
Abstract
Abstract
Background:
Primary necrotizing fasciitis of the breast is a rare clinical condition and therefore a challenge for the clinical doctor. Its severity is associated with high morbidity and mortality.
Patients and Methods:
In the current article we present three cases that we treated in our surgical department with a combination of empirical antibiotic treatment, complete surgical debridement in stages, and negative pressure wound therapy.
Conclusions:
It appears that prompt diagnosis and surgical intervention are key for the successful management of these cases. The recognition of early clinical signs as well as risk factors are issues of great importance. A high index of suspicion is required for the early diagnosis and treatment, aiming to the best outcome for the patient.
Necrotizing fasciitis in general is a rare yet potentially lethal disease with approximately 500 new cases reported annually in the United Kingdom. 1 It suggests a bacterial inflammation that leads to necrosis of the underlying soft tissues and fascias and is associated with a mortality that approaches 25%.2,3
Necrotizing fasciitis usually appears at the extremities, the abdominal wall, and the perineum. It rarely affects the breast and as a result, there are few cases in the literature. It is usually a consequence of trauma or surgical interventions, yet it can manifest itself in the existence of certain comorbidities.4,5 In the literature, it is usually related to post-operative situations,6–8 contamination of a breast ulcerative lesion,9,10 or core-needle biopsy.11,12 According to a recent review by Konik and Huang 13 only 25 cases of primary necrotizing fasciitis of the breast without any previous intervention were reported in the English language and with complete data, emphasizing the rarity of this clinical entity.
At the onset it can be underestimated or misdiagnosed as an abscess or cellulitis, resulting in delayed diagnosis 14 and therefore increased morbidity and mortality. Three cases of primary necrotizing fasciitis without any history of trauma or surgery that presented to our department are presented. The therapeutic management and final outcome are described.
Patients and Methods
Case 1
The first case concerns an obese (body mass index [BMI], 34 kg/m2), hypertensive, Caucasian female, 47 years old, who presented to the emergency department complaining of pain and inflammation of the right breast for three days. No breastfeeding, trauma, biopsy, or surgical intervention was reported. Mammography and ultrasound performed one year prior revealed no pathology.
On admission, the patient's vitals were stable but she was feverish with a body temperature of 38°C, tachycardia (105 bpm), blood pressure 145/70 mm Hg, and oxygen saturation rate 94%. Physical examination revealed inflammation of the right breast with redness, intense sensitivity during palpation, and painful right axillary lymph nodes.
The patient's laboratory results disclosed leukocytosis (15,000 K/mcL white blood cell [WBC] count, 89% neutrophils), deterioration of kidney function (urea 75 mg/dL and creatinine 2,70 mg/dL; her levels were normal two months ago), hyponatremia 127 mmol/L and hypoalbuminemia 2.7 g/dL. C-reactive protein was 470 mg/L, procalcitonin 23 ng/mL, and erythrocyte sedimentation rate (ESR) 127 mm. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) Score was 11.
Computed tomography of the thorax was performed and showed signs of fat stranding of the right breast with subcutaneous gas and skin thickening, as well as the ambiguity of the borders of the superior thoracic wall and presence of right-sided enlarged axillary lymph nodes with a maximum diameter of 2.5 cm and reactive characteristics (Fig. 1).
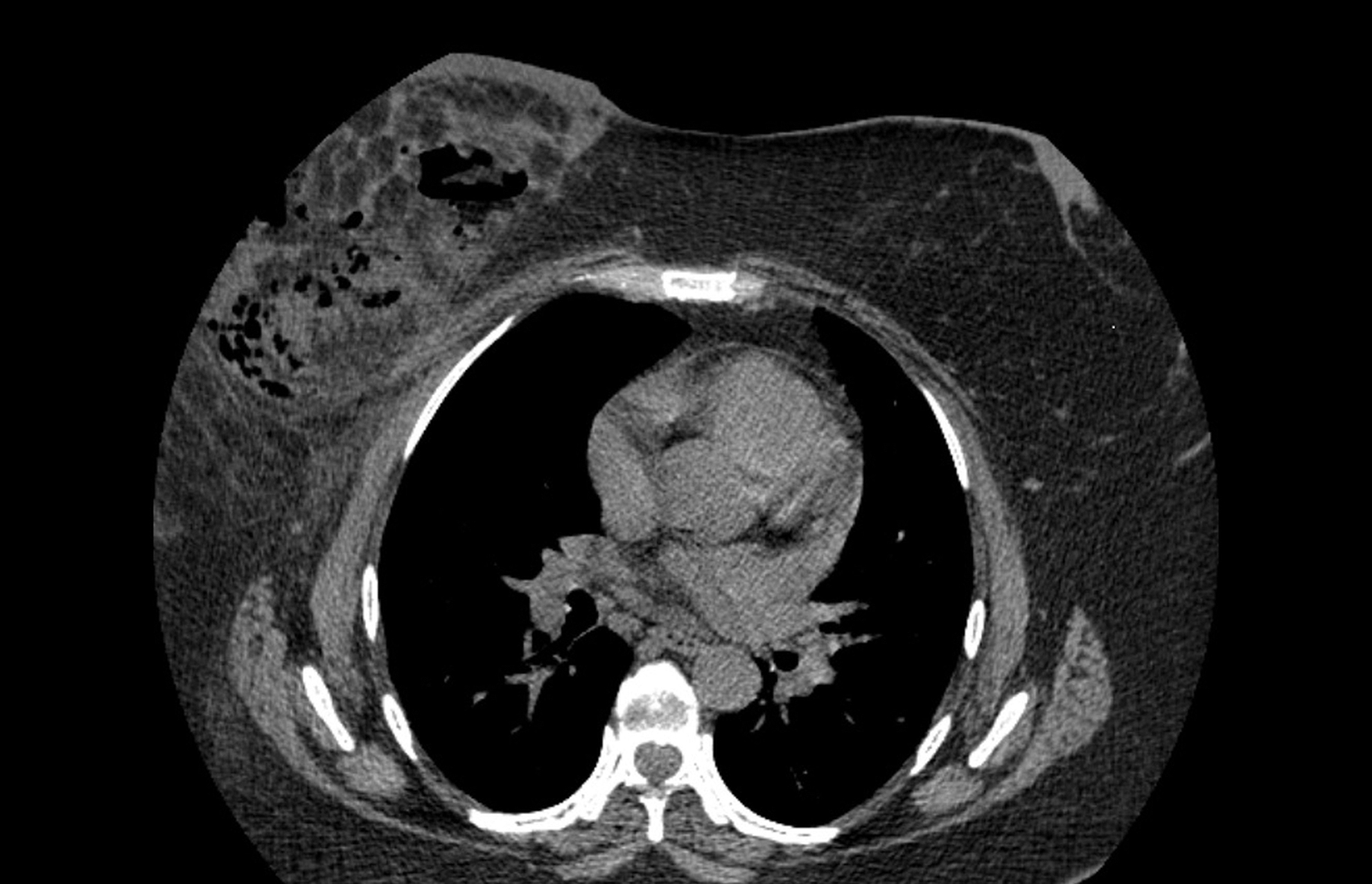
Computed tomography scan: fat stranding of the right breast with subcutaneous gas and skin thickening, ambiguity of the borders of the front thoracic wall.
Immediate resuscitation with fluids and empirical antibiotic treatment with piperacillin-tazobactam and fosamil ceftaroline was began. The patient was taken to the operation room, where necrotizing fasciitis with malodorous fluid outflow were noted. A specimen was collected for culture, and a partial mastectomy (two-thirds of the breast including the nipple) was performed to achieve complete necrosectomy. A whitish formation underneath the areola was detected (Fig. 2) and also removed. A second surgical debridement followed 24 hours later, even though the patient was afebrile. On post-operative day two we initiated vacuum-assisted wound therapy that continued until post-operative day 10. The patient was discharged in excellent condition on post-operative day eight. On post-operative day 20 the incision margins converged. The final cosmetic result was satisfying.
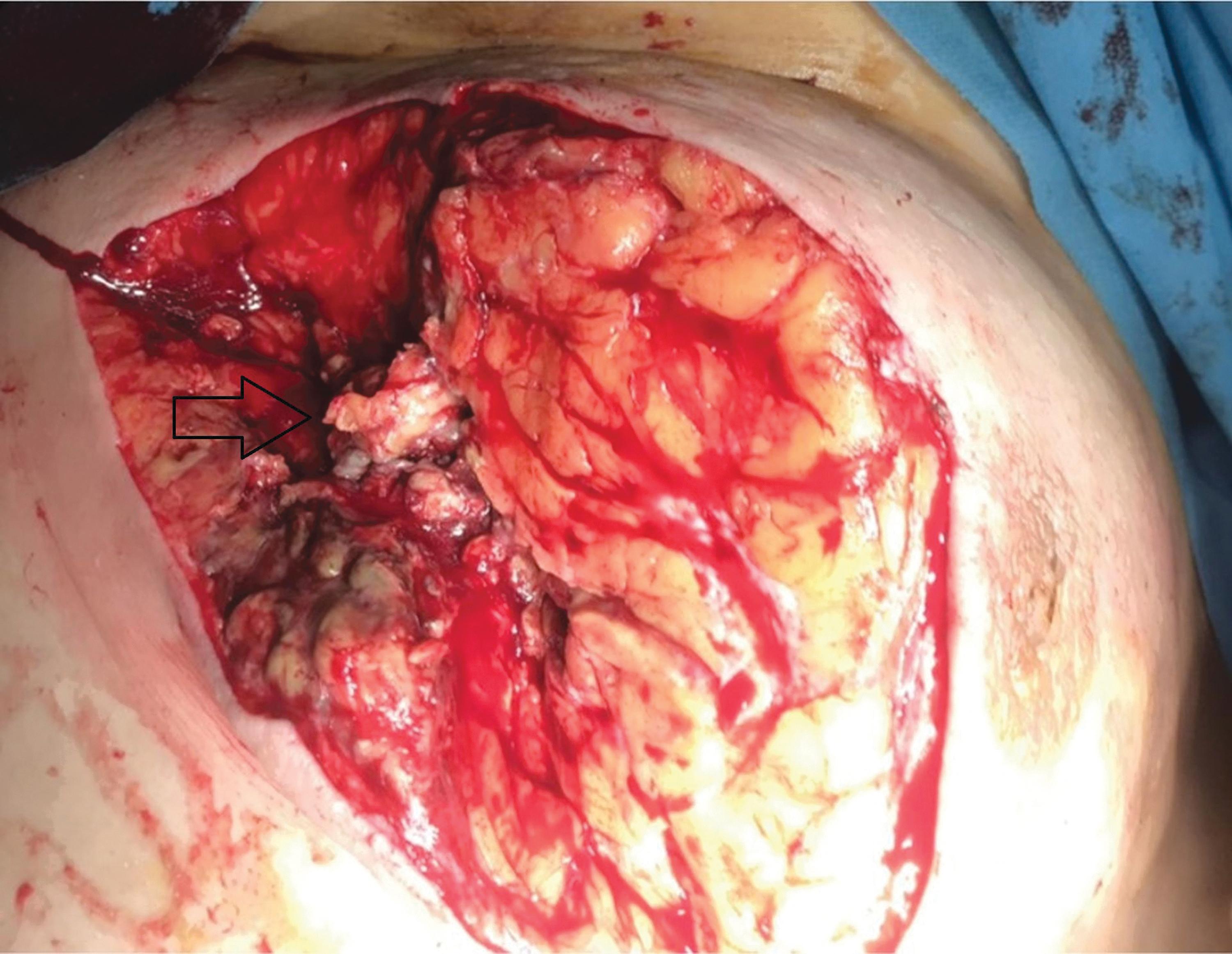
Partial mastectomy, tissue necrosis, and the suspicious formation under the areola (black arrow).
Streptococcus gallolyticus and Streptococcus pasteurianus were isolated from the culture, both sensitive to the initial antibiotic agents. The antibiotic treatment continued orally with clindamycin according to the antibiogram. The pathology report stated necrotic lesions with dense piles of neutrophils and foam mast cells, whereas the formation under the areola was related to sclerosing adenosis with no signs of malignancy.
Case 2
The second case was an obese (BMI 31 kg/m2) 73-year-old Caucasian female, with a history of type 2 diabetes mellitus and hypertension, who presented with inflammation of the left breast that began a week ago, under oral treatment with clindamycin, without clinical improvement.
On admission, she was feverish (38.8°C) and tachycardic (114 bpm), and her blood pressure was 100/80 mm Hg. Clinical examination revealed excessive inflammation of the left breast with redness, necrotic lesions, and malodorous fluid outflow (Fig. 3). The patient's laboratory test results showed leukocytosis up to 21,000 K/mcL WBCs with 88% neutrophils, hemoglobin 9 g/dl, deregulation of her glucose levels up to 350 mg/dL, creatinine 1.8 mg/dL, hyponatremia with sodium 130 mmol/L, and hypoalbuminemia (2 g/dL), C-reactive protein 350 mg/L, and ESR 54 mm. In this case, the LRINEC Score was 12.

Admission day: before the draining and the placement of the Penrose drain.
Aggressive resuscitation with crystalloids was initiated immediately and empirical antibiotic treatment (clindamycin and fosamil ceftaroline) was administrated. The patient was transferred to the operation room, where necrotizing fasciitis among with multiple abscess cavities were detected. Drainage of the abscesses, necrosectomy, and surgical debridement was performed and two Penrose drains were placed in the incisions. A specimen was collected for culture. On post-operative day one the patient remained septic and feverish with clinical deterioration, so a second, more extensive surgical debridement, was performed. However, on post-operative day three the necrosis was expanded (Fig. 4) and it was therefore decided to proceed with complete mastectomy including the extraction of major and minor pectoralis muscles, and a vacuum-assisted closure (VAC) dressing was placed. On post-operative day five the surgical site was inspected under general anesthesia, additional necrosectomies were necessary, and a VAC dressing was applied again.

Expansion of the necrosis on post-operative day three.
Citrobacter koseri and Proteus mirabilis, both sensitive to ciprofloxacin, were isolated from the culture and the antibiotic treatment was adjusted to monotherapy with ciprofloxacin. The patient showed clinical and laboratory improvement. Her glucose levels were well-regulated and renal function was restored. The pathology review reported diffuse acute inflammation and parenchyma necrosis with a large number of bacteria and focal thrombophlebitis, negative for malignancy. The patient was discharged on the fifteenth post-operative day in good condition with oral ciprofloxacin.
During her follow-up period, two VAC dressing changes were necessary, and the patient was referred to plastic surgeons, who performed a breast reconstruction surgery with Latissimus dorsi skin and muscle flap resulting in an excellent cosmetic outcome, as shown in Figure 5.

Reconstruction using a Latissimus dorsi skin and muscle flap, by plastic surgeons.
Case 3
The third case we encountered was a 55-year-old Caucasian woman, obese (BMI, 43 kg/m2), of low socioeconomic status living under inadequate conditions who presented to the emergency department complaining of fever and pain above her left breast lasting three days. Clinical examination revealed inflammation of the upper outer quadrant of her left breast and a temperature of 38.7°C. Regarding her medical history, she had hypertension and hypothyroidism.
The patient's laboratory results on admission included WBCs 15,300 K/mcL with 85% neutrophils, deterioration of kidney function with creatinine 2.75 mg/dL, urea 143 mmol/mL, sodium 131 mmol/L, serum glutamic oxaloacetic transaminase (SGOT) 82, serum glutamic pyruvic transferase (SGPT) 42, and C-reactive protein 533.5 (LRINEC Score 10).
Fluid resuscitation and intravenous broad-spectrum antibiotic treatment (fosamil ceftaroline) were initiated immediately. Under general anesthesia, incisions were made, necrotizing fasciitis was confirmed, surgical debridement until the left axilla was performed, a Penrose drain was placed, and cultures were obtained. The patient was extubated after the surgery but soon presented with respiratory arrest as well as kidney failure. She was re-intubated on the same day and transferred to the intensive care unit. Twenty-four hours later, the surgical site was inspected revealing the expansion of the necrotizing infection. Additional surgical debridement was performed in combination with negative pressure wound therapy. The culture isolated Bacteroides and the patient's antibiotic treatment was modified to piperacillin-tazobactam. Despite this, she remained septic under continuous renal replacement therapy and invasive ventilation. In addition, she developed liver failure and thrombocytopenia. Four days later the patient underwent total mastectomy, further surgical debridement, and VAC wound closure was applied again. No clinical improvement was noted despite the interventions. The patient died seven days later, confirming the life-threatening nature of the disease.
Discussion
Necrotizing fasciitis predominantly manifests at the perineum, the torso, or the extremities, especially in immunosuppressed patients, patients with autoimmune disease treated with steroids and methotrexate, patients with diabetic mellitus, or patients with peripheral vascular disease. Other risk factors include human immunodeficiency virus (HIV), obesity, malnutrition, intravenous drug use, alcoholism, liver cirrhosis, permanent catheters, insect bites, breast implants, mastectomy, lactational mastitis, asthma, and ruptured colorectal tumors.4,15,20–26 Diabetes mellitus is an independent risk factor8,27–29 as is arterial hypertension 28 and obesity.6–8,28 Nevertheless, the cause is undetected in 20%–50% of cases.30,31 In our report, all patients were obese and hypertensive, whereas diabetes mellitus was an additional risk factor in case 2.
Necrotizing fasciitis in general is classified as type 1 and type 2. Type 1 includes multiple bacterial infections and is more common, suggesting 55%–75% of the incidents.15–17 Usually, four different bacteria are isolated on average from the wound culture, including a combination of gram-positive cocci (Staphylococcus aureus, Streptococcus species), gram-negative bacilli (Klebsiella species, Escherichia coli), and anaerobic micro-organisms. Clostridium perfringens has become a rare cause of necrotizing fasciitis due to the improvement of hygiene conditions.18,19
On the contrary, type 2 infections are caused by one bacterial species, usually Streptococcus group A (Streptococcus pyogenes), sometimes in combination with Staphylococcus aureus. 15 They are less common than type 1, and they concern mainly young and healthy patients. History of surgical intervention or trauma often exists. 15 An augmentation in the frequency of methicillin-resistant Staphylococcus aureus incidence in the community was noted lately, mostly affecting alcoholics and athletes. 32
In a recent review by Cai et al., 33 it was noted that Streptococcus pyogenes is the responsible pathogen for 83.3% of the single organism type 2 necrotizing fasciitis of the breast, whereas Staphylococcus aureus was not identified. Another interesting finding is that both type 1 and type 2 breast necrotizing fasciitis might appear primary (50% in type 1 and 55% in type 2), or after breast surgery (31.25% in type 1 and 40% in type 2). Furthermore, type 2 is slightly more common than type 1 (55.6% vs. 44.4%). These results suggest that necrotizing fasciitis of the breast might have a different microbiologic pattern from other necrotizing fasciitis. More studies are needed to understand better the pathogenesis and therefore the microbiologic preference of necrotizing fasciitis of the breast. Regarding our experience, Streptococcus gallolyticus and Streptococcus pasteurianus were isolated at the first case (type 2), Citrobacter koseri and Proteus mirabilis were isolated in the second case (type 1), whereas only Bacteroides was isolated in the third case (type 2).
Necrotizing fasciitis of the breast is a rare and potentially life-threatening condition that is characterized by the rapid expansion of the inflammation, resulting in necrosis of the fascia and the underlying tissues. 27 The thick skin and the subcutaneous tissue may prevent the early recognition of the disease, therefore, delaying the immediate treatment. 33 The accountable bacteria overdevelop and expand rapidly attacking the fascia while producing endotoxins and exotoxins. This procedure evolves to tissue ischemia, liquefactive necrosis, and systemic toxicity. One study supports the theoretical assumption that bacteria infect selectively Cooper's ligament, leading to late skin alterations and relative conservation of superficial and deeper structures. 36 For this reason, high clinical suspicion index is required for the early recognition of this condition.
The clinical presentation includes redness, local inflammation, and pain. The pain is often disproportionate to the clinical findings, which is a warning sign for necrotizing infection. 1 The characteristic skin marks a delayed sign. The redness on the onset may be underestimated as cellulitis. Gradually, the skin color alters into cyanotic and as the necrosis expands, hemorrhagic blisters appear even in the chest and the flank.1,35 Similar clinical signs developed in our cases. Multiorgan failure, including renal or respiratory insufficiency, might also present in the frame of sepsis. A bilateral infection has also been reported.12,20
In 2018, the American Association for the Surgery of Trauma (AAST) created a classification system for breast infection. According to the proposed revised criteria, necrotizing infections of the breast are classified as type 4, indicating the severity of the disease, which is associated with a more aggressive surgical procedure, a longer hospital stay, higher morbidity, and mortality. It suggests a convenient and useful tool for the classification of low to moderate severity infections, to determine in which cases an invasive procedure is necessary, in addition to the antibiotic treatment. However, improvements are needed to be applied in more serious types. 37
The LRINEC Score is another important tool for the detection of even early forms of the disease. The variables taken into consideration are total WBC count, hemoglobin, glucose, creatinine, sodium, and C-reactive protein. 38 A total score is calculated according to the mentioned variables indicating the next step for the therapeutic approach. The cutoff value for the LRINEC Score is six points with a positive predictive value of 92% and a negative predictive value of 96%. The LRINEC Score was calculated at 11 for the first case,12 for the second case, and 10 for the third case, suggesting a high risk of necrotizing fasciitis existence and indicating the need for surgery.
Early aggressive treatment with broad-spectrum intravenous antibiotic agents, complete surgical debridement, and life support in the intensive care unit, if necessary, comprise the cornerstone of the therapeutic approach. The antibiotic treatment should cover gram-positive, gram-negative, and anaerobic micro-organisms. Penicillin, ceftriaxone, cefazolin, clindamycin, and metronidazole, as well as anti-MRSA such as vancomycin are recommended. Surgical debridement must include all of the necrotized tissue, regardless of the expansion. The surgical site should remain open and be inspected daily, whereas surgical debridement is repeated when necessary. A number of interventions may be required in order to control the infection. Fifty-two percent of the patients will eventually require mastectomy (total or radical), followed by serial debridement (32%, with or without nipple-areola sparing), and 16% partial mastectomy 16%. 13 Shah et al. 14 and Ward et al. 39 suggest early surgical treatment for patients with atypical cellulitis disproportionate to the clinical presentation pain, intravenous administration of fluids and antibiotic agents, complete surgical debridement, re-evaluation after 24 hours with a second look operation, and plastic surgery consult for breast reconstruction and better cosmetic outcome. After the acute inflammation passes, reconstruction is usually possible with split-thickness skin grafts or delayed primary closure. Full-thickness skin graft, local tissue rearrangement, negative-pressure wound therapy (VAC), and Latissimus dorsi flap, have also been suggested.13,40 Our first patient was treated with partial mastectomy and delayed primary closure while radical mastectomy and breast reconstruction with a Latissimus dorsi skin and muscle flap was performed to the second one. Both were immediately referred to the surgical department and taken to the operation room two hours later. The final cosmetic result was satisfying.
A negative wound pressure therapy system is a common method of treating extensive tissue deficits after surgical debridement. Its potency is based on the increase of local oxygen concentration and the stimulation of fibroblasts which accelerate the formation of granulation tissue. Although the use of skin grafts demands both skill and experience and burdens the patient with another surgical procedure, negative pressure therapy contributes to second-intention surgical site healing with impressive results proven by studies,19,35,36,41 facilitating the secondary deficit management for plastic surgeons. Nevertheless, there are no well-designed studies evaluating its benefits for patients with sizable wounds as a result of complete surgical debridement because of infection. 42 Furthermore, only two cases of primary necrotizing fasciitis of the breast treated with a combination of hyperbaric oxygen and negative pressure wound therapy are described in the literature, both with successful outcomes, suggesting the need for further studies for the evaluation of the potential benefits of this therapeutic approach.35,43
Different variables are associated with mortality, such as age, 44 septic shock at admission, acute kidney failure, diabetes mellitus, comorbidities, and infections from Clostridium or group A Streptococcus. 45 The only variable proven to consist of an independent prognostic factor is prompt surgical intervention. 15 Wong et al. 31 reported a ninefold increase in mortality if surgical management is delayed more than 24 hours after admission. Flandrin et al. 11 reported a decrease greater than 10% in mortality with early surgery, antibiotic treatment, and intensive care unit support. According to Cai et al. 33 the only determinant mortality factor is the presence of septic shock, whereas the wound/blood culture, the type of the infection, or the operation are not statistically significant. Increased morbidity includes long hospital stay, administration of intravenous and oral antibiotic agents, multiple interventions, post-discharge follow-up visits for dressing changes, and a reconstruction surgery, such as in case 2. However, as proven by case 3, mortality remains high regardless of all the therapeutic strategies, suggesting the severity of this clinical entity.
Conclusions
Necrotizing fasciitis of the breast presents a challenge to surgeons. Because of its rare prevalence and its rapid progress, clinical diagnosis may be delayed resulting in a further increase in morbidity and mortality. The single most important factor in improving outcome is early recognition and complete debridement. Partial or even total mastectomy might be necessary to control the infection. Vacuum-assisted closure therapy also seems to be beneficial. This combination of therapeutic measures aims to the improvement of survival.
Footnotes
Authors' Contributions
Data curation: Symeonidou. Visualization: Symeonidou. Writing–original draft: Symeonidou. Formal analysis: Gkoutziotis. Supervision: Gkoutziotis. Investigation: Moulazimi. Methodology: Moulazimi. Writing–review and editing: Moulazimi. Conceptualization: Lagopoulos. Validation: Lagopoulos. Project administration: Kamparoudis.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors have no conflict of interest to disclose.