
Abstract
Background:
Vancomycin-resistant Enterococcus faecalis and multi-drug–resistant (MDR) Acinetobacter baumannii are rising contributors to spinal fusion and fracture-associated infections (FAI), respectively. These MDR bacteria can form protective biofilms, complicating traditional antibiotic treatment. This study explores the effects of the antibiotic-independent antimicrobial silver carboxylate (AgCar)-doped coating on the adherence sand proliferation of these pathogens on orthopedic implant materials utilized in spinal fusion and orthopedic trauma fixation.
Methods:
Multi-drug–resistant Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis were inoculated on five common implant materials: cobalt chromium, titanium, titanium alloy, polyether ether ketone, and stainless steel. Dose response curves were generated to assess antimicrobial potency. Scanning electron microscopy and confocal laser scanning microscopy were utilized to characterize and quantify growth and adherence on each material.
Results:
The optimal AgCar concentration was a 95% titanium dioxide (TiO2)-5% polydimethylsiloxane (PDMS) matrix combined with 10 × silver carboxylate, which inhibited bacterial proliferation by 89.40% (p = 0.001) for MDR Acinetobacter baumannii and 84.02% (p = 0.001) for vancomycin-resistant Enterococcus faecalis compared with uncoated implants. A 95% TiO2-5% PDMS matrix combined with 10 × AgCar was equally effective at inhibiting bacterial proliferation across all implant materials for MDR Acinetobacter baumannii (p = 0.19) and vancomycin-resistant Enterococcus faecalis (p = 0.07). A 95% TiO2-5% PDMS matrix with 10 × AgCar is effective at decreasing bacterial adherence of both MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis on implant materials.
Conclusions:
Application of this antibiotic-independent coating for surgery in which these implant materials might be used may prevent adherence, biofilm formation, spinal infections, and FAI by MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis.
Fracture-associated infection (FAI) and spinal infections are serious complications of orthopedic surgery, leading to poor functional outcomes.1,2 The incidence of FAI depends on injury severity, occurring in approximately 1% of low-energy fractures 3 with FAI rates as high as 30% in open tibial fractures. 1 In spine surgery, infection rates vary from 3.2% to 10.3% depending on surgery, patient characteristics, and the number of fusion levels.5–8
Although the most common organisms implicated in FAI are Staphylococcus species,9,10 both multi-drug–resistant (MDR) Acinetobacter baumannii (Acinetobacter baumannii) and vancomycin-resistant Enterococcus faecalis may also cause FAI, most often in the setting of military trauma and polymicrobial spinal surgery infections, respectively.7,11–14 Vancomycin-resistant Enterococcus faecalis is frequently cultured in trauma-associated polymicrobial infections of the thigh, where some studies have reported over 50% prevalence. 13 Multi-drug–resistant Acinetobacter baumannii was initially unique to combat injuries in Middle East field hospitals, but has since been seen in the continental United States12,15 where it can be a driver of infection in soft tissue injuries and open fractures.5,12,16 Colonization by Enterococcus faecalis and Acinetobacter baumannii is common among frequently hospitalized patients.17,18 Infections with either bacteria are challenging as they pose broad antimicrobial resistance and persistence through revision debridement, irrigation, and amputation.1,12,19,20
The microtopography of implant materials plays a critical role in surgical site infection (SSI). 21 Texture contributes to an increase in surface area, which gives opportunistic bacteria the chance to adhere and colonize the implant surface.21–23 After adherence, both Enterococcus faecalis and Acinetobacter baumannii form biofilms, a dynamic matrix of exopolysaccharide, protein, and extracellular DNA impenetrable to antibiotic agents and immune therapy. 24 Biofilms are the primary cause of persistent FAI. 1 They also play a major role in the increased risk of post-operative spinal infections after hardware use.6,8,25 This emphasizes the need for new antibiotic-independent modalities to manage such complications.
We have previously characterized an antibiotic-independent silver carboxylate (AgCar) based coating, which utilizes a titanium dioxide (TiO2), polydimethylsiloxane (PDMS) matrix, to initiate a controlled release of AgCar particles over an extended period of time.10,26–29 This coating has been shown to reduce bacterial adherence of Staphylococcus aureus, Staphylococcus epidermidis, and MDR Serratia marcescens on orthopedic implant materials.10,27 Therapeutic concentrations of this AgCar coating do not inhibit osteoblast proliferation, nor are they cytotoxic to eukaryotic cell lines.10,26 In this study, we use five implant materials common to spinal fusion surgery and fracture fixation to study the efficacy of this coating in preventing adherence and proliferation of MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis.
Materials and Methods
Implant biomaterials
Five orthopedic implant materials were selected for this study: titanium (Ti), titanium alloy (TiA), stainless steel (SS), cobalt chromium (CC; Stryker Trauma, Kalamazoo, MI), and polyetheretherketone (PEEK; MSC Industrial, Melville, NY). Implant materials were cut into 2.5-mm semi-circular rods via saw for PEEK, and electron discharge machining (EDM) for metallic implants. Implants were sonicated under a 10% Alconox solution in distilled deionized water for 10 minutes and rinsed again with acetone to remove surface impurities.
Preparation of silver-doped TiO2-PDMS coating
Titanium and PDMS precursors were prepared by diluting titanium isopropoxide (Sigma-Aldrich, St. Louis, MO) in isopropanol (10% v/v) and PDMS (Nusil Technology, Carpinteria, CA) in a hexane/isopropanol (70/30) mixture (10% v/v). Titanium and PDMS precursors were combined at three volume ratios, 50:50, 75:25, and 95:5 (TiO2-PDMS), based on previously established protocols. 26 Silver neodecanoate (25% in xylene, Gelest, Morrisville, PA) was then added to the mixture. A solution of only silver neodecanoate was used as a positive control and termed 100% Ag. Negative controls were left uncoated, without matrix or silver.
Samples were prepared and a 10 × dopage of AgCar was selected based on prior studies.10,27 The implants were dip-coated in the prepared coatings, allowed to dry overnight in the fume hood, and weighed pre- and post-coating to confirm loading. They were then placed in sterile pouch bags and autoclaved at 121°C for 40 minutes. A total of 20 trials for each of the eight different coating/AgCar concentration, n = 160 data points per pathogen were collected for each methodology.
Bacterial inoculation
Multi-drug–resistant Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis were obtained from ATCC (Manassas, VA). Multi-drug–resistant Acinetobacter baumannii was grown in Tryptic Soy Broth (TSB) (Sigma-Aldrich, St. Louis, MO), and vancomycin-resistant Enterococcus faecalis in brain-heart infusion (BHI) media (Sigma Aldrich) with 6 mcg/mL vancomycin. The cultures were grown overnight in an incubator at 37°C. Implant samples were inoculated with each pathogen at a concentration of 1 × 107 colony forming units per milliliter (CFU/mL) and allowed to adhere for four hours. Samples were rinsed with phosphate buffered saline (PBS) to remove non-adherent bacteria and allowed to proliferate over the next 20 hours.
Dose response curve
Ninety-six–well plates were coated with 10 mcL of the respective TiO2-PDMS matrix formulation and increasing concentrations of AgCar. Every AgCar condition was tested at three different TiO2 and PDMS ratios (50:50, 75:25, and 95:5). After culturing, 200 mcL of 107 CFU/mL of bacteria was transferred into their corresponding coated wells and incubated for 24 hours. After incubation, 150 mcL of each sample was transferred to a new sterile plate and read by spectroscopy at 562 nm. Results were correlated to CFU/mL according to pre-established correlations between OD562 and bacterial CFUs.
Scanning electron microscopy preparation
After 24-hour incubation, the implants were fixed in 2.5% glutaraldehyde with a sodium cacodylate buffer (pH 7.4), put through a gradual ethanol dehydration, dried via critical point drying (Polaron Critical Point Dryer, Quorum Technologies, Guelph, Ontario, Canada), and sputter-coated with 10 nm palladium gold using an Emitech K550 sputter coater (Quorum Technologies, United Kingdom). Images were taken by random selection to avoid operator bias. Three images were taken of each implant at 5,000 × magnification using a Hitachi 2700 SEM (Hitachi, Tokyo, Japan).
Confocal laser scanning microscopy preparation
After a 24-hour incubation, each implant was washed with 2.5 mL PBS three times and fixed in 10% neutral buffered formalin overnight. Each sample was then rinsed gently with 2.5 mL PBS three times and blocked with bovine serum albumin. After blocking, samples were tagged with an anti-LPS mouse monoclonal primary antibody (Invitrogen, Waltham, MA, USA) and anti-LTA primary antibody (Abcam BD1380, Cambridge, United Kingdom) and incubated for 1 hour at room temperature. Both antibodies were diluted to a 1:100 ratio with sterile PBS. Each implant was then washed with 2.5 mL PBS three times and conjugated with a 1:200 dilution of fluorescein isothiocyanate (FITC)-conjugated Fab goat anti-mouse IgG 2° antibody (Thermo Fisher Scientific, Waltham, MA, USA). Samples were imaged at 120 × using a Nikon eclipse-e confocal microscope and analyzed for surface coverage and biofilm density using ImageJ (NIH, Bethesda, MD).
Data analysis
Experiments were performed in triplicates and reported values are mean ± standard deviation. All data was analyzed in JMP (SAS Institute Inc., Cary, NC) using a two-way analysis of variance (ANOVA) to account for both coating and material differences across time points. A Tukey post hoc analysis was performed to further examine significance between different coatings and materials. Statistical significance was set at p < 0.05.
Results
Dose response curves
Dose response curves of AgCar were generated of the 50% 10 × (labeled 50%), 75% 10 × (labeled 75%), and 95% 10 × (labeled 95%) TiO2-PDMS coatings, against both pathogens (Fig. 1). Against MDR Acinetobacter baumannii, the 95% 10 × coating demonstrated the highest potency (median effective concentration [EC50] = 2 μM). The 50% 10 × coating showed a slower bactericidal profile against MDR Acinetobacter baumannii, requiring higher MICs of silver for bactericidal activity (EC50 = 4 mcM). All three ratios of TiO2 and PDMS demonstrated similar potencies against vancomycin-resistant Enterococcus faecalis with EC50 of approximately 128 mcM. The positive control of the 100% AgCar coating is at the end of the x-axis of Figure 1.
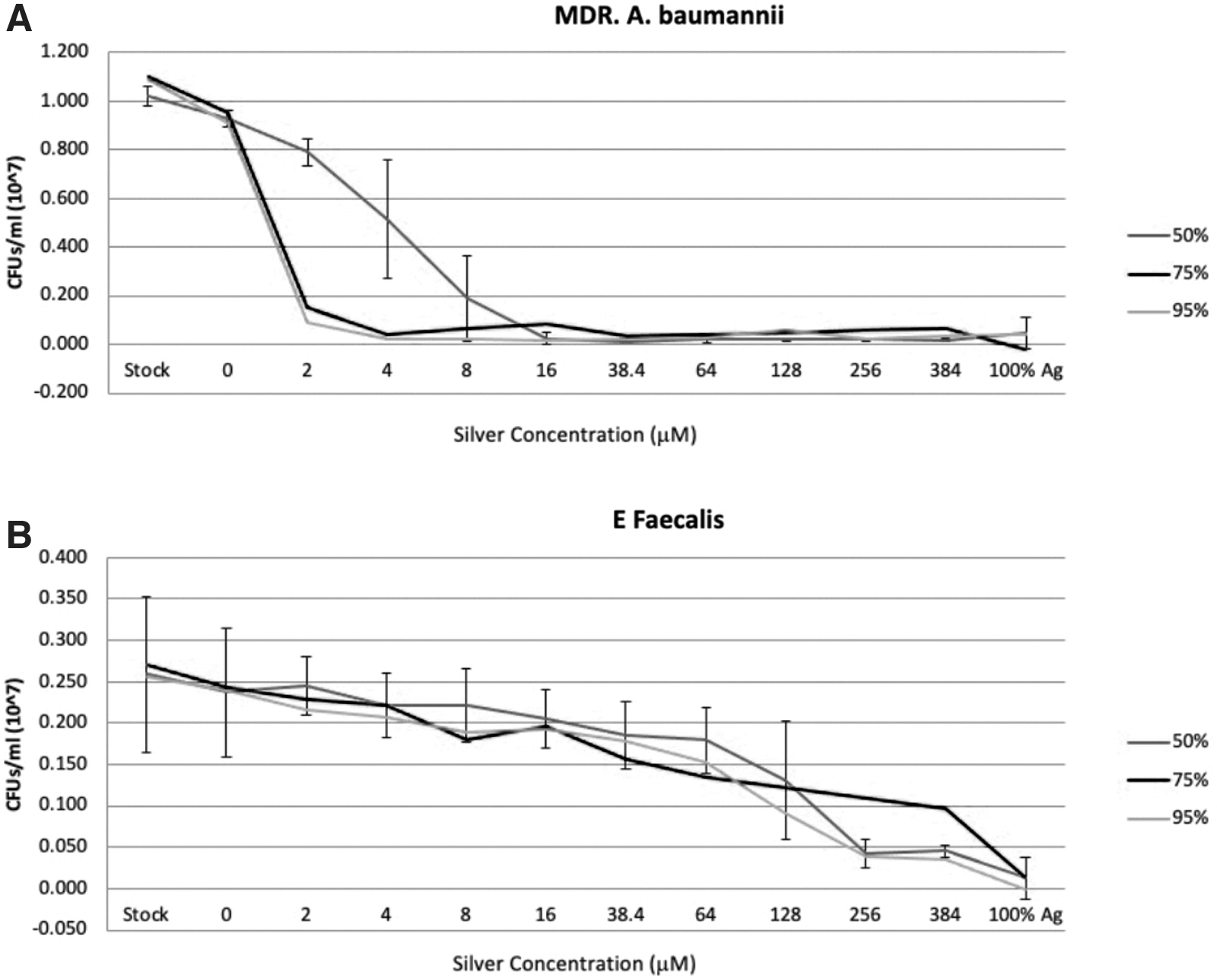
Dose response curves for silver carboxylate. (
Bacterial growth on uncoated implants
For uncoated samples, MDR Acinetobacter baumannii grew on all implant materials tested (Fig. 2). There was a difference in MDR Acinetobacter baumannii adherence across implant types by both SEM (p = 0.02) and confocal laser scanning microscopy (CLSM; p = 0.02). By SEM, adherence was lowest on Ti, and highest on CC (112.83 CFUs vs. 247.83 CFUs; p = 0.001). By CLSM, percent adherence was lowest on PEEK, and highest on TI [11% vs. 41.3%; p = 0.01). Other differences between implants were not statistically significant for either imaging technique. On visual analysis of SEM images, MDR Acinetobacter baumannii colonies were mostly localized in the ridges in the microtopography of the implants, particularly evident in CC and PEEK implants (Fig. 3).

Comparison of bacterial growth on common orthopedic materials without any coating. (
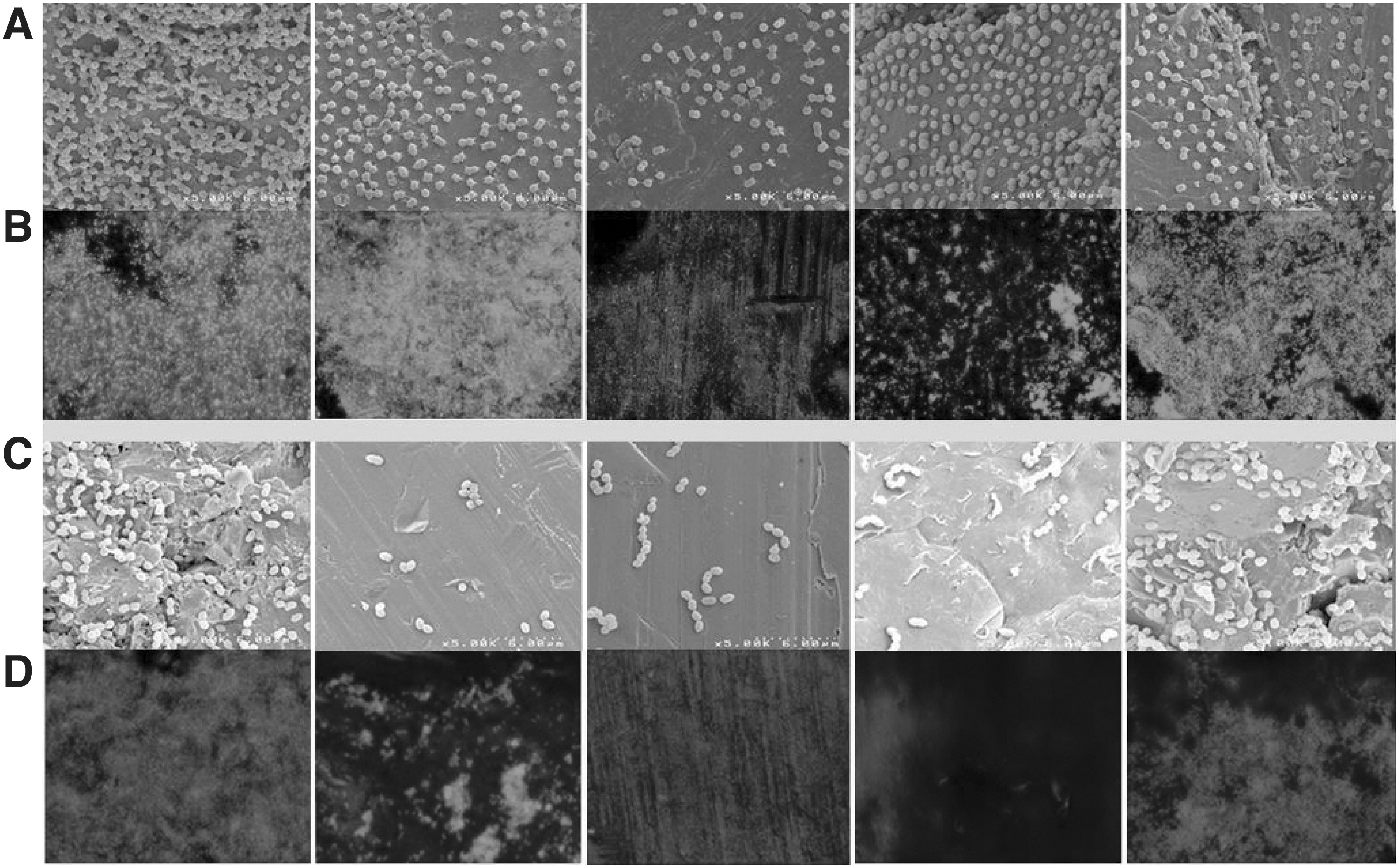
Representative images of scanning electron microscopy (SEM) and confocal laser scanning microscopy (CLSM) images on uncoated spinal implant materials. (
Enterococcus faecalis grew on all uncoated implant surfaces. By SEM, bacterial adherence was not different across implant types (p = 0.40). By CLSM, there was a difference in bacterial adherence across groups (p = 0.02). Percent adherence was lowest on PEEK, highest on CC (7% vs. 67%; p = 0.001). No other statistical differences were found between groups. On visual analysis of SEM images, vancomycin-resistant Enterococcus faecalis grew in linear clusters and more avidly on ridges, particularly in CC and PEEK (Fig. 3). No biofilm formation was seen on any of the implants tested for either MDR Acinetobacter baumannii or vancomycin-resistant Enterococcus faecalis within the time period tested (Fig. 3).
Scanning electron microscopy
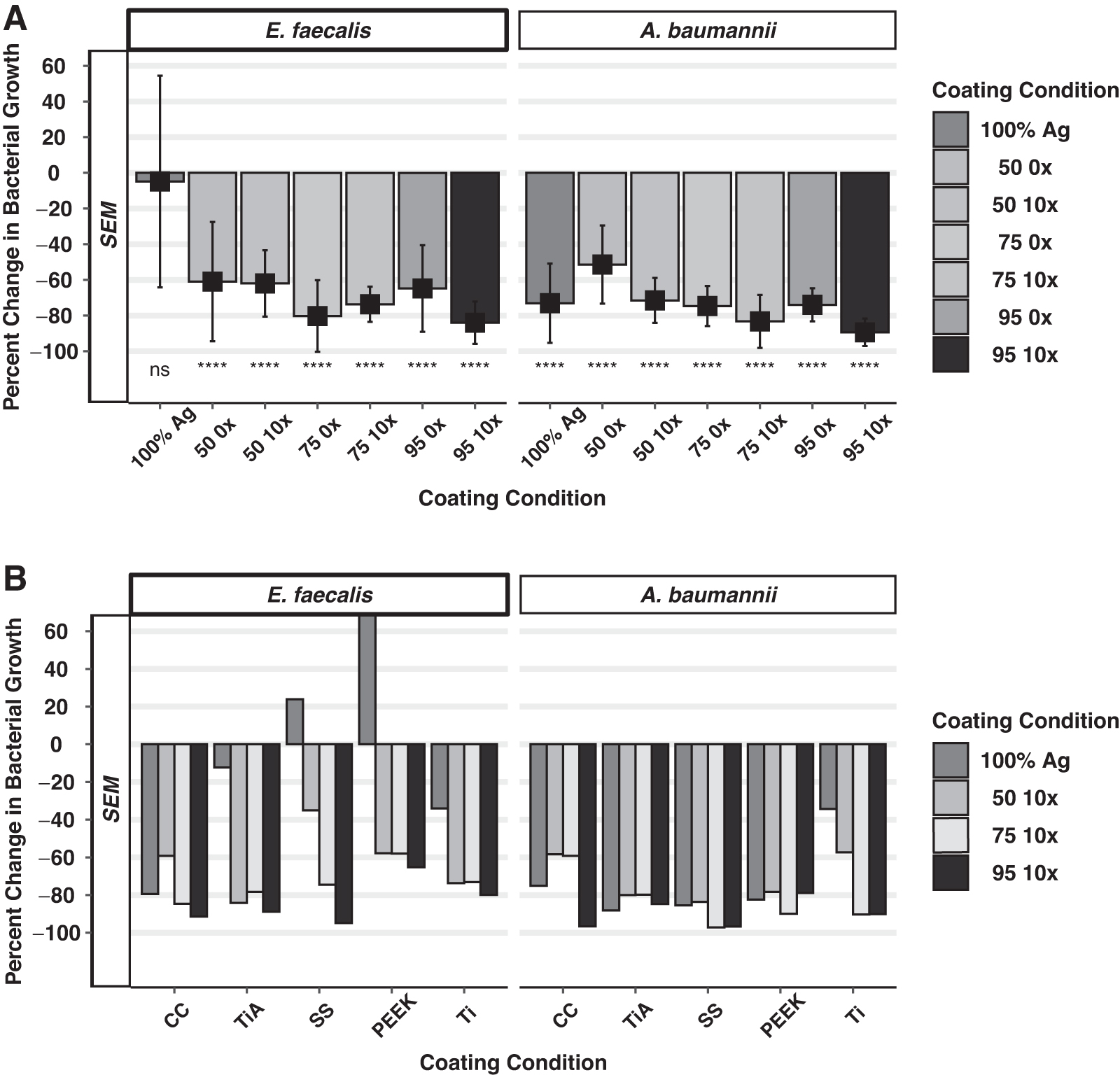
Figure 4 shows SEM data of the bactericidal effects of the 50%, 75%, and 95% matrix concentrations with and without the 10 × AgCar doping. Implant types were aggregated to study the overall effect of the coating. Compared with controls, the 95% 10 × coating inhibited vancomycin-resistant Enterococcus faecalis growth by 84% (p = 0.001), the 75% 10 × coating inhibited growth by 73.7% (p = 0.001), and the 50% 10 × coating inhibited growth by 62% (p = 0.001; Fig. 4A). Without any AgCar present, the 95% 0 × coating inhibited bacterial growth by 64.8% (p = 0.001), the 75% 0 × coating by 80.3% (p = 0.001), and 50% 0 × coating by 60.1% (p = 0.001). The 95% 10 × coating showed higher growth inhibition of vancomycin-resistant Enterococcus faecalis compared to the 50% 10 × coating (p = 0.01), but not statistically higher than the 75% 10 × coating (p = 0.63). Furthermore, the 95% 10 × coating was not significantly better at preventing bacterial adherence than the 95% 0 × (p = 0.89), 75% 0 × (p = 0.99), or 50% 0 × coatings (p = 0.8).
(
The 95% 10 × was equally effective at reducing bacterial growth across all implant types (p = 0.07), as was the 75% 10 × coating (p = 0.25). The 50% 10 × coating showed different rates of bacterial adherence across implant types (p = 0.001), with post hoc analysis revealing percent inhibition was significantly lower on SS than CC (35.1% vs. 84.2%; p = 0.003), or Ti (35.1% vs. 73.7%; p = 0.004).
Compared with controls, the 95% 10 × coating inhibited MDR Acinetobacter baumannii growth and adherence by 89.4% (p = 0.001), the 75% 10 × coating inhibited growth by 83.3% (p = 0.001), and the 50% 10 × coating inhibited growth by 71.5% (p = 0.001; Fig. 4A). Without the presence of AgCar, the 95% 0 × coating decreased bacterial adherence by 74% (p = 0.001), the 75% 0 × coating by 74.7% (p = 0.001), and the 50% 0 × coating by 51.4% (p = 0.001). The 95% 10 × coating showed statistically higher bacterial growth inhibition than the 50% 10 × coating (p = 0.004), the 95% 0 × (p = 0.04), and the 50% 0 × (p = 0.001). There was no statistical difference in bacterial inhibition between the 95% 10 × coating and the 75% 10 × coating (p = 0.61), or the 95% 10 × and 75% 0 × coating (p = 0.20).
The 95% 10 × coating showed similar bacterial inhibition of MDR Acinetobacter baumannii across implant type for the 95% 10 × coating (p = 0.19), however, there were differences by implant for both the 75% 10 × coating (p = 0.005) and 50% 10 × coating (p = 0.001). For the 75% 10 × coating, percent inhibition was significantly lower on CC compared with TiA (59.2% vs. 80%; p = 0.005), SS (59.2% vs. 97.2%; p = 0.005), and PEEK (59.2% vs. 89.9%; p = 0.0044). For the 50% 10 × coating, percent inhibition was significantly lower on CC compared with TiA (58.4% vs. 80%; p = 0.04), and SS (58.4% vs. 83.6%; p = 0.01). Furthermore, percent inhibition was lower on Ti than TiA (57.3% vs. 80%; p = 0.02), and SS (57.3% vs. 83.6%; p = 0.005).
The 100% silver condition with no TiO2/PDMS matrix showed a poor ability to inhibit vancomycin-resistant Enterococcus faecalis growth (4.84% inhibition; p = 0.496), but was able to inhibit MDR Acinetobacter baumannii growth (73.10% inhibition; p = 0.001) compared with the uncoated samples. The 100% silver had weaker inhibition of bacterial growth compared with the 95% 10 × coating against both vancomycin-resistant Enterococcus faecalis (p = 0.001) and MDR Acinetobacter baumannii (p = 0.04).
Confocal laser scanning microscopy
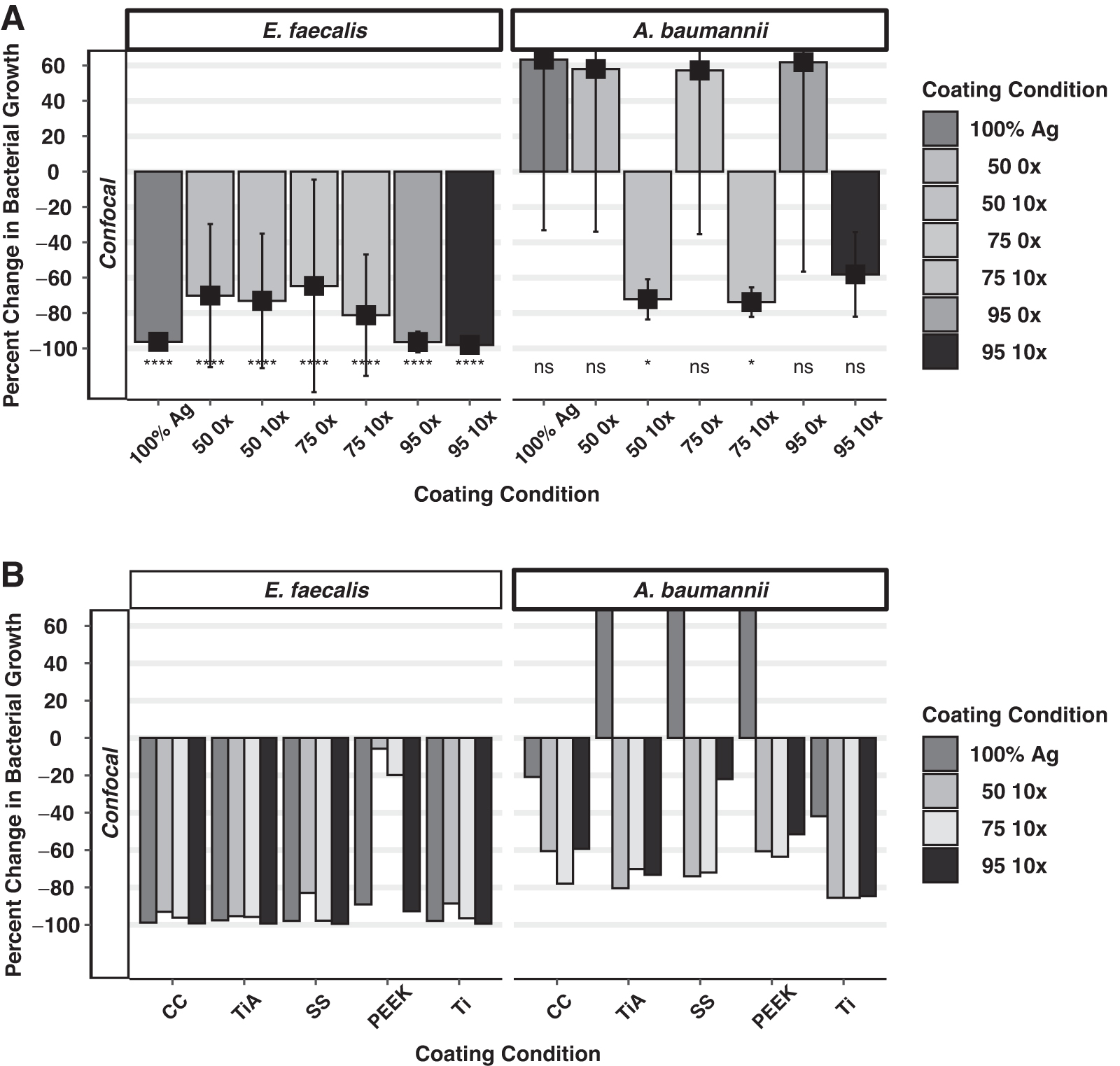
The CLSM data show similar trends to SEM data when implant types are aggregated. For vancomycin-resistant Enterococcus faecalis, the 95% 10 × coating inhibited bacterial growth 98.02% (p = 0.001) compared with the uncoated sample (Fig. 5). The 75% 10 × and 50% 10 × coatings demonstrated reductions of bacterial growth by 81.22% (p = 0.001) and 73.10% (p = 0.001), respectively. Without the presence of AgCar, the 95% 0 × condition inhibited bacterial growth by 96.38% (p = 0.001), the 75% 0 × condition by 64.7% (p = 0.001), and 50% 0 × condition by 70.1% (p = 0.001). The 95% 10 × coating showed similar decreases in bacterial adherence of vancomycin-resistant Enterococcus faecalis across all implant types (p = 0.30), as did the 75% 10 × coating (p = 0.21), and 50% 10 × condition (p = 0.40). Polyetheretherketone samples for both the 75% 10 × and 50% 10 × conditions had high standard deviations yielding varied inhibition across trials.
(
When MDR Acinetobacter baumannii confocal data were aggregated by implant type, the 95% 10 × coating decreased bacterial growth by 58.14% (p = 0.006), the 75% 10 × by 72.2% (p = 0.001), and the 50% 10 × by 73.82% (p = 0.001). Without the presence of AgCar, bacterial adherence increased compared with the uncoated sample (Fig. 5). The 95% 0 × increased bacterial adherence by 61.92% (p = 0.86), the 75% 0 × increased adherence by 57.2% (p = 0.22), and the 50% 0 × increased adherence by 58.04% (p = 0.21). For MDR Acinetobacter baumannii, the 95% 10 × coating demonstrated equal bacterial inhibition across implant types (p = 0.20), as did the 75% 10 × coating (p = 0.06), and the 50% 10 × coating (p = 0.69).
Discussion
Both MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis are of increasing concern in spinal surgical infections and FAI, particularly in the setting of combat-associated trauma.4,12–15 Their colonization of spinal instrumentation and fracture-fixation devices requires aggressive antibiotic treatment, debridement, and even hardware removal, which can be risky in spinal fusion leading to spine destabilization.8,30 There is a need for antibiotic-independent treatments for these SSIs that may work synergistically with existing therapies.
This study aims to further characterize the interactions between a TiO2-PDMS 10 × AgCar-based coating on the orthopedic material adherence patterns of MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis. Based on DRCs, a 2 mcM concentration eluted from the 95:5 TiO2-PDMS was sufficient for bacterial antisepsis of MDR Acinetobacter baumannii, whereas a 128 mcM concentration was necessary for vancomycin-resistant Enterococcus faecalis. Both of these concentrations are significantly lower than the U.S. Food and Drug Administration daily safe value of silver. 10
All coating formulations inhibited growth of vancomycin-resistant Enterococcus faecalis and MDR Acinetobacter baumannii on implant surfaces compared with uncoated samples. Increasing the ratio of TiO2-PDMS and increased AgCar concentration yielded higher growth inhibition. Compared with the uncoated samples, the 95% 10 × coating decreased the adherence of MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis on implants by an average of 89.40% (p = 0.001) and 84.02% (p = 0.0001), respectively. Bacterial inhibition was maintained over time on all materials, a trait consistently seen with AgCar.10,26,27 This is particularly important to FAI given the tendency for slow growing pathogens, not initially seen on cultures, to drive infection. 33
Interestingly, we found even without the presence of AgCar, the TiO2-PDMS matrix showed a strong ability to decrease bacterial adherence. Given the propensity of both bacteria to adhere to implant crevices, it is possible the addition of this coating served as a physical barrier to adherence and proliferation. The antimicrobial activity of TiO2 has also been well characterized,34–36 offering another explanation for the strong growth inhibition of the TiO2-PDMS matrix compared with controls.
The 95% 10 × condition conferred significantly greater inhibition than 100% Ag with no TiO2-PDMS matrix. The TiO2-PDMS hybrid coating has been shown to form a matrix that can effectively retain and provide controlled release of an antimicrobial agent.10,27 We suggest this mechanism allows for predictable pharmacokinetics and controllable release of AgCar, ensuring persistent bacteria are killed even after initial silver release on first contact. The presence of a higher ratio of TiO2 likely presents a better matrix to trap and provide a slower AgCar release.
No advanced biofilm formation was observed. This can be attributed to the short adherence and growth time of 24 hours for the bacteria, as other studies have shown a prolonged time of growth will eventually lead to fully formed biofilm colonies for both these bacteria.37–39 This indicates there is an advantage to using a AgCar-doped coating, as it may prevent the initial adherence of bacteria before full-fledged biofilms can develop.
Consistent with previous literature, 22 orthopedic material microtopography was a major factor for bacterial adherence and growth. Both pathogens preferentially adhered to crevices in the microtopography of the implants. These areas offer rougher, more irregular surfaces bacteria can anchor to for adherence. Cobalt chromium, Ti, and PEEK, which have been characterized as rougher and more fibrous, 22 generally had greater adherence rates than SS and TiA, which have smoother microtopographies. The varying growth patterns supports the concept that the industrial process of implant production, in addition to any post-production surface modifications, may play a role in the adherence and growth of bacteria.22,23,40
The 95% 10 × coating was equally effective in preventing adherence across materials tested both in this study and prior studies.10,27 Although factors such as surface chemistry and hydrophilicity of materials contribute to the adherence of bacteria, it seems the effectiveness of the coating is preserved. This would allow the 95% 10 × coating to have broad antimicrobial potential and utility, given the direct application of TiA, Ti, PEEK, and SS materials for fracture fixation.41–43 Although CC is infrequently used in appendicular skeletal fracture cases, the efficacy of AgCar would serve well in cases of spinal fusion, where cobalt chromium is increasingly popular.30,44
Conclusions
This study demonstrated a 95% TiO2-5% PDMS 10 × AgCar coating decreases bacterial adherence growth and proliferation of both MDR Acinetobacter baumannii and vancomycin-resistant Enterococcus faecalis on five different implant materials commonly utilized in spinal fusion and orthopedic trauma fixation surgery. This chemistry has the potential to be used in vivo as an antibiotic-independent coating for orthopedic implants. Prevention of adherence and proliferation by these pathogens could reduce spinal fixation infections and FAI.
Footnotes
Authors' Contributions
DG assisted in study development, data collection, analysis, writing, and editing
NV assisted in analysis, writing, and editing
AM assisted in data collection, analysis, writing, and editing
SA assisted in writing and editing
CW assisted in writing and editing
BS assisted in writing and editing
EB assisted in writing and editing
CS assisted in writing and editing
DD assisted in writing and editing
CCB assisted in writing and editing
MM assisted in writing and editing
WC assisted in writing and editing
DC assisted in writing and editing
VA assisted in writing and editing
CTB assisted in study development, data collection, analysis, writing, and editing
Funding Information
This work was supported by Diane N. Weiss and The Sipprelle Family Foundation.
Author Disclosure Statement
DG holds equity in BI Medical, LLC.
NV has no disclosures
AM has no disclosures
SA has no disclosures
CW has no disclosures
BS has no disclosures
EB has no disclosures
CS has stock/stock options in Johnson & Johnson
DD has no disclosures
CCB has no disclosures MM has no disclosures
WC has no disclosures
DC has no disclosures
VA has no disclosures
CTB holds equity in BI Medical, LLC. and in BioIntraface, Inc.