
Abstract
Background:
The increase of multi-drug–resistant organisms has revived the use of silver as an alternative antibiotic-independent antimicrobial. Although silver's multimodal mechanism of action provides low risk for bacterial resistance, high local and uncontrolled concentrations have shown toxicity. This has resulted in efforts to develop novel silver formulations that are safer and more predictable in their application. Optimization of silver as an antimicrobial is crucial given the growing resistance profile against antibiotics. This article reviews formulations of silver used as antimicrobials, focusing on the mechanisms of action, potential for toxicity, and clinical applications.
Methods:
A search of four electronic databases (PubMed, Embase, MEDLINE, and Cochrane Library) was conducted for relevant studies up to January 2022. Searches were conducted for the following types of silver: ionic, nanoparticles, colloidal, silver nitrate, silver sulfadiazine, silver oxide, silver carboxylate, and AQUACEL® (ConvaTec, Berkshire, UK). Sources were compiled based on title and abstract and screened for inclusion based on relevance and study design.
Results:
A review of the antimicrobial activity and uses of ionic silver, silver nanoparticles, colloidal silver, silver nitrate, silver sulfadiazine, silver oxide, Aquacel, and silver carboxylate was conducted. The mechanisms of action, clinical uses, and potential for toxicity were studied, and general trends between earlier and more advanced formulations noted.
Conclusions:
Early forms of silver have more limited utility because of their uncontrolled release of silver ions and potential for systemic toxicity. Multiple new formulations show promise; however, there is a need for more prospective in vivo studies to validate the clinical potential of these formulations.
Silver is a transition metal with antimicrobial uses dating as far back as the civilizations of Ancient Greece, Egypt, and Phoenicia.1,2 Today, silver is used for its antimicrobial properties in a number of medical applications. Silver acts mainly through four mechanisms: the adherence of silver particles to the cell wall and membrane-limiting transportation across these structures; penetration into the bacterial cell and subsequent damage to intracellular structures; the generation of reactive oxygen species and free radicals leading to oxidative stress; and signal transduction pathway modulation.3,4 It has also been shown to activate an inflammatory response in human cells leading to further microbial inhibition. 3 Because of this multifactorial mechanism of action, resistance to silver is exceedingly rare. 1 These characteristics have established silver as a viable antibiotic-independent adjunct to traditional treatment regimens.2,5,6
Post-operative infections, including deep peri-prosthetic joint infections (PJIs) and more superficial surgical site infections (SSIs), are a serious complication and mode of failure in surgery. 7 The current methods of combating post-operative infections include use of antibiotic prophylaxis (e.g., cefazolin, vancomycin, and gentamicin), pre-operative prophylactic skin preparations (e.g., ChloraPrep™ [BD, Haryana India] and Betadine® [Avrio Health, Stamford, CT]), and intra-operative decontamination with saline and topical antiseptics.7–9 Despite these methods, bacteria still persist and cause post-operative infections in 2% to 5% of all inpatient surgeries, largely because of growing antibiotic resistance profiles to current treatments. 10 As a result, a growing body of research has focused on the study of complementary treatments like silver, which have a lower potential for antimicrobial resistance.2,5,6
Cytotoxicity is a primary concern in the application of silver to human tissues. The same mechanisms that mediate bactericidal activity may instead cause diffuse multisystem toxicity resulting from high local concentrations. 11 The common blue–gray skin discoloration known as argyria is the most well-documented physical finding of high silver concentrations, however, cardiotoxicity, hepatotoxicity, gastrointestinal toxicity, and weight loss have all been described in human or animal studies.11–14 It has been demonstrated that high levels of silver ion release most often drives human toxicity. 11 As a result, new formulations have been created to control the pharmacokinetic and pharmacodynamic properties of silver and to prevent the toxicity caused by the uncontrolled release of silver ions.11,15–17
The primary forms of silver being used as antimicrobials include early chemistries such as ionic silver, colloidal silver, silver nanoparticles, and silver nitrate, along with more advanced forms such as silver sulfadiazine, silver oxide, AQUACEL® (ConvaTec, Berkshire, UK), and silver carboxylate. With numerous products available, and the varied mechanisms of action, it is important to track the progression of silver and the novel techniques used to maximize bactericidal activity while minimizing toxicity. To date, minimal literature exists delineating and directly comparing the different forms of silver. This review aims to provide a breakdown of the current forms of silver used as antimicrobial agents (Table 1), creating a framework of how these mechanisms attempt to mitigate the well documented toxicity of silver, while still maintaining its broad-spectrum antisepsis.
Summary of Most Popular Medically Used Silver Formulations
Methods
Literature search
A systematic search of PubMed, MEDLINE, Embase, and Cochrane Library was performed from the inception of these electronic databases to January 2022. Searches were conducted using two phrase formats: [type of silver] orthopedic surgery and [type of silver] wound care, for the following types of silver: silver nanoparticles, colloidal silver, ionic silver, silver nitrate, silver sulfadiazine, silver oxide, silver carboxylate, and Aquacel. Four hundred ten articles were compiled and screened by authors based on title and abstract for inclusion.
Study selection
All study designs were deemed eligible, including randomized control trials, observational studies, reviews, meta-analyses, case series, and case reports. When discussing content from review articles, citations were followed to their original studies and these studies were referenced when possible. Eligible studies for each silver formulation were considered if they reported on the mechanism of action, clinical uses in medicine or surgery, current limitations, or avenues for improvement. For each eligible abstract, the full-length article was read and judged based on merit and study design. Studies pertaining to dental care were excluded. Four reviewers worked independently to determine if a study met inclusion criteria, with the senior author (D.R.G.) providing a final unbiased review when a consensus was not reached. A total of 82 studies were included in this review through this screening process (Figure 1). Most of the studies were of randomized control trials, or observational studies used to review efficacy and uses of each silver formulation in medicine. There was also a significant number of studies that were from basic science that evaluated the mechanism of each silver formulation and potential side effects. Articles were gathered, sorted based on topic, and then used for draft creation. Results are reported by type of silver.
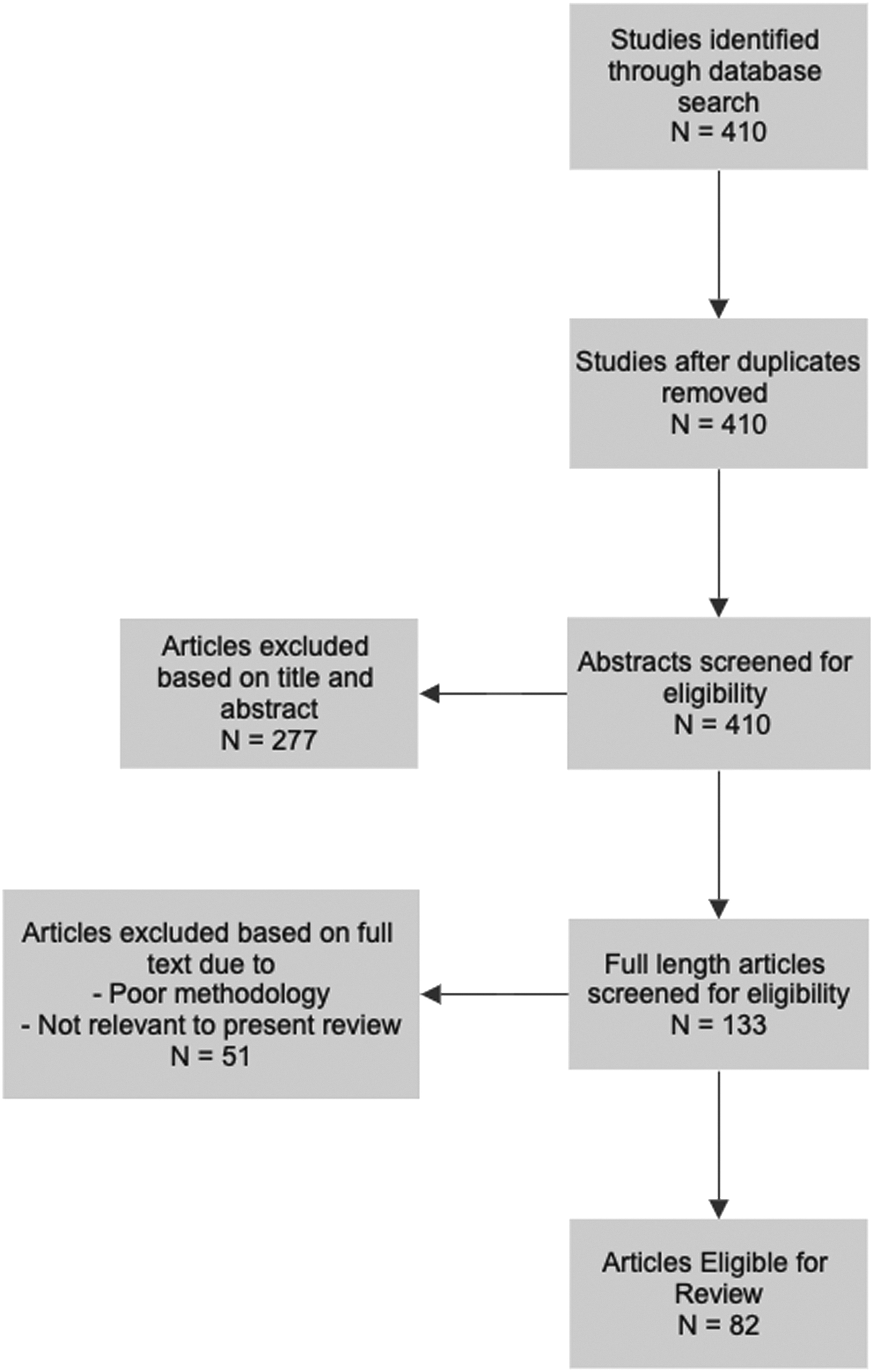
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram for study inclusion.
Results
Ionic silver
Ionic silver (Ag+) as an antimicrobial agent can be supplied from various silver salts with different solubility characteristics. 18 Highly soluble formulations deliver large, uncontrolled amounts of silver ions making sparingly soluble formulations more desirable for clinical use. 19 Ionic silver was first used as an antimicrobial in topical wound dressings. 20 However, the release of silver ions from dressings and ointments has been found to be cytotoxic to tissue and can impair wound healing.21,22 To reduce issues of toxicity, silver ions have been bound to macromolecular polyanions, which have a low solubility, limiting the concentration of free silver ions in solution. 18 More recently, the activity of ionic silver has been characterized against antibiotic-resistant bacterial strains. 23 Percival et al. 23 examined the antimicrobial efficacy of silver alginate and silver carboxymethylcellulose dressings on 49 antibiotic-resistant bacteria routinely isolated from burn wounds. All 49 bacteria, including all methicillin-resistant Staphylococcus aureus (MRSA) strains, showed susceptibility to the antimicrobial activity of both dressings. Clinically, ionic silver formulations are also used as a coating for medical devices. The delivery of ionic silver via the coating of heart valves, cardiac catheters, and urinary catheters has proved to reduce the infection rate of medical devices.24–26
In vivo use of ionic silver is complicated by binding proteins such as serum albumin, which cause free silver ions to precipitate and drop below effective antibacterial concentrations. 27 Conversely, when ionic silver concentrations in blood reach 300 ppb, toxic side effects occur including argyrosis, leucopenia, and liver and kidney damage. 24 At concentrations ≥0.5 mg/mL, ionic silver may induce DNA damage, and apoptosis in human cells despite normal histologic evaluation and cell viability testing. 28 Thus, locally elevated silver levels can have cytotoxic effects on cells despite negative findings in standard laboratory and histologic assessments.
Contrasting literature exists regarding the therapeutic index of ionic silver. Albers et al. 29 investigated the cytotoxic effects of Ag+ released from various silver particles on osteoblasts and osteoclasts. The authors found that the minimum inhibitory concentrations (MIC) of Ag+ derived from AgNO3 and silver nanoparticles for bacterial inhibition were two to four times higher than the MIC required to decrease the viability and differentiation of both osteoblasts and osteoclasts. 29 Ramstedt et al. 27 compared the antibacterial activity of ionic silver on Pseudomonas aeruginosa with the silver-induced inhibition of bronchial epithelial cell viability. The MIC studies show that the concentration range in which ionic silver could be used to treat bacteria is either very narrow or in many cases surpasses cytotoxic levels. 27 Still, numerous additional studies have concluded that ionic silver mediates antibacterial effects at noncytotoxic concentrations for eukaryotic cells.30–32
Taken in concert, ionic silver has been found to potently inhibit the growth of bacterial strains without developing bacterial resistance; however, silver ion release must be carefully controlled as high systemic or local concentrations can have severe cytotoxic effects.
Silver nanoparticles
Silver nanoparticles (AgNPs) are metal-based nanoparticles that have gained considerable attention as antimicrobials and have demonstrated efficacy against a wide range of bacteria, fungi, and viruses. 33 Because of their antimicrobial effectiveness, AgNPs have been considered as a viable alternative for wound care and post-operative infections. 34
Silver nanoparticles primarily act via release of silver ions. Even at low concentrations, AgNPs have shown promising antimicrobial activity becaues of their large surface-to-volume ratio (usually 20 to 15,000 silver atoms with diameters smaller than 100 nm). 35 However, in the same way that AgNPs are antibacterial, these mechanisms have been shown to be cytotoxic to human tissue in concentrations above 10 mcg/g. 36
Van Hengel et al. 37 examined the effectiveness of AgNPs as a coating on the surface of porous titanium implants, and showed that the nanoparticles exhibited antimicrobial activity against MRSA. The antimicrobial assays from this in vitro study revealed considerable surface antimicrobial activity and showed no formation of biofilms on the implants coated with AgNPs. Marsich et al. 38 showed that AgNPs integrated within hydroxyapatite and titanium bone scaffolds were highly effective at neutralizing both gram-positive and gram-negative bacteria. Additional studies have suggested that silver nanoparticles exhibit a weaker antibacterial effect on gram-positive bacteria due to their larger peptidoglycan cell wall. 39 As such, strains commonly implicated for PJIs such as Staphylococcus aureus have demonstrated decreased susceptibility to AgNPs. 39 In contrast, AgNPs are highly effective at neutralizing gram-negatives such as Escherichia coli even more so than silver chloride and silver nitrate. 40 Compared with common antibiotic agents, AgNPs have demonstrated a decreased risk of bacterial resistace. 41 Ellis et al. 41 showed through a series of in vitro experiments that of three common bacterial species implicated in PJIs after orthopedic surgeries, only Pseudomonas aeruginosa was able to develop resistance to AgNPs. 42
Current clinical applications of AgNPs include bone cement, external fixation pins, and wound dressings. Alt et al. 30 reported that polymethylmethacrylate bone cement integrated with AgNPs was highly antimicrobial in vitro against Staphylococcus epidermidis, methicillin-resistant Staphylococcus epidermidis, and MRSA. Compared with gentamicin-loaded cement that was only able to inhibit Staphylococcus epidermidis, AgNP-loaded cement was effective at completely inhibiting all three strains. Furkert et al. 43 examined the effectiveness against Staphylococcus epidermidis biofilms for AgNP-coated stainless steel fixator pins. Compared with copper, titanium, and uncoated stainless-steel pins, the AgNP-coated pins demonstrated a 3-log step reduction in biofilm colony-forming units. 43 Wound dressings containing AgNPs have also been shown to have a greater antimicrobial effect compared with dressings with bulk silver, although it is unclear whether this comes at a tradeoff with increased cytotoxicity. 44
Concerns regarding AgNP size, concentration, and coating methods as factors affecting toxicity have prevented this formulation's widespread usage. Carrola et al. 45 demonstrated that cytotoxicity derived from AgNPs is associated with uncontrolled silver ion release. They also determined that the type of nanoparticle coating had the largest effect on human keratinocyte cell viability, independent of nanoparticle size. Silver nanoparticles have also demonstrated dose-dependent toxicity on osteogenesis-related cells such as osteoblasts, osteoclasts, and mesenchymal stem cells (MSCs). Pauksch et al. 36 demonstrated the cytotoxic effects of AgNPs on osteoblasts and MSCs at concentrations of 10 mcg/g, a dose considered effective for medical application in other studies.33,46 Additional concerns about AgNPs stem from its usage topically, mainly in wound dressing integration. Here, AgNPs have been shown to migrate systemically causing deposits and toxicity within the spleen, liver, and kidneys. 33
Colloidal silver
Colloidal silver is a combination of silver ions and silver particles in an aqueous suspension with sizes ranging from microparticles (1,000 nm) to nanoparticles (<100 nm). 47 Colloidal silver has been applied to a wide range of uses as an antiviral, surface disinfectant, and water disinfectant. It is also utilized as a topical agent in the form of a spray on treatment for streptococcus pharyngitis, and gingivitis. Colloidal silver has also been used to treat gastrointestinal infections and gastroenteritis. 48
The proposed mechanism of action for neutralizing bacteria is colloidal silver's ability to invade the intracellular space and alter the physical properties of the cell wall. It effectively inhibits critical transcriptional processes within bacteria due to the resulting high intracellular levels of Ag+. 49 Domínguez et al. 50 showed that a 2 × MIC was needed to neutralize gram-positive bacteria including Staphylococcus aureus and Staphylococcus epidermidis, whereas only a 1 × MIC was effective against gram-negative bacteria including Acinetobacter baumannii, Pseudomonas aeruginosa, and Escherichia coli, suggesting increased potency against gram-negatives. However, the efficacy of colloidal silver as an antimicrobial has been contested, with work demonstrating that colloidal silver may not have any antibacterial potency against common pathogenic strains such as Staphylococcus aureus, Pseudomonas aeruginosa, and Escherichia coli. 51
Although colloidal silver is less frequently used as an antimicrobial, its potential as a component for wound dressings has been investigated. 52 Tran et al. 52 demonstrated the ability of colloidal silver for bacteria and biofilm neutralization. A colloidal silver gel wound dressing resulted in a 7 log inhibition for Pseudomonas aeruginosa, Staphylococcus aureus, and Acinetobacter baumannii both in vitro and in vivo compared to the control dressing. 52 The gel also demonstrated strong antibiofilm effects, exhibiting total biofilm inhibition in the wound dressing and tissue. 52 The efficacy of colloidal silver against clinical isolates from patients experiencing chronic rhinosinusitis was also examined. 53 Feizi et al. 53 demonstrated that colloidal silver was an effective antibacterial agent against planktonic and biofilm forms of both gram-positive and gram-negative strains; without exhibiting cytotoxicity on airway epithelial cells.
Because of safety concerns, colloidal silver is not commonly utilized in healthcare. These concerns are mainly due to the uncontrolled release of silver ions. Locht et al. 54 demonstrated that there is a concerning amount of continuous release of ionic silver from the exterior of early forms of silver such as colloidal within minutes of their exposure to the human body. Uncontrolled silver ions are thought to subsequently contribute to decreased macrophage viability via apoptosis and necrosis and cause a proinflammatory response. 54
Silver nitrate
Silver nitrate is a highly soluble compound that has been historically used for cauterization and the treatment of burns.18,55 This formulation represents the first use of silver as an antimicrobial, however, its fast and uncontrolled release of silver ions have limited its modern-day antimicrobial utility.18,55
Silver nitrate's high solubility (122 g/100 mL) means that it freely dissociates into silver cations and nitrate anions. 54 It is typically prepared by combining silver nitrate with hydrochloric acid to produce either a solution, a powder, or a solid pencil-like structure. 55 Topical application of silver nitrate results in a large, rapid delivery of silver ions that exert strong antibacterial activity by breaking down cell walls and inhibiting bacterial growth.
In the eighteenth and nineteenth centuries, silver nitrate was used to treat deep or fresh burns that were associated with great pain and irritation. 55 When knowledge of micro-organisms developed in the late nineteenth century, its use expanded to treating infected tissue. In 1879, a 2% silver nitrate eye drop solution reduced the rate of conjunctivitis in newborn children from 13.6% to 0.5% in Germany. 55
Silver nitrate has very potent antimicrobial activity without developing bacterial resistance.56,57 Ellis et al. 41 ran a series of in vitro experiments with Pseudomonas aeruginosa, Acinetobacter baumannii, and Staphylococcus aureus. All three of these species developed resistance to ciprofloxacin while none of them developed resistance to silver nitrate. 41
Although effective at preventing bacterial infections, dressings containing 0.5% silver nitrate have been shown to increase the risk of inappropriate wound healing 58 ; 0.5% silver nitrate has also been found to cause the skin surface to blacken, especially when exposed to light. 59 Drewa et al. 58 studied the effect of silver nitrate on murine 3T3 fibroblasts viability in vitro during a duration of three to 12 hours. The lethal concentrations of silver nitrate for 50% viability (LC50) were 6.44 dmM after a three-hour exposure and 6.91 dmM after a 12-hour exposure, suggesting that silver nitrate had a similar toxicity for a short-term and long-term exposure. 58
Poon et al. 21 studied the in vitro cytotoxicity of silver nitrate on keratinocytes and fibroblasts. They found that a solution of >50 × 10−4% silver nitrate had a lethal effect on all human keratinocyte cultures as early as three hours after exposure. 21 For fibroblasts, 33.3 × 10−4% silver nitrate solution caused a 90% reduction in fibroblast activity at three hours. 21 Silver nitrate had an important historical role in wound care, however, its use as an antimicrobial has largely been discontinued because of these safety issues. 60 Although this compound will continue to have a role in cauterization, its fast and uncontrolled delivery of silver ions renders significant concerns for toxicity if used as a systemic antimicrobial.
Silver sulfadiazine
Silver sulfadiazine (SSD) is a topical antimicrobial that is commonly used in burn wound dressings.55,61 This formulation blends the antibacterial elements of sulfadiazine with the biocidal effects of silver, creating a novel and potent antimicrobial. The sulfadiazine modality does not appear to be involved in the antibacterial aspects of SSD, but its binding to silver allows for the slow and consistent release of silver achieving superiority over silver nitrate and other previous silver compounds. 62 With more than 50 years in clinical use and few reported side effects, SSD has applications in orthopedics, is used as a coating on indwelling medical devices, and also prophylactically in burns, ulcers, and pressure sores.22,63,64
The most common use of SSD is in the treatment of burns.61–63 Originally silver nitrate-soaked bandages were used to prevent water loss and provide antimicrobial activity, but they required frequent dressing changes and lead to electrolyte imbalances. 65 The novel formulation of SSD allowed for more effective mitigation of these complications and faster patient recovery. 66 In animal studies, SSD showed a reduction from 87% to 7%–38% mortality rates in untreated versus SSD-treated burns. 67 Now SSD is widely available, relatively inexpensive, and the most commonly used burn dressing. 66
Silver sulfadiazine has been used to treat many of the complications associated with orthopedic injuries and surgeries.68,69 It is an effective treatment for blisters associated with lower extremity fractures, both decreasing complications and promoting re-epithelialization. 68 Strauss et al. 68 found that of 47 patients who developed a closed lower extremity fracture with blister formation, 82.3% healed without skin or wound complication when unroofed and treated with topical SSD. Silver sulfadiazine has also been recommended for use as a topical antibiotic to achieve a clean wound after an open reduction internal fixation of a calcaneal fracture. 70 Its broad antibacterial activity along with limited damage to host tissues makes it an effective antimicrobial to stimulate re-epithelization and encourage tissue regrowth. 70
Silver sulfadiazine has also been considered as a method of limiting pin site infections.64,71 Although Yuenyongviwat et al. 64 found there was no difference between the use of SSD-soaked dressings and dry dressings on pin site infection rates. Ogbemudia et al. 71 found that when 1% SSD was combined with 5% chlorhexidine there was a substantially lowered rate of pin site infections (p = 0.03). Silver sulfadiazine has also been used to treat a variety of ulcers. However, multiple meta-analyses have found insufficient evidence to refute or support its use for this presentation.72–74
There have been mixed results about the role of SSD in silver-coated catheters, Schuerer et al. 60 showed there is no benefit of using silver-coated catheters whereas Veenstra et al. 75 demonstrated that a chlorhexidine-SSD combination for silver-coated catheters has shown a reduction of bacterial colonization of indwelling catheters (p < 0.001) and reduction in catheter-related blood infections (p = 0 .005).
Although SSD has a long safety record, argyria can be observed. In SSD this only occurs in rare circumstances with extensive or extended topical use. 76 Additionally, patients may be allergic to sulfa, or in rare cases silver, and some case studies have shown organ malfunction because of silver deposition.77,78 Another limitation of SSD is it does not address patient pain. When SSD was compared with soft silicone foam dressings SSD required more analgesic for dressing changes than soft silicone. 79 This combined with the reported higher number of dressing changes with SSD than soft silicone leads to increased costs for the hospital and lower patient satisfaction. 79 When used as a topical antibiotic for burns, the biggest limitation of SSD is the need for frequent dressing changes, leading to higher risks of infection, slower healing times, longer hospital stays, higher patient pain levels (leading to increased need for analgesics), and increased costs for hospitals. 79
Silver oxide
Silver oxide is a newer silver formulation that functions by adhering to the surface of cells, releasing silver ions. As ions adhere to the surface of cells, the permeability of the cell membrane progressively increases until the cell completely lyses. 80 In Kirby-Bauer assay, silver oxide produced large zones of inhibition against bacteria and pathogens such as MRSA, Mycobacterium smegmatis, Candida albicans, and Candida glabrata. 81 Clinically, silver oxide is primarily studied in wound care. Belcaro et al. 82 found that silver oxide ointment improved microcirculation and healing rate. At four weeks a higher number of nervous ulcers were completely healed when treated with a silver oxide ointment compared with other alternative treatments. 82 Silver oxide has further been used in polyurethane film dressings in both acute wound therapy and postoperative surgical site treatment.5,82 Urethral catheters and catheter adapters have also implemented silver oxide coatings to prevent catheter-associated bacteriuria. 83 In a prospective randomized study by Schaeffer et al. 83 only 27% of patients using a silver-oxide–coated catheter developed urinary tract infections compared with 55% of patients using a regular catheter.
Silver oxide has also shown potential in preventing SSIs for joint replacement. 84 In an in vivo study using rats, Akiyama et al. 84 found that when silver oxide was added to hydroxyapatite coatings in the tibia, infection rates were significantly lower than without silver oxide. Furthermore, the use of silver oxide showed favorable results for abscesses and bone resorption. 84 Kawano et al. 85 confirmed that the addition of silver oxide to acetabular sockets containing hydroxyapatite promoted bone growth and antibacterial activity. Eto et al. 86 found that coating total hip arthroplasty implants with silver oxide containing hydroxyapatite significantly improved patients' activities of daily living without any adverse complications.
Although silver oxide has a lower ionizing capacity than colloidal silver preparations and silver sulfadiazine, an excess of silver ions can still lead to cytotoxicity. 5 Most commonly, silver topical products and sprays can lead to argyria and argyrosis. 5 In orthopedic surgery, concentrated silver oxide has been found to demonstrate toxicity to osteoblasts and suppress ossification. 86 Overall, silver oxide has shown potential as a coating for orthopedic implants, in treating nervous ulcers, and in urinary tract infection prevention in catheters. However, there are still concerns about cytotoxicity and suppression of ossification that may limit widespread use.
AQUACEL Silver Dressing
The AQUACEL Ag Surgical Cover Dressing is one of the primary silver-impregnated occlusive dressings used in orthopedics. AQUACEL is a silver-impregnated, occlusive, hydrofiber-based dressing that maintains a moist and antimicrobial environment to support wound healing. This dressing is made of a weaved cellulose center that allows it to micro-contour to the wound bed and prevent microbial growth through the release of antimicrobial ionic silver. 87 In vitro testing has demonstrated that AQUACEL dressing, compared to other silver dressing products, minimizes the voids and spaces where bacteria can thrive because of its ability to microcontour to the wound bed, allowing the ionic silver to be in better contact with the wound. 88
The antimicrobial activity of AQUACEL has been well described. Cai et al. 89 found the use of AQUACEL Ag Surgical Dressing to be an independent factor for the reduction in incidence of acute PJIs compared with a standard gauze dressing (p = 0.005). Kuo et al. 90 found that this unique surgical dressing only reduced the incidence of superficial incisional SSIs (p < 0.01), but there was no difference in terms of deep incisional SSIs and organ/space SSIs.
Dressings such as AQUACEL that incorporate hydrofiber and polyurethane foam have been shown to require fewer dressing changes than traditional dressings, using gauze or synthetic bandages. 91 On the other hand, downsides exist with this antimicrobial therapy. Michelin et al. 91 found the AQUACEL® Ag surgical dressing to allow for more water penetration, more failure, more discomfort, and was found to be more expensive than Tegaderm™ (3M, St. Paul, MN).
In addition, studies have found alternatives with superior side effect profiles to the silver-impregnated occlusive dressing. In the context of total hip arthroplasty (THA), Herndon et al. 92 found a cyanoacrylate adhesive with a polyester mesh (Dermabond Prineo, Ethicon, Somerville, NJ) to result in fewer wound infections and better wound healing compared with a silver-impregnated occlusive dressing, because of the increased tension-sharing properties of the mesh dressings and longer duration of protection from occlusion. Although an occlusive dressing such as an AQUACEL Ag Surgical Cover Dressing would be able to provide this high tension, this comes at the cost of wound healing and increases the risk of wound dehiscence, post-operative infection, and ischemic necrosis. 93
Silver carboxylate
Silver carboxylate (AgCar) is a metal-organic derived compound that is categorized under a relatively new class of antimicrobial delivery systems referred to as metal-organic frameworks (MOFs). Silver carboxylate has emerged as an attractive antimicrobial compound, because the chemistry allows for the controlled and predictable release of silver ions, increasing duration of action while decreasing risks for toxicity.15,94,95
Recent work has explored the use of a carboxylate silver, in a titanium dioxide/polydimethylsiloxane matrix (TiO2/PDMS) as a coating for commonly used orthopedic implant materials and prosthetic liners. 95 This AgCar eluting TiO2/PDMS matrix has shown antimicrobial efficacy against both gram-positive and -negative organisms. 96 Antimicrobial activity has shown significant inhibition of Staphylococcus aureus, Staphylococcus epidermidis, multi-drug–resistant Serratia marcescens, Acinetobacter baumannii, and Cutibacterium acnes while coating polyether ether ketone (PEEK), titanium, silicone prosthetic liners and stainless steel.95,97–99 Silver carboxylate has also shown promise in limiting the formation of bacterial biofilms. 15 Garcia et al. 97 demonstrated a decrease in bacterial adhesion and biofilm formation of Cutibacterium acnes after coating application to PEEK. This formulation was also observed to work synergistically with chlorhexidine gluconate as a wound care product and suture coating against MRSA and Cutibacterium acnes. 98 Clinically, AgCar is utilized as a cleaner and protectant for amputee prosthetic liners through a product known as the Liner Wand, sold by BI Medical, LLC.
Silver carboxylate is able to overcome some of the problems of cytotoxicity that are associated with previous formulations of silver due to its controlled release from a TiO2/PDMS matrix. The rate of silver ion release is postulated to be due to the strength of the covalent bonds between the silver ions and the carboxylated compound. 94 This opens the possibility of additional modification of the chemistry for aggressive release against some bacteria or subdued release in situations where excess cytotoxicity is a concern.
Recent data on the cytotoxicity of silver carboxylate is promising. Minimal cytotoxicity of various silver carboxylate compounds was observed in fibroblasts and epithelial ovarian cancer cells. 94 Furthermore, silver carboxylate showed minimal effect on in vitro osteoblast proliferation at concentrations that were effective in inhibiting growth of Staphylococcus aureus. 16 Despite this data more information on cytotoxicity is still needed to fully understand the safety of silver carboxylate in cell human lines.
Discussion
We reviewed the most common medically used silver formulations, paying particular attention to current uses as an antibiotic-independent antimicrobial. For each formulation, the authors analyzed the strengths and drawbacks, with the goal of providing a framework of where silver based antimicrobial therapy is, and what the future holds. Early forms include AgNPs, colloidal silver, and ionic silver. Broadly, we found that while the antimicrobial activity of these silver formulations has been demonstrated, two primary concerns exist. There is potential for systemic dissemination and deposition of silver particles in body organs following local application. This necessitates further studies on clearance and biodegradability of these products, especially AgNPs and ionic silver. The uncontrolled release of silver ions, which causes local concentrations to enter cytotoxic ranges and mediate cell death.
These shortcomings severely limit the utility of early silver formulations. Newer formulations attempt to overcome these weaknesses while maintaining silver's strong antimicrobial activity. An early attempt was silver nitrate, which recapitulates some traits of more advanced silver formulations, however, silver nitrate still does not control silver ion release in a safe manner, with demonstrated concerns for cytotoxicity.21,58 Silver sulfadiazine introduces a successful method of silver delivery, and has been rigorously tested, validated, and made clinically available particularly in burn care. Although still a mainstay, this formulation increases the number of dressing changes required, and may slow wound healing. 79 Silver oxide has even more recently been developed and utilizes AgNPs or microparticles to deliver silver ions. AQUACEL utilize a more complex matrix of weaved cellulose, allowing this dressing to microcontour to the wound bed and release silver ions. In turn, this formulation controls release, whereas also helping to limit silver release to the affected area. Finally, silver carboxylate builds on prior work, with perhaps the most advanced matrix for a controlled and extended elution of silver. This TiO2/PDMS matrix decreases concerns for toxicity while increasing duration of action.
Although new forms of silver improve upon the early formulas of the past, concerns still exist. Most notably, although results have demonstrated strong in vitro activity for these compounds, there are fewer studies demonstrating in vivo efficacy. Given silver's interactions with serum proteins, anions, and other sequestrants, 2 in vivo tests may show vastly different efficacy or dosing curves. One final concern is the growing number of cases of antimicrobial resistance demonstrated against silver.1,41 Although this is still exceedingly rare given silver's multimodal mechanism of antisepsis, it warrants monitoring.
Conclusions
With growing antimicrobial resistance profiles and widespread increases in nosocomial infections, the need for antibiotic-independent antimicrobials like silver are high. Multiple promising formulations of silver exist which allow for controlled dosing and limit potential for toxicity. However, there are a lack of high-quality in vivo studies to validate efficacy and dosing in different clinical scenarios. To address this shortcoming, further research must be conducted assessing these novel forms of silver. In turn, there is potential that silver may increase in popularity as an antibiotic-independent antimicrobial.
Footnotes
Authors' Contributions
N.V.: writing original draft (lead); Conceptualization (equal); supervision (lead)
CW: writing original draft (equal); formal analysis (equal); review and editing (equal). S.A.: writing original draft (equal); formal analysis (lead); review and editing (equal). D.C.: writing original draft (equal); formal analysis (equal); review and editing (equal). E.J.: writing original draft (equal); investigation (equal); review and editing (equal). J.H.: writing original draft (equal); formal analysis (equal); review and editing (equal). B.S.: review and editing (equal); methodology (equal). W.C.: review and editing (equal); investigation (equal).
C.C.B.: review and editing (supporting); methodology (equal); visualization (lead). V.A.: Conceptualization (equal); review and editing (equal); project administration (equal). C.B.: review and editing (lead); formal analysis (equal); project administration (equal). D.G.: Conceptualization (lead); project administration (lead); methodology (equal); formal analysis (equal).
Funding Information
This work was supported by Diane N. Weiss and The Sipprelle Family Foundation.
Author Disclosure Statement
C.B. holds equity in BI Medical, LLC. and in BioIntraface. D.G. holds equity in BI Medical, LLC. The remaining authors have nothing to disclose.