
Abstract
Abstract
Background:
To investigate retrospectively whether changes in serum albumin levels within one hour of flexible ureteroscopy (fURS) lithotripsy can be used as a predictor of post-operative urosepsis.
Patients and Methods:
Eligible patients with unilateral upper urinary calculi who underwent fRUS lithotripsy performed by a single surgeon at our center were included in the analysis. The patients were divided into sepsis and non-sepsis groups. The change ratio of albumin and white blood cell (WBC) count was calculated by post-operative/pre-operative index*100%. Univariable and multivariable logistic regression analyses were used to assess whether there was a correlation between risk factors and post-operative urosepsis. The receiver operating characteristic (ROC) curve was used to analyze factors that showed significant differences in multivariable logistic regression analysis.
Results:
A total of 314 patients were included in the analysis, 20 of whom had post-operative urosepsis and five developed septic shock; no deaths occurred. Multivariable logistic regression analysis showed that urine culture results, WBC counts within one hour after surgery, post-operative albumin levels, and the degree of albumin changes after surgery were independent predictors of post-operative urosepsis. Receiver operating characteristic curve analysis showed that noteworthy hypoalbuminemia after surgery and positive pre-operative urine culture could help screen high-risk patients for post-operative urosepsis effectively.
Conclusions:
Hypoalbuminemia shortly after operation can be utilized as a predictor for early diagnosis of post-operative urosepsis in patients undergoing fURS lithotripsy.
Endourologic procedure, encompassing all percutaneous nephrolithotomy (PNL) and ureterorenoscopy (URS) interventions, has become one of the mainstream methods of treating urinary calculi. If active stone removal is indicated, for ureteral stones >1 cm and all kidney stones of all sizes, endourologic procedure can be used as a first-line treatment. 1 However, endourology is associated with some complications. The risk of developing urosepsis after PNL has been reported to range from 0.3%–4.7% of patients, 2 whereas the probability of urosepsis after flexible ureteroscopy (fURS) lithotripsy is approximately 0.06%–7.3%.3,4 As stated in various studies, early identification and suitable management of sepsis can improve the chance of survival.5,6 The concept that sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection is now widely shared, 6 although urosepsis is defined as sepsis caused by a urogenital tract infection.
Albumin is known as a nutritional marker and negative acute-phase protein, decreasing after operation due to surgical stress. Surgeons from different disciplines have reported the prognostic role of hypoalbuminemia in patients undergoing surgery therapy.7–10 Nonetheless, the prognostic significance of the immediate reduction in serum albumin levels after fURS lithotripsy procedure has not been verified. In this retrospective study, we investigated post-operative serum albumin levels and other peri-operative variables as predictors of post-operative urosepsis in patients who underwent fURS lithotripsy.
Patients and Methods
Study population
Eligible patients with urolithiasis who received fURS lithotripsy at the Urinary Stone Treatment Center, Tianjin Medical University Second Hospital from May 2021 to May 2022 were included. Children aged <18 years, patients without records of hematologic and biochemical tests within one hour after surgery, patients with severe liver disease, patients with acute cerebrovascular disease or acute coronary syndrome, and patients with advanced malignant tumor were excluded from the study.
After the exclusion, a total of 314 patients were included in the study. Data were obtained retrospectively from hospital records. Of the included patients, 20 cases were diagnosed with post-operative urosepsis (sepsis group) and 294 were non-sepsis subjects (non-sepsis group).
Peri-operative management
At the time of the initial admission, physical examination, urinalysis, urine culture, blood count, serum biochemical and coagulation tests were performed. Patients who had positive results in the urine culture examination or patients with elevated leukocyte cells in the urine were treated with antibiotic agents pre-operatively. Surgical treatment was not performed until there was a reduction in urinary leukocytes and the urine culture became negative. Patients with negative urine and urine culture results received intravenous empirical antibiotic therapy 30 minutes before surgery. In addition, if the patient had had a fever within half a year before admission, antibiotic agents would be administered intravenously for three to five days before surgery.
The diameter of the ureteral access sheath used during the surgery was 12/14F. The duration of the procedure was limited to 90 minutes. Urologic ultrasound and abdominal radiograph were performed on the first post-operative day for observation of residual calculi.
Definitions
A1 was defined as serum albumin level within one week prior to surgery, whereas A2 was defined as serum albumin level within one hour after surgery. Analogously, W1 was defined as white blood cell (WBC) count within one week prior to surgery and W2 was defined as WBC count within one hour after surgery. A2/A1 and W2/W1 represented the extent of post-operative albumin and WBC count changes compared with pre-operative, respectively. If repeated laboratory tests had been performed before the operation, A1 and W1 were based on the test results closest to the procedure. Post-operative residual stone was defined as stone fragments >4 mm found during urologic ultrasound or abdominal radiograph review on post-operative day one.
Diagnostic criteria for sepsis and septic shock were as follows. 11 The patient's mental state and vital signs were closely observed after surgery, and a Quick Sequential Organ Failure Assessment (qSOFA) score was performed (Table 1). When two of these three qSOFA criteria were met, the possibility of sepsis was considered, and the presence of organ dysfunction was further assessed. Sepsis could be diagnosed if the Sequential [Sepsis-Related] Organ Failure Assessment (SOFA) score (Supplementary Table S1) increased by two or more points from baseline. Septic shock referred to the presence of persistent hypotension on the basis of sepsis and the need for vasoactive drugs to maintain mean arterial pressure (MAP) ≥65 mm Hg and blood lactic acid concentration >2 mmol/L after adequate fluid resuscitation.
qSOFA Criteria
qSOFA = Quick Sequential Organ Failure Assessment Score.
Statistical analysis
SPSS Statistics, version 18 software (SPSS Inc., Chicago, IL) and MedClac version 15.2.2 software were used for the statistical analysis. Numerical data were expressed as mean ± standard deviation, whereas categorical data were indicated as numbers and percentages. The χ 2 test was used to analyze categorical variables, and an independent sample Student t-test was used for numerical variables. A p value of <0.05 was considered statistically significant. The variates with p value <0.2 were subjected to multivariable logistic regression analysis to determine the independent risk factors for urosepsis after fURS surgeries. The predictive efficiency of the multivariable model was evaluated by receiver operating characteristic (ROC) curve analysis. The values on the ROC curve that maximized the area under the curve (AUC) were taken as the cutoff values (i.e., values that have the maximum Youden index), accuracy was calculated with a 95% confidence interval.
Results
The results of univariable analysis
As illustrated in Table 2, female gender (55.0% vs. 31.6%; p = 0.047) and pre-operative fever (20.0% vs. 4.4%; p = 0.017) had substantial influence on the occurrence of post-operative urosepsis. As for the comparison results of laboratory tests (Table 2), urine culture results (40.0% vs. 18.2%; p = 0.038), A2 (31.4 ± 3.6 g/L vs. 37.5 ± 3.8 g/L; p < 0.001), A2/A1 (76.6% ± 5.8% vs. 88.7% ± 8.0%; p < 0.001), W2 (5.0 ± 2.2 * 109/L vs. 6.9 ± 3.7 * 109/L; p = 0.031) and W2/W1 (82.6% ± 30.1% vs. 104.9% ± 60.1%; p = 0.003) were significantly different between the two groups. Infectious calculus (p = 0.058) and age (p = 0.189) were also included in the multivariable analysis.
Results of Univariable Analysis
BMI = body mass index; POD1 = first post-operative day.
p < 0.05.
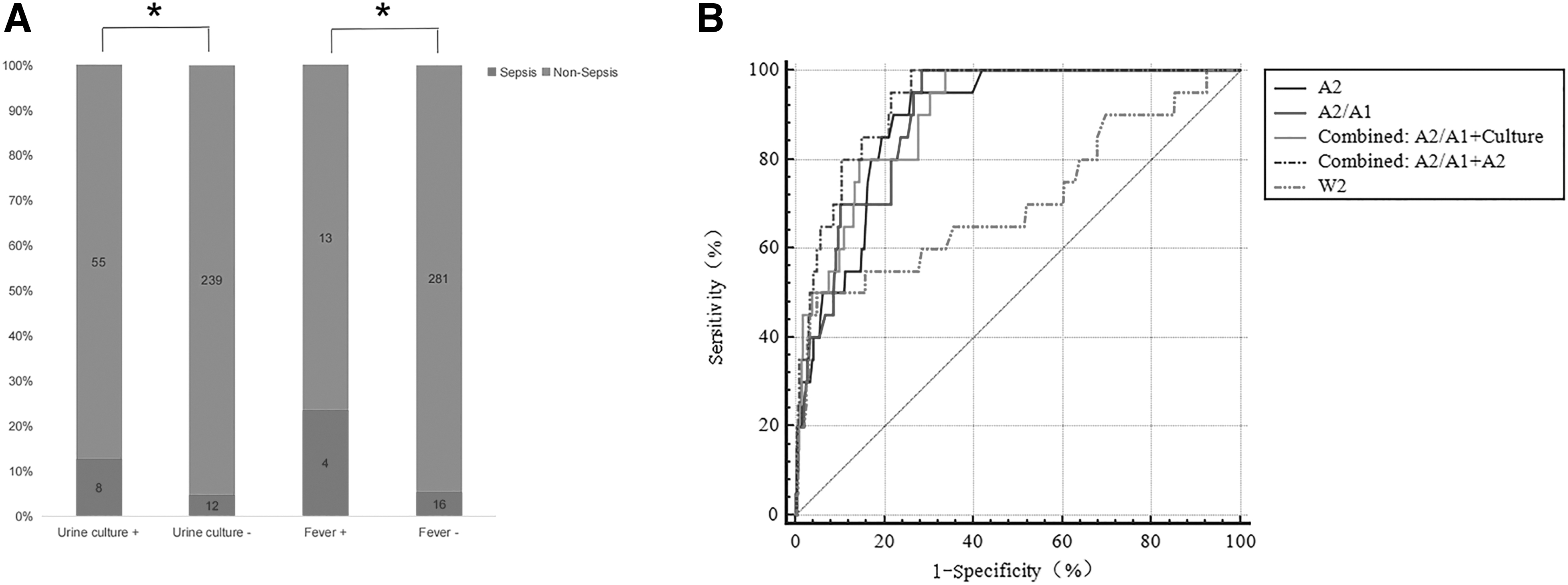
We also analyzed the incidence of urosepsis with/without positive culture and pre-operative fever. As shown in Figure 1A, patients with positive urine culture and a history of pre-operative fever had a higher probability of post-operative urosepsis, validating the results of univariable analysis.
Risk factors associated with post-operative urosepsis
The results of multivariate logistic regression analysis are summarized in Table 3. To provide more information, we also presented the results of the univariable logistic regression analysis (Table 3). Multivariable logistic regression analysis obtained four factors that had substantial influence on post-operative urosepsis, which were urine culture results (odds ratio [OR], 4.667; 95% confidence interval [CI], 1.405–15.499; p = 0.012), W2 (OR, 0.697; 95% CI, 0.480–0.959; p = 0.028), A2 (OR, 0.817; 95% CI, 0.669–0.997; p = 0.047) and A2/A1 (OR, 0.849; 95% CI, 0.769–0.937; p = 0.001).
Results of Univariable and Multivariable Logistic Regression Analysis
OR = odds ratio; CI = confidence interval; A1 = pre-operative albumin level; A2 = post-operative albumin level; W1 = pre = operative WBC count; W2 = post-operative WBC count; POD1 = first postoperative day; WBC = white blood cell.
p < 0.05.
Predictive performance of risk model for post-operative urosepsis
The ROC curve analysis was applied to establish the predictive power of these four independent risk factors for post-operative urosepsis. As demonstrated in Figure 1B, according to the results of multivariable logistic regression analysis, the ROC curves of A2, A2/A1, and W2 were drawn, respectively. In addition, we plotted the ROC curve of combined diagnosis of A2 plus A2/A1 and urine culture plus A2/A1. The specific parameters are shown in Table 4.
Relevant Parameters of ROC Curve
ROC = receiver operating characteristic curve; AUC = area under the curve; A1, pre-operative albumin level; A2 = post-operative albumin level; W1 = pre-operative WBC count; W2 = post-operative WBC count; WBC = white blood cell.
p < 0.05.
The AUC of A2/A1 was 0.895, the cutoff value was 84.2%, the sensitivity and specificity were 0.950 and 0.718, respectively (p < 0.001). The AUC of A2 was 0.890, the cutoff value was 34.85 g/L, the sensitivity and specificity were 0.900 and 0.779 (p < 0.001), respectively. The AUC of W2 was 0.706, the cutoff value was 3.93*109/L, the sensitivity and specificity were 0.500 and 0.952, respectively (p = 0.002), suggesting that W2 was an independent risk factor associated with post-operative urosepsis, but of low predictive performance. The AUC of A2 plus A2/A1 and urine culture plus A2/A1 combined for prediction were 0.929 and 0.900, respectively.
Discussion
In this study, we investigated the prognostic significance of post-operative serum albumin levels and their changes compared with those before operation for predicting urosepsis after fURS lithotripsy. Our observation that serum albumin levels tended to decrease to different degrees in most patients post-operatively is consistent with previous studies.12–14
Some researchers have reported that pre-operative hypoalbuminemia/malnutrition is one of the factors that leads to post-operative complications.14,15 However, these studies did not involve prediction of post-operative complications in patients with normal pre-operative albumin levels, nor did they demonstrate the predictive performance of post-operative laboratory tests results of patients for disease outcome. In fact, even experienced surgeons cannot guarantee that every operation will be performed perfectly, so the impact of operations must be considered. We believe that the post-operative laboratory reports can more accurately reflect the real-time status of patients and the impact of surgery. Wang et al. 9 have also indicated that the extent of albumin declined within two days after surgery could independently predict patients with serious post-operative complications. However, to improve the survival rate and prognosis of patients with sepsis, we need to screen patients at higher risk more quickly. 6
There has been a consensus about the correlation between albumin and inflammatory response. 16 Our data confirmed the decline in albumin levels post-operatively and demonstrated that serum albumin levels within one hour after surgery can be used as a predictor of post-operative urosepsis. If albumin level shows a substantial decrease within this period, clinicians should be highly alert to the occurrence of post-operative urosepsis as well as pay close attention to the changes in conditions of the patients (e.g., blood pressure, consciousness, and urine volume in the short term). This can greatly improve the diagnostic efficiency of post-operative urosepsis. The dilution of plasma albumin through massive transfusion and the extravasation of albumin molecules through permeable capillaries in the vascular system are deemed to be the main causes of post-operative hypoalbuminemia.17–19 In the present study, there is no difference in the amount of fluid input during surgery between the two groups, so the influence of intra-operative infusion volume on the decrease of post-operative albumin can be excluded. Although inflammation can exacerbate capillary permeability and hypoalbuminemia. More severe inflammation is associated with progressively lower serum albumin levels, proinflammatory and inflammatory cytokines, growth factor, nitric oxide (NO), and vascular endothelial growth factor (VEGF) are involved in this process. 16
Several mechanisms may be proposed to explain why a low post-operative albumin level suggests a poor prognosis. First, a low albumin level reflects poor nutritional status, and patients with poor nutritional status are more prone to severe complications after surgery. Second, albumin is considered a negative acute-phase protein. As mentioned above, hypoalbuminemia reflects inflammatory state, and severe hypoalbuminemia can lead to adverse outcomes. 20 In addition, the protective effect of albumin may depend on its other functions partially, such as its capacity to maintain normal colloid osmotic pressure (COP), antioxidant and free radical-scavenging activity, anti-inflammatory capacity, and affinity for binding drugs, toxic substances, and other ligands.21–23
A positive mid-stream urine culture result is direct evidence of urinary tract infection. In the multivariable analysis, urine culture (OR, 4.667) was the strongest predictor, we believe that a positive pre-operative urine culture result indicates a higher risk of post-operative urosepsis. Although the AUC (0.900) was slightly smaller than that in the combined diagnosis of A2/A1 and A2 (Table 4), the combination of A2/A1 and urine culture results still had a good predictive efficiency. Consistent with current opinion, urine culture result is an ideal predictor. Although according to the research reports of Dogan et al., 24 renal pelvic urine and stone culture results were better predictors of post-operative systemic inflammatory response syndrome (SIRS) and sepsis. Unfortunately, the results of these bacterial cultures are often not available before the operation. Pre-operative fever is another established risk factor for post-operative sepsis, but this factor was excluded in the multivariable analysis.
Cannon et al. 25 pointed out that a “drop then rise” phenomenon in serum WBC counts could be observed in patients with serious infection, which suggested a link between decreased WBC count and severe infection. A recent study said that a significant decrease in WBC was associated with septic shock after fURS procedure. 26 The decrease in WBC level is due to endotoxin release into the blood stream and subsequent production of inflammatory factors that activate the systemic inflammatory responses, which then lead to the consumption of WBCs. In addition, the degree of the WBC decrease and the severity of uroseptic shock directly correlated with the concentration of endotoxin. 27 Our data showed that the mean value of W2 (5.0 ± 2.2*109/L) in the urosepsis group was a little less than that of W1 (6.2 ± 1.8*109/L), which indicated that the infection was indeed more severe in this group, but W2 was not a good predictor of post-operative urosepsis. The possible reason for this discrepancy is that peri-operative antibiotic administration and post-operative active intervention may interrupt the progression of infection, or W2 becomes a good predictor only when it drops below a certain level. Thus, WBC has no obvious advantage in fast screening patients who may develop urosepsis post-operatively in our research. Nevertheless, based on the sensitivity of drastic decrease in WBC level to septic shock in the short term after surgery,26,27 we still recommend monitoring this indicator.
To the best of our knowledge, prior to this study there was no research to investigate whether the comparison of pre-operative test results and post-operative test results within one hour after surgery could predict the occurrence of post-operative urosepsis. It provides a different idea for predicting the post-operative urosepsis, allowing clinicians to identify potential critical patients more quickly. Screening with routine test results is also more cost-effective, reducing unnecessary financial burden on patients.
There are several limitations to the present study. First, patients with urosepsis comprise only 6% of the study population, so the number of patients in the urosepsis group was relatively small, with only a few patients with post-operative WBC levels of 4*109/L or below. Furthermore, this research is a single-center retrospective study, therefore large-scale prospective studies and basic research are needed to confirm our findings.
Conclusions
In this study, we analyzed and discussed whether peri-operative laboratory test results and other variables could help urologists more quickly identify patients at high risk for urosepsis after fURS lithotomy. We came to the following conclusions. Positive results of pre-operative urine culture, serum albumin level within one hour after surgery (A2), blood WBC count within one hour after surgery (W2), and the decrease of serum albumin level within one hour after surgery (A2/A1) are independent risk factors for the occurrence of urosepsis after fURS lithotomy. If a patient presents with noteworthy hypoalbuminemia soon after surgery and the pre-operative urine culture result is positive, urologists should be highly vigilant about the post-operative urosepsis.
Footnotes
Acknowledgments
This study was approved by the Ethics Committee of The Second Hospital of Tianjin Medical University (KY2022K095).
Authors' Contributions
Junkai Huang and Linguo Xie contributed equally to this work. Junkai Huang, Yu Yang, and Linguo Xie designed the research and wrote the manuscript. Haijie Xie and Yu Yang collected and analyzed data. Chunyu Liu designed the project and edited the manuscript. All authors approved the final version to be published.
Funding Information
This work was supported by Tianjin Key Medical Discipline (Specialty) Construction Project, Tianjin Health Research Project (TJWJ2022ZD004), The Science and Technology Project of Tianjin (21JCYBJC01300) and Tianjin Health Science and Technology Project (KJ20152).
Author Disclosure Statement
All authors declare no competing interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.