
Abstract
Background:
Peri-prosthetic joint infection (PJI) is the most serious complication after prosthetic joint replacement. However, the diagnosis of PJI remains challenging for clinicians because of the lack of a gold standard. The purpose of this study was to investigate the diagnostic significance of serum globulin, albumin/globulin, and other biomarkers in acute and chronic periprosthetic infections.
Patients and Methods:
A retrospective study of 162 patients with PJI and aseptic loosening between January 2016 and March 2021 at our institution was performed in three groups. There were 20 patients with acute infection in group A, 36 patients with chronic infection in group B, and 106 patients with aseptic loosening in group C. Globulin, albumin/globulin, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), platelet count (PLT), mean platelet volume (MPV),
Results:
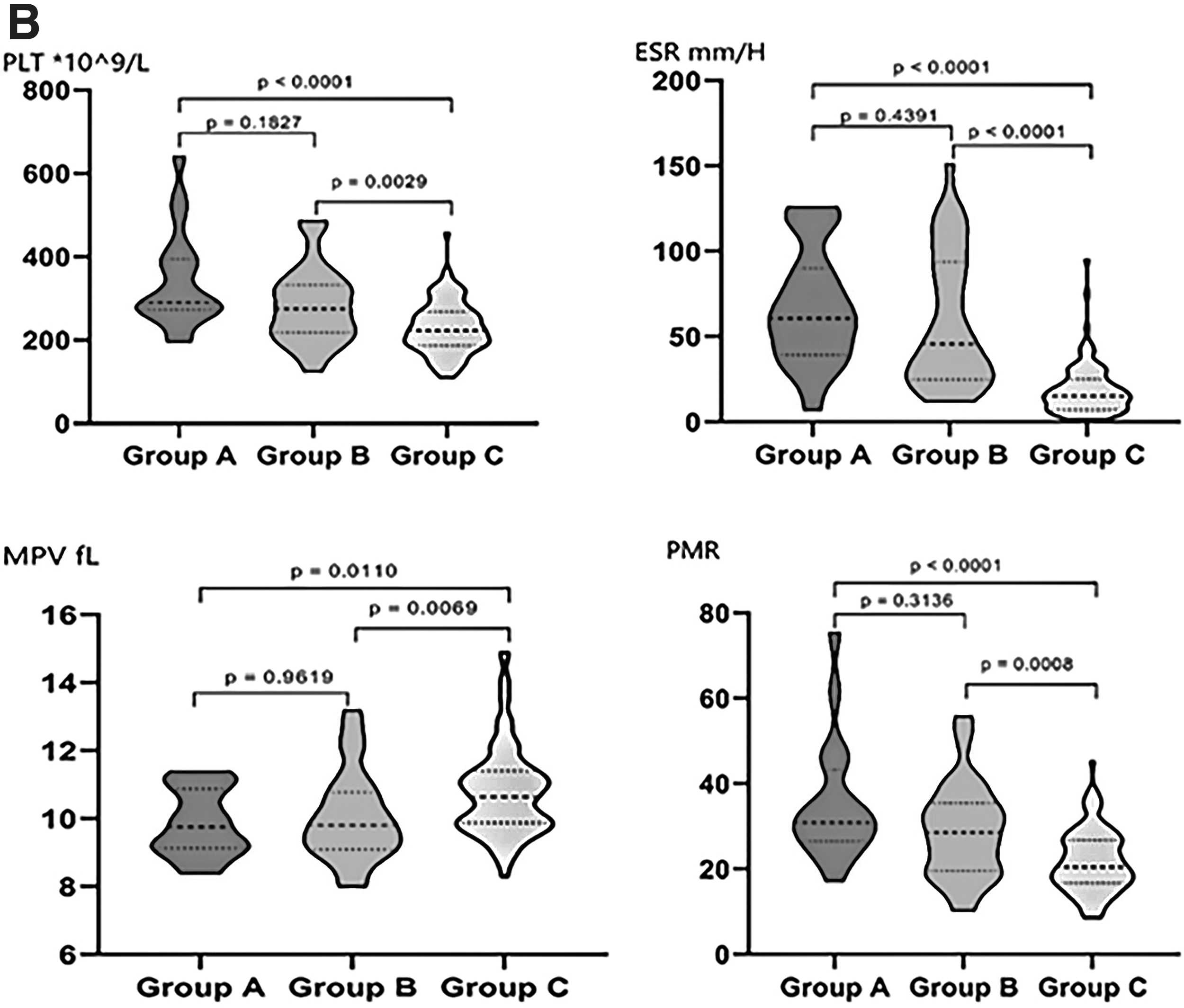
Compared with the aseptic loosening group, the acute and chronic PJI group had higher levels of CRP, ESR,
Conclusions:
Globulin and albumin/globulin have excellent diagnostic value for acute and chronic PJI and are promising potential biomarkers for the diagnosis of PJI. The diagnostic performance of albumin/globulin is superior to that of ESR and similar to that of CRP.
Peri-prosthetic joint infection (PJI) is a serious complication after primary total knee arthroplasty or total hip arthroplasty. The incidence of PJI has been reported to be between 0.5% and 2.0%. 1 Aseptic loosening is another major complication after prosthetic arthroplasty and has been reported to be one of the most common causes of failure.2,3 In contrast to aseptic loosening, the treatment of PJI has multiple options, such as debridement, antibiotic agents, and implant retention (DAIR), phase 1 antibiotic bone cement protraction, and phase 2 revision4–6 ; failure to diagnose PJI promptly may have devastating consequences for the patient.
Currently, no clinical gold standard has been established for diagnosing PJI, forcing orthopedic surgeons to rely on synovial fluid testing and serologic markers to explore and find accurate biomarkers for the diagnosis of PJI. 7 The current widely used diagnostic criteria are derived from the revised 2014 Musculoskeletal Infection Society (MSIS) criteria. 8 These criteria included at least one major criterion (sinus tract communicating with prosthesis, two positive peri-prosthetic cultures with the same pathogen collected on separate occasions) or three minor criteria (elevated erythrocyte sedimentation rate [ESR] and C-reactive protein [CRP], elevated synovial leukocyte count or change on a leukocyte esterase test strip, elevated synovial neutrophil percentage, positive histologic analysis of peri-prosthetic tissue, or a single positive culture), which played a positive role in the diagnosis and treatment of PJI. However, the diagnostic value on PJI varies widely in different studies. 9 The diagnosis of PJI is still in exploration stage.
Globulin is a serum protein present in the body that is produced in varying amounts depending on the characteristics of the invader when the body's immunoglobulin system encounters an invasion by a foreign pathogen. Several studies have shown that globulin is a key marker associated with inflammation and infection.
10
Because there are few studies on the use of globulin and albumin/globulin in the diagnosis of PJI, and there is still a lack of substantial data to validate their performance in the diagnosis of PJI. Therefore, this study was conducted to verify the relevance and accuracy of globulin and albumin/globulin in the diagnosis of PJI and to compare them with other biomarkers in the diagnosis of PJI, namely CRP, ESR, platelet count (PLT), mean platelet volume (MPV),
Patients and Methods
Study design
This study was approved by and conducted in accordance with regulations set by our Institutional Review Board. A retrospective study of 182 patients with PJI and aseptic loosening at our institution between January 2016 and March 2021 was conducted with the approval of the hospital review board. The types of surgery were total arthroplasty followed by DAIR, stage 1 antibiotic bone cement absence, and stage 2 revision or stage 1 revision. In all patients, the diagnosis of PJI was retrospectively confirmed according to the revised 2014 MSIS criteria. 8 The diagnosis of aseptic loosening is confirmed on the basis of intra-operative evaluation. We excluded patients with a lack of laboratory data (n = 3), recent anticoagulant use or history of deep vein thrombosis (n = 4), autoimmune disease (n = 2), comorbid inflammation at other sites (n = 6), hepatic or renal insufficiency (n = 4), or malignancy (n = 1).
Acute infection was defined as less than six weeks after the initial procedure and chronic infection was defined as more than six weeks. 11 The final 162 patients were included and divided into three groups: acute infection group A (n = 20), chronic infection group B (n = 36), and aseptic loosening group C (n = 106). The data of patient's gender, age, height, body mass index (BMI), and involved joints were collected separately, in which there was no statistical difference (p > 0.05) between the three groups in terms of age, gender, height, and BMI. In comparison, there was a statistical difference (p < 0.0001) between the PJI group and the loosening group in terms of involved sites. The knee joint was primarily involved in chronic infection and the hip joint was in aseptic loosening (Table 1).
Statistical Analysis of Patients' General Information
Note: Group A is the acute infection group; Group B is the chronic infection group; Group C is the aseptic loosening group.
BMI = body mass index; CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; PLT = platelet count; MPV = mean platelet volume; GLB = globulin; AGR = albumin to globulin ratio; PMR = platelet count/mean platelet volume ratio.
The three groups with statistically significant overall were compared two by two. The difference between groups with the same symbol is not statistically significant, and the difference between groups with different symbols is statistically significant.
Data extraction
The patient's basic information, surgical treatment, antibiotic treatment, laboratory test results, and culture results were recorded in detail. Patient's venous blood was obtained before breakfast on the first day of admission after an overnight fast of at least eight hours and sent to the testing department within two hours. Blood samples were tested to obtain PLT, MPV, CRP, ESR, liver function tests (including globulin, albumin/globulin) and coagulation tests (
Laboratory assessment
Platelet count and MPV were determined by our institution's SysmexXN9000 hemocytometer; ESR was measured by Zhong χ hematocrit meter; globulin and albumin/globulin were calculated by fully automated line (biochemical) instrument; CRP was measured by immunoturbidimetric method by fully automated line (biochemical) instrument; and
Statistical analysis
Normal continuous data were described by mean ± standard deviation, analysis of variance (ANOVA) analyzed differences between groups, and two comparisons were made by t-test (Bonferroni method correction); non-normal continuous data were described by median (upper quartile, lower quartile), differences between groups were tested by rank-sum test, and two comparisons were made by Dwass, Steel, Critchlow-Fligner multiple tests. Categorical data were described by absolute numbers (relative numbers), differences between groups were tested by χ 2 , and two-way comparisons were corrected by the Bonferroni method. The diagnostic value of each test was evaluated by plotting the working characteristic curves of the subjects and calculating the area under the curve (AUC) and 95% confidence interval. The optimal threshold values of the eight biomarkers for the diagnosis of PJI were determined based on the principle of the maximum Youden index. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the diagnostic tests. The AUC values were determined as excellent (0.900–1.000), good (0.800–0.899), fair (0.700–0.799), poor (0.600–0.699), and no diagnostic power (0.500–0.599).
Results
Comparison of the levels of three groups of biomarkers
The differences in the levels of different biomarkers between the infected and aseptic loosening groups were statistically significant (p < 0.01), with significantly higher levels of CRP, ESR,
Diagnostic performance of globulin, albumin/globulin, and other biomarkers in PJI
Table 2 shows the AUC, Youden index, optimal cutoff, and PJI predictive values for the eight biomarkers. The AUC in Figure 2 showed that the diagnostic performance of CRP was excellent (0.903), followed by a good diagnostic performance of albumin/globulin (0.899), ESR (0.888), globulin (0.880), and
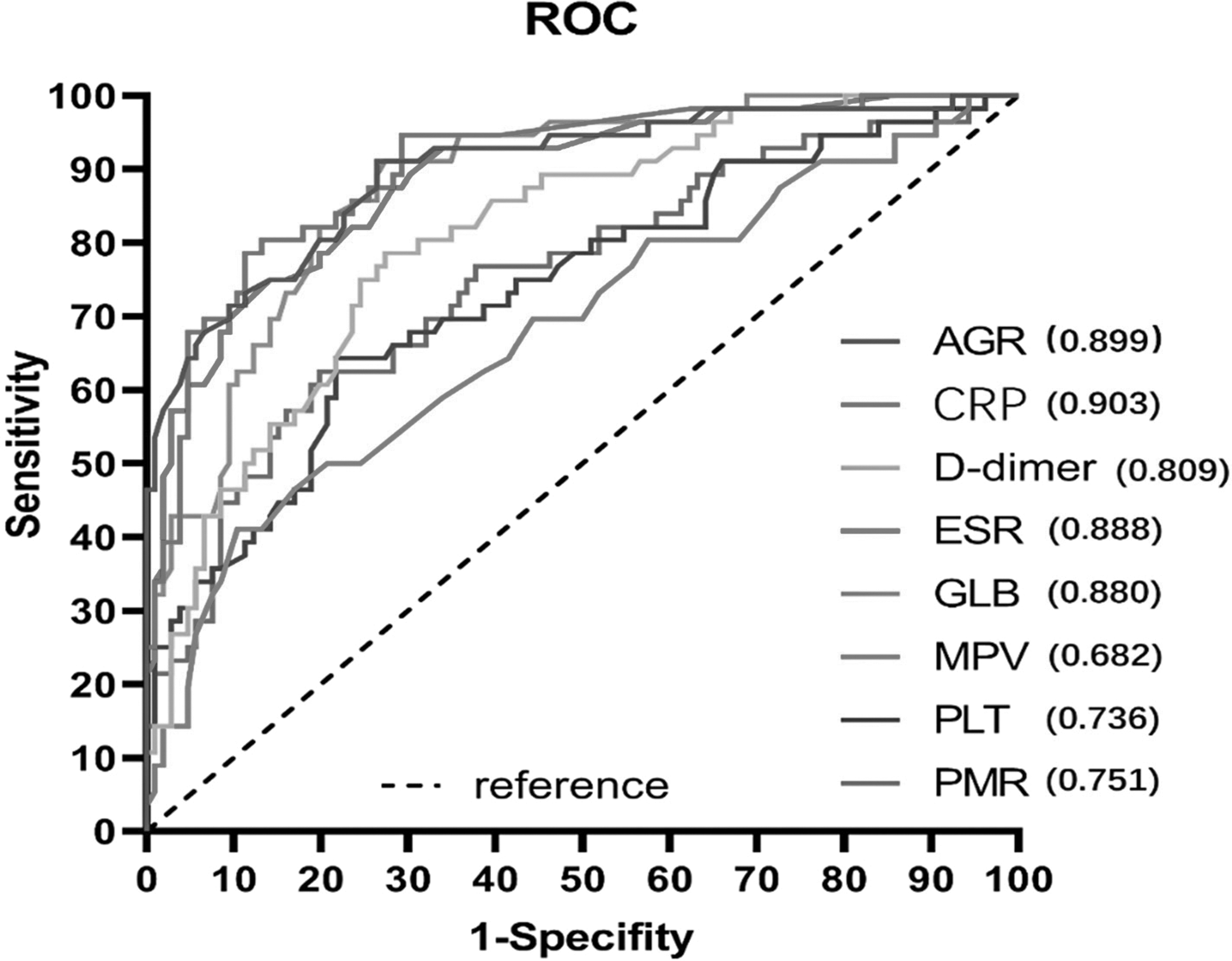
Receiver operating characteristic curves and AUC of different biomarkers. ROC = receiver operating characteristic curve; AGR = albumin to globulin ratio; CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; GLB = globulin; MPV = mean platelet volume; PLT = platelet count; PMR = platelet count/mean platelet volume ratio.
Diagnostic Performance of Different Biomarkers in PJI
PJI = peri-prosthetic joint infection; AUC = area under the curve; CI = confidence interval; PPV = positive predictive value; NPV = negative predictive value; CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; PLT = platelet count; MPV = mean platelet volume; GLB = globulin; AGR = albumin to globulin ratio; PMR = platelet count/mean platelet volume ratio.
Note: The selection of cutoff points was based on the Youden index maximum principle; 95% CI was calculated from 1000 bootstrap attempts.
Comparison of biomarker levels in the knee and hip joints in the infected group
Table 3 compares biomarker levels in patients with PJI at different sites. The results showed that the levels of
Comparison of Biomarker Levels at Different Sites in the Infected Group
CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; PLT = platelet count; MPV = mean platelet volume; GLB = globulin; AGR = albumin to globulin ratio; PMR = platelet count/mean platelet volume ratio.
Statistical results of bacterial culture
Table 4 shows the results of bacterial cultures in patients with PJI. Of the 56 patients with PJI, 31 had positive cultures, with the top three most common pathogens being Staphylococcus epidermidis in 12 (39%), Staphylococcus aureus in six (19%), and methicillin-resistant Staphylococcus aureus in three (10%).
Bacterial Culture Results of Patients with PJI
PJI = peri-prosthetic joint infection.
Table 5 shows the comparison of bacterial culture-positive and bacterial culture-negative biomarker levels in the PJI group and shows that globulin levels were higher in bacterial culture-positive patients than in bacterial culture-negative patients (35.40 > 32.6 g/L; p < 0.05).
Comparison of Biomarker Levels between Positive and Negative Bacterial Cultures in the Infected Groups
CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; PLT = platelet count; MPV = mean platelet volume; GLB = globulin; AGR = albumin to globulin ratio; PMR = platelet count/mean platelet volume ratio.
Discussion
In this study, we found that CRP, albumin/globulin, ESR, globulin, and
Serum globulin, the body's serum protein, is synthesized and secreted primarily by the liver and plasma cells in response to inflammation and infection, with antibodies and inflammatory cytokines such as complement, interleukin-6, and immunoglobulins. Therefore, elevated GLB reflects an organism's inflammatory and infectious status.12,13 Serum albumin and globulin are closely associated with various inflammatory conditions and infections. 14 Serum albumin is often used clinically as an indicator of the nutritional status of an organism, but several studies have shown that the acute phase of inflammation negatively regulates it and that there is a strong association between decreased serum albumin and post-arthroplasty sepsis15,16
This implies that lower serum AGR can be a better response to the inflammatory and infectious state of the body. Although the role of globulin and AGR in inflammation and infection has been demonstrated in several studies, further validation is needed in the diagnostic performance of PJI. Ye et al. 17 found that both GLB and AGR are associated with PJI and can be used as potential auxiliary biomarkers for diagnosing PJI. Wang et al. 18 showed that GLB and AGR can be used to diagnose patients with suspected PJI and are promising biomarkers for diagnosing PJI. Shang et al. 19 showed that GLB and AGR were found to have good diagnostic value for PJI and can predict culture results and persistent infection accurately. However, the results of both Wang et al. 18 and Shang et al. 19 indicated that the diagnostic performance of globulin an AGR was lower than that of ESR and CRP, but our results found AGR superior to ESR (0.899, 0.888) and was similar to CRP (0.899, 0.903) in the diagnostic performance of PJI.
C-reactive protein and ESR are the most frequently used clinical indicators for diagnosing PJI, but their diagnostic performance in PJI still has different definitions. McArthur et al. 9 investigated seronegative cases of PJI after hip and knee arthroplasty, and their findings suggested that the combination of ESR and CRP could improve the diagnostic accuracy. Saleh et al. 20 showed that ESR and CRP had the highest value in the diagnosis of PJI. However, it has also been found that ESR and CRP do not meet the guideline diagnostic criteria for PJI in some hypotonic and chronic PJI, such as coagulase-negative staphylococci, Bacillus, and Propionibacterium acnes. 21 This suggests that the diagnosis of PJI by CRP and ESR alone is unreliable. In the present study, CRP had the highest AUC of 0.903, and ESR had an AUC of 0.888, showing good diagnostic performance for PJI.
Platelet count plays a powerful role in mediating the innate aspects of the organism to acute and chronic inflammation and infection.27–29 The results of Gaertner et al. 30 showed that PLT can directly contribute to the organism's response to infection. When stimulated by bacteria, PLT can secrete a series of bioactive peptides stored in its alpha granules and dense body contents. 27 Korniluk et al. 31 found that MPV has been studied as a potential biomarker in cardiovascular, respiratory, and oncologic diseases. In the last two years, several studies have seen the value of PLT, MPV, and PMR in diagnosing PJI. Paziuk et al. 32 showed that PLT and MPV are associated with PJI and deserve consideration in the evaluation of patients with potential PJI. Maimaiti et al. 33 reported that PMR combined with ESR and CRP had better diagnostic performance than MPV alone in the diagnosis of PJI. However, Sahin et al. 34 found that the diagnostic performance of MPV was low and did not support its use to improve the accuracy of PJI diagnosis. Our results showed the average diagnostic value of PMR and PLT for PJI (AUC 0.751 and 0.736, respectively) and poor diagnostic value of MPV (AUC 0.682). Here our results were similar to the study by Sahin et al. 34 However, the specificity of MPV was highest (89.62%) at the optimal cutoff point, which suggests that low levels of MPV can well reduce the misdiagnosis rate of PJI. In conclusion, although PLT, PMR, and MPV have underperformed in the diagnostic performance of PJI, they can be well used as an aid to diagnose PJI.
Bacterial results showed that Staphylococcus epidermidis (39%) was the most frequent, followed by Staphylococcus aureus (19%). The positive bacterial culture rate was 55% (31/56) and the negative rate was 45% (25/56). The higher negative rate in this study compared with other similar studies may be related to the fact that the patients had already used antibiotic agents in other clinics before being hospitalized for surgical treatment. The new finding in this study that the difference in globulin levels between bacterial culture-positive and bacterial culture-negative patients with PJI was statistically significant (35.40 > 32.6 g/L; p < 0.05) suggests that globulin may be more sensitive compared to other indicators in bacterial culture-positive patients with PJI, but further data are needed to verify this.
This study has some limitations. First, it is a retrospective analysis and some patients with negative infections may have been missed or classified in the aseptic loosening group. Second, many infections occur in patients with medical comorbidities such as liver and renal insufficiency and autoimmune diseases, and the exclusion of these patients makes these additional biomarkers less feasible. In addition, this study is still a hypothetical diagnostic study and the causal relation between globulin and AGR and PJI is still not supported by a large body of data, resulting in relatively low reliability of these two new biomarkers. Finally, this study is a single-center study with a small sample size, and a large prospective multicenter study is still needed to validate the diagnostic value of globulin and AGR for PJI.
Conclusions
Globulin and AGR have excellent diagnostic value for acute and chronic PJI and are promising potential biomarkers for the diagnosis of PJI. The diagnostic performance of AGR is superior to that of ESR and similar to that of CRP.
Footnotes
Acknowledgments
We would first like to thank my supervisor, Quang Jiao, for his constant encouragement and guidance. He has accompanied me through the various stages of writing this thesis. Without his consistent and enlightening guidance, this thesis could not have reached its present form.
All experimental protocols were approved by the Second hospital of Shanxi Medical University. All methods were performed in accordance with relevant guidelines and regulations.
Authors' Contributions
Writing, data analysis, and completion of the manuscript: R. Wang, Shi. Data collection: Zhang, T. Wang, Ren. Conception of the design of the study and revision: Jiao. All authors read and approved the final manuscript.
Data Availability
All data generated or used during the study appear in the submitted article.
Funding Information
This study was supported by grants from Fund Program for the Scientific Activities of Selected Returned Overseas Professionals in Shanxi Province (grant number 20210006).
Author Disclosure Statement
The authors declare that they have no conflict of interest.