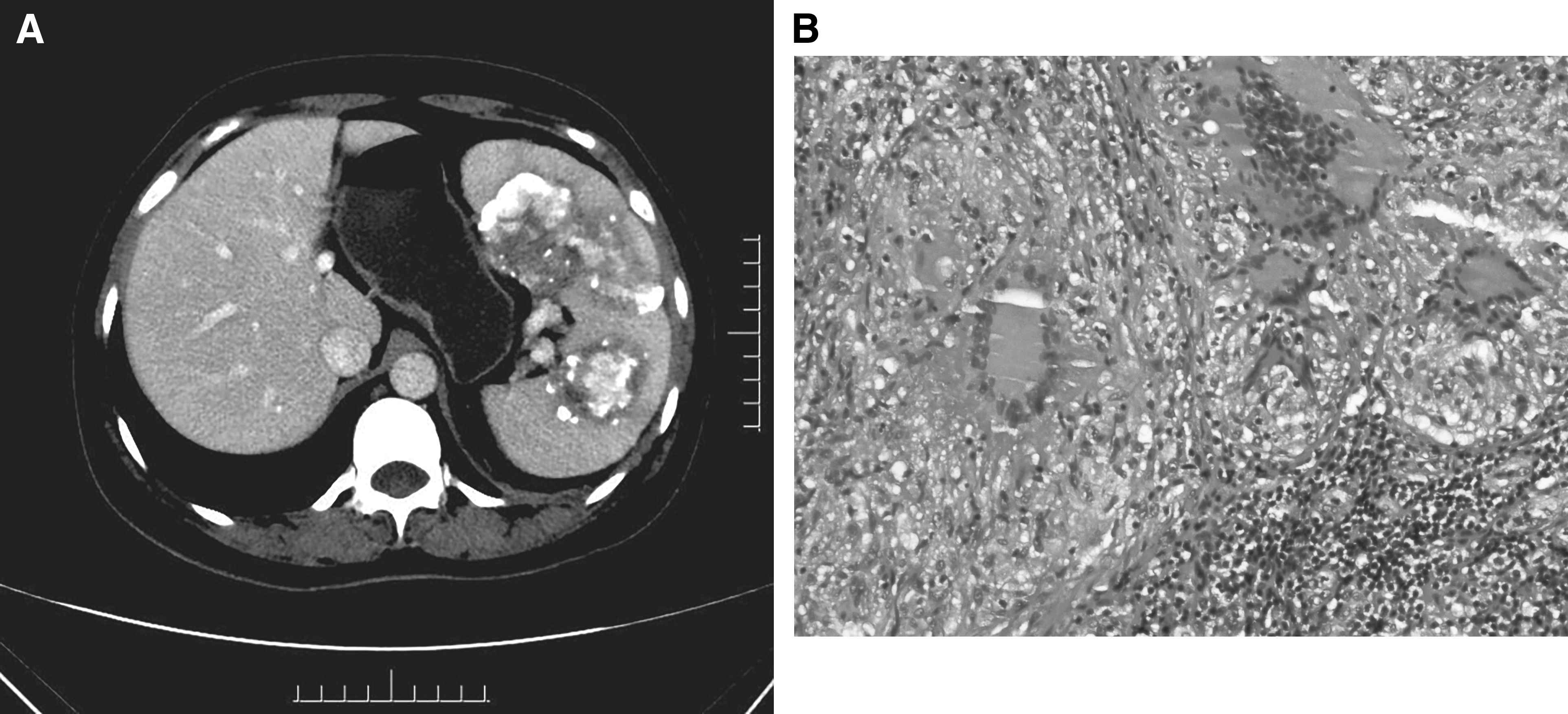
A 52-year-old female presented to the hospital because during her physical examination computed tomography (CT) had revealed a splenic mass. She had no abdominal discomfort, fevers, night sweats, and weight loss. She denied history of any infectious disease. Abdominal CT indicated multiple high-density masses with calcification in the spleen, which were considered as hemangiomas (Fig. 1A). Chest CT was normal. Human immunodeficiency virus (HIV)-1 and HIV-2 enzyme-linked immunosorbent assay was negative. Erythrocyte sedimentation rate was normal. Interferon-γ release assays was positive. The patient underwent a splenectomy and histopathologic examination of splenic mass revealed granulomatous inflammation with caseous necrosis (Fig. 1B), pathologic tissue Mycobacterium tuberculosis nucleic acid test was positive. The diagnosis of primary splenic TB was established. Anti-TB treatment continued for six months.
(
Splenic TB can remain asymptomatic initially and later present with non-specific complaints, especially in patients with primary splenic TB, splenomegaly was the common clinical manifestation that has been reported in literature [1]. Given the lack of pathognomonic findings on imaging, splenic TB is often misdiagnosed as hemangiomas, hamartomas, inflammatory splenic abscesses, or splenic cysts. The diagnosis of splenic TB usually needs histologic or cytologic diagnosis, biopsy techniques include percutaneous biopsy and surgical biopsy.
Splenic TB is rare and can be primary or secondary disease. In TB-endemic areas where the other causes of spleen mass are ruled out, splenic TB should be suspected. Pre-operative examination can be difficult to make a definitive diagnosis. Anti-TB treatment should be initiated once the diagnosis is established.