
Abstract
Background:
We aimed to summarize and synthesize the current evidence regarding the indirect impact of the coronavirus disease 2019 (COVID-19) pandemic and its associated measures on the surgical site infection (SSI) rate compared with the pre-pandemic period.
Methods:
A computerized search was conducted on MEDLINE via PubMed, Web of Science, and Scopus using the relevant keywords. Two-stage screening and data extraction were done. The National Institutes of Health (NIH) tools were used for the quality assessment. The Review Manager 5.4.1 program was used for the analysis.
Results:
Sixteen articles (n = 157,426 patients) were included. The COVID-19 pandemic and lockdown were associated with reduced risk of SSIs after surgery (odds ratio [OR], 0.65; 95% confidence interval [CI], 0.56–0.75; p < 0.00001) and (OR, 0.49; 95% CI, 0.29–0.84; p = 0.009), respectively. There was no significant reduction in the SSIs rate after applying the extended use of masks (OR, 0.73; 95% CI, 0.30–1.73; p = 0.47). A reduction in the superficial SSI rate during the COVID-19 pandemic compared with the pre-COVID-19 pandemic period was observed (OR, 0.58; 95% CI, 0.45–0.75; p < 0.0001).
Conclusions:
The current evidence suggests that the COVID-19 pandemic may have some unexpected benefits, including improved infection control protocols, which resulted in reduced SSI rates, especially superficial SSIs. In contrast to extended mask use, the lockdown was associated with reduced rates of SSIs.
Based on the U.S. Centers for Disease Control and Prevention (CDC) definition, surgical site infection (SSI) is “an infection associated with an operative procedure that occurs at or near the surgical incision, within 30 days following the procedure or within 90 days if a prosthetic implant is used during surgery.” 1 Surgical site infections are the most prevalent nosocomial infection and the most common avoidable consequence of surgery.2,3 Nationwide research conducted in the United Kingdom found that the risk of SSIs was 5%, whereas the global estimates showed that SSIs ranged between 3% and 20% of all surgical operations.4,5 Nevertheless, because SSI symptoms sometimes do not present themselves until after patients are released from the hospital, this assessment may be underestimated.6,7 Substantial morbidity is caused by SSIs in surgical patients, extending their hospital stay and increasing the overall costs of treatment.8,9 It has been estimated that the direct expenses of treating a patient with an SSI are approximately double those of treating a patient without an SSI while they are hospitalized. 10 Reducing the rate of SSIs in surgical departments across specialties has traditionally been supported by a firm foundation of appropriate hand hygiene principles and reinforcement of sterility measures throughout in-hospital treatment. 11
In response to the worldwide spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), hospitals had to instantly implement new protocols to protect their staff and patients from being infected with the virus while still providing emergency care and making sure they had enough supplies to treat the unexpected increase in patients with coronavirus disease 2019 (COVID-19) who needed treatment. It has been hypothesized in multiple studies that the overall rate of SSIs after surgery could have been reduced through the strict implementation and repeated reinforcement of sterilization principles during the pandemic.12–15 These principles include increased universal hand sanitization among surgeons, paramedical staff, patients, and their caregivers; near-universal usage of masks; and restriction of crowds in outpatient and inpatient wards. Many studies have investigated the impact of the COVID-19 pandemic and the applied measures on the SSIs rate.16–23 However, these studies were conducted on different populations and surgeries, and some reported conflicting results. Hence, we conducted this systematic review and meta-analysis to investigate the impact of the COVID-19 pandemic on the SSI rate compared with the pre-pandemic period.
Methods
We have followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist and Cochrane Handbook for Systematic Reviews of Interventions in reporting this study.24,25
Eligibility criteria
We included observational studies (case-control, cohort, and cross-sectional) that reported data regarding the SSIs rate during and before the COVID-19 pandemic. In addition, any study that compared the SSIs rate in patients with positive versus negative COVID-19 infection was included. All types of surgeries were included. We excluded case reports and non-English studies.
Information sources and search strategy
On March 1, 2022, we searched the following databases: MEDLINE via PubMed, Scopus, and Web of Science, using the relevant keywords to identify the relevant citations (COVID-19 or SARS-CoV-2 infection or SARS-CoV-2 or 2019 novel coronavirus disease or 2019 novel coronavirus infection or 2019-nCoV disease or COVID-19 virus infection or coronavirus disease 2019 or coronavirus disease-19 or severe acute respiratory syndrome coronavirus 2 or Severe Acute Respiratory Syndrome Coronavirus 2 Infection or SARS coronavirus 2 infection or COVID-19 virus disease or 2019-nCoV infection or COVID 19) and [surgical site infection or infections, surgical wound or surgical wound infections or wound infections, surgical or infection, surgical wound or infection, surgical site or infections, surgical site or surgical site infections or wound infection, postoperative or wound infection, surgical or infection, postoperative wound or infections, postoperative wound or postoperative wound infections or wound infections, postoperative or postoperative wound infection]. These databases were searched from inception to the date of search. Moreover, the reference lists of all included citations were searched. The retrieved citations were imported to EndNote X9 software, and duplicates were removed.
Selection process
Using Microsoft Excel software (Microsoft, Redmond, WA), a screening sheet was created. Study identification, publication year, title, abstract, keywords, DOI, and URL are all included. The selection process was undertaken using a two-step screening technique by three independent reviewers (M.N.A, M.A.A., and A.N.A). Step one was screening the title and abstract of all studies found via the literature search to determine which studies might proceed to step two (full-text screening), in which reviewers would read and assess whether each research met eligibility criteria. Any disagreement between the reviewers was solved by the judgment of the study supervisor (O.A.A).
Data items and collection process
Four independent reviewers (M.A.A., A.N.A., M.O.F., and S.M.A.) extracted the following data from the included studies to an offline pre-prepared Excel sheet: demographic data of the included patients (age and gender), study characteristics (studies groups, study duration, total sample size, country, and main findings), outcomes (SSI and pre-pandemic or post-pandemic infection rate).
Risk of bias and quality assessment
Using the National Institutes of Health (NIH) quality assessment tool for observational cohort, case-control, and cross-sectional studies, two authors (S.M.A. and H.S.A.) independently evaluated the risk of bias and the quality of each included article. Reviewers can critically evaluate the internal validity of research using this tool. Studies were deemed good, fair, or poor. In the case when the authors disagreed on a rating, a third author (O.A.A.) resolved any disagreements.
Data synthesis
The risk of developing SSIs after surgery during or before the COVID-19 pandemic was calculated using the fixed-effect model of odds ratio (OR) with a 95% confidence interval (CI). Using the I2 statistic, we calculated the percentage of heterogeneity and inconsistency between studies, with values of 25%, 50%, and 75% deemed low, moderate, and high, respectively. The random-effect model was used if the heterogeneity was considerable and I2 > 50%; otherwise, the fixed-effect model was utilized. Review Manager 5.4.1. was used for all statistical analyses. To resolve heterogeneity, if present, sensitivity analysis was performed by removing one study in each scenario, which is known as sequential sensitivity analysis. Publication bias was assessed based on the criteria of Egger test, and a funnel plot was generated for the forest plots that included 10 studies or more.
Results
Study selection
Based on our literature search, we found a total of 1,183 relevant citations. After removing duplication, 931 articles underwent title/abstract screening. Then, 902 studies were deemed ineligible to our criteria. The full-text screening was performed on 29 articles, and only 13 studies were excluded. Finally, 16 articles (n = 157,426 patients) were included in the qualitative (systematic review) and quantitative synthesis (meta-analysis).12–23,26–29 Figure 1 shows the PRISMA flow diagram of included studies.

Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram.
Characteristics of included studies and patients
Twelve studies were retrospective, three studies were prospective, and one was cross-sectional. Five studies were conducted in the United States, two in the United Kingdom, and one in the following countries: Brazil, Greece, Germany, Italy, India, Japan, Iran, Mexico, and Switzerland. Almost all studies investigated the impact of the COVID-19 pandemic on the SSIs rate, however, some studies were more specific, e.g., Fraser et al. 19 and Erickson et al. 30 evaluated the impact of extended use of surgical masks during COVID-19 on the SSI rate, Unterfrauner et al. 27 and Losurdo et al. 13 evaluated the impact of COVID-19 lockdown on SSIs rate, and Nachon-Acosta et al. 20 and McLaren et al. 21 evaluated the impact of COVID-19 infection on SSIs rate. Table 1 summarizes the characteristics of included studies.
Summary Characteristics of Included Studies
COVID-19 = coronavirus disease 2019; CLABSIs = central-line–associated blood stream infections; CAUTIs = catheter-associated urinary tract infections; VAEs = ventilator-associated
Events; SSI = surgical site infections; NA = not available.
Pre-COVID-19 cohort sample from Q1 and Q2 2019 only, while the COVID-19 cohort was taken from the whole 2020 year
Quality of the included studies
Based on the NIH quality assessment tool for observational cohort studies, about 66.67% of the studies were deemed as good, and 33.33% of the studies were deemed as fair. In terms of case-control studies, 75% were deemed as good, 16.67% were deemed as fair, and only one study was poor. The quality of the cross-sectional study was good (Fig. 2).
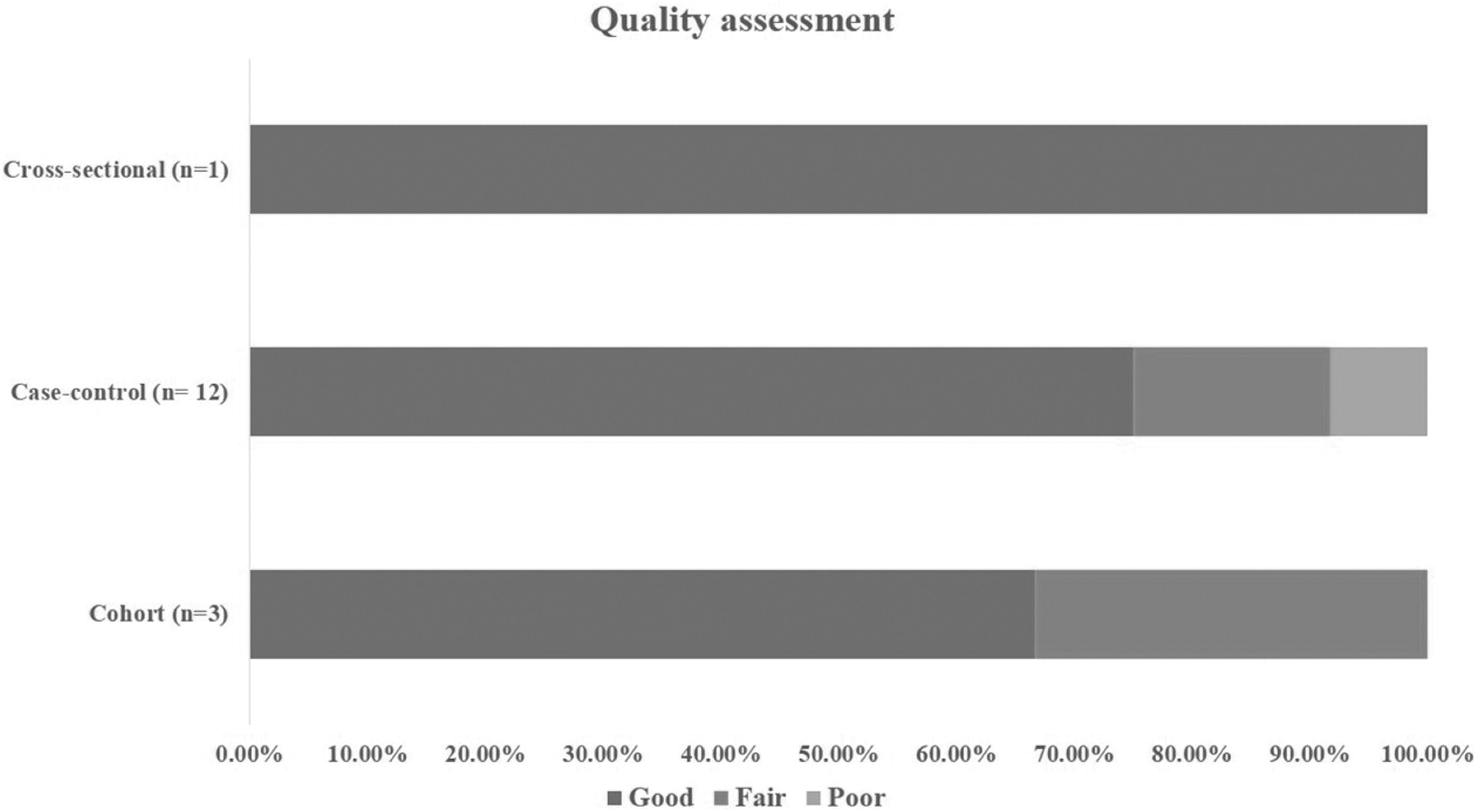
Quality assessment of included studies.
The overall impact of the COVID-19 pandemic on the SSIs rate
A fixed-model pooled analysis of 13 studies showed that the COVID-19 pandemic was associated with a reduced risk of SSIs after surgery (OR, 0.65; 95% CI, 0.56–0.75; p < 0.00001) compared with the pre-COVID-19 pandemic (Fig. 3). The pooled data were homogenous (I 2 , 32%; p = 0.13). Regarding the publication bias, the visual inspection of the funnel plot revealed an asymmetrical figure, suggesting a risk of publication bias (Fig. 4).
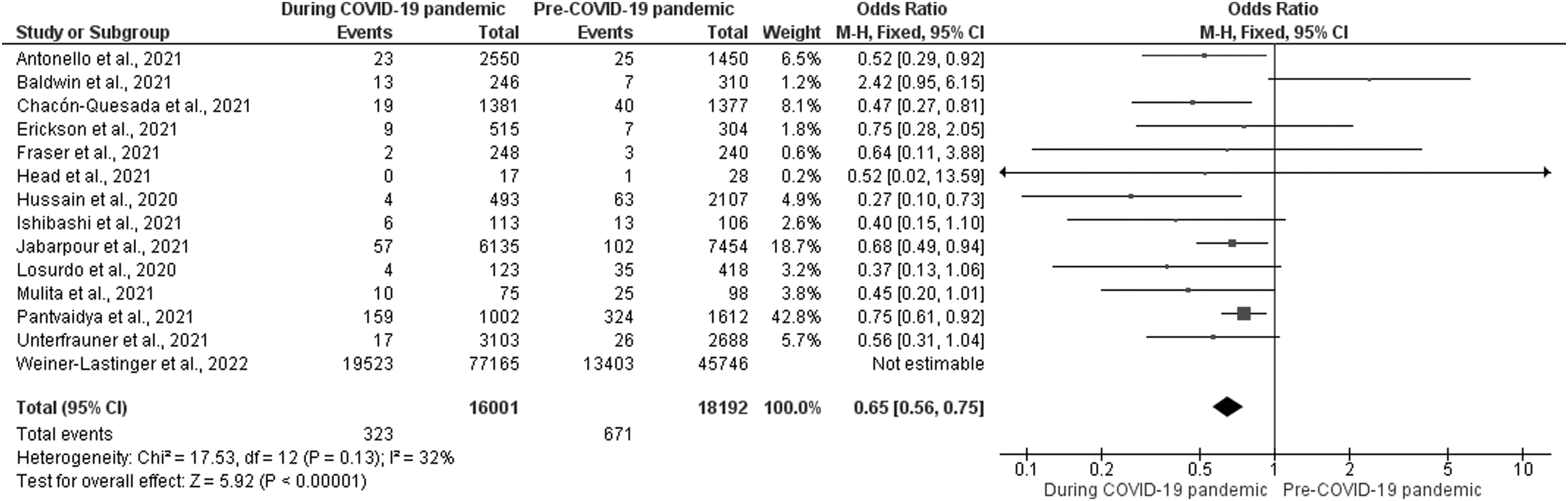
Forest plot of the fixed-effect estimate of the odds ratio (OR) of surgical site infections (SSIs) rate before and during the coronavirus disease 2019 (COVID-19) pandemic.

Publication bias based on funnel plot.
Impact of COVID-19 extended mask use on SSIs rate
The estimated effect size of two studies showed no reduction in the SSIs rate after applying the extended use of a mask during COVID-19 compared with the pre-COVID-19 pandemic period (OR, 0.73; 95% CI, 0.30–1.73; p = 0.47). The pooled data were homogenous (I 2 , 0%; p = 0.88; Fig. 5A).

Forest plot of the odds ratio (OR) of surgical site infections (SSIs) in (
Impact of COVID-19 lockdown on SSIs rate
The estimated effect size of two studies showed that the application of lockdown during the COVID-19 pandemic was associated with a reduction in the SSIs rate compared with the pre-COVID-19 pandemic period (OR, 0.49; 95% CI, 0.29–0.84; p = 0.009). The pooled data were homogenous (I 2 , 0%, p = 0.49; Fig. 5B).
Impact of COVID-19 infection on SSIs rate
The random-model pooled analysis of two studies showed no difference between positive versus negative COVID-19 cases regarding SSIs rate (OR, 1.37; 95% CI, 0.17–11.09; p = 0.77). The pooled data were moderately heterogeneous (I 2 , 68%, p = 0.08). Sensitivity analysis was not applicable (Fig. 5C).
Subgroup analysis according to SSIs type
Superficial SSIs
The estimated effect size of five studies showed a reduction in the superficial SSIs rate during the COVID-19 pandemic compared with the pre-COVID-19 pandemic period (OR, 0.58; 95% CI, 0.45–0.75; p < 0.0001). The pooled data were homogenous (I 2 , 0%; p = 0.41; Fig. 6A).

Forest plots of the odds ratio (OR) of (
Deep SSIs
The random-model pooled analysis of four studies showed a reduction in the deep SSIs rate during the COVID-19 pandemic compared with the pre-COVID-19 pandemic period (OR, 0.44; 95% CI, 0.21–0.96; p = 0.04). The pooled data were heterogeneous (I 2 , 79%; p = 0.003; Fig. 6B). To solve the heterogeneity, a sensitivity analysis was performed. The heterogeneity was resolved by excluding Chacón-Quesada et al. 18 from the analysis (I 2 , 38%; p = 0.20), and the effect estimate has changed to be non-significant (OR, 0.70; 95% CI, 0.43–1.12; p = 0.14).
Organ/space SSIs
The estimated effect size of two studies showed that there was no difference between pre-COVID-19 and during the COVID-19 pandemic in terms of organ/space SSIs rate (OR, 0.99; 95% CI, 0.53–1.83; p = 0.97). The pooled data were homogenous (I 2 , 36%; p = 0.21; Fig. 6C).
Discussion
To combat the SARS-CoV-2 virus transmission among healthcare professionals and patients, surgical departments worldwide have adopted new regulations to permit social distancing, stricter hand hygiene, and universal use of face masks because of the COVID-19 pandemic. Therefore, many studies proposed that the SSIs rate could be reduced as a result of these restricted measures. This systematic review and meta-analysis showed a reduction in the SSIs rate during the COVID-19 pandemic, especially the superficial SSIs. It would be reasonable to believe that near-universal use of face masks, social distancing, and stricter implementation of extended hand hygiene in all personnel involved in patient care helped decrease the incidence of SSIs during the pandemic, even though data from observational studies cannot confirm direct causation.
Pandemic mitigation techniques have also been linked to similar reductions in influenza transmission and hospital-acquired respiratory infections during the COVID-19 pandemic. According to the site involved, various comorbidities, previous therapy received, and the type of surgical wounds, SSI rates for patients undergoing oncologic or gastrointestinal procedures have a broad range reported between 1.4% and 38%.31–34 Prior chemotherapy, radiotherapy, or surgical intervention is an independent predictor of developing SSI in patients who underwent oncologic surgeries.35–37 On the other hand, some studies demonstrated a negative correlation.38,39 A higher risk of SSIs has been linked to longer surgical time and needing to decontaminate previously infected wounds. 40 Multiple investigations failed to find a statistically significant relation between SSI and the use of orthopedic implants, the presence of comorbidities, decreasing hemoglobin or albumin levels, and age. 41
Our findings showed no statistically significant reduction in the SSIs rate after extended surgical mask use during the COVID-19 pandemic. Generally, it is recommended to replace surgical masks after every case for both patient and provider protection. 42 The rapid and major change in operating room policy that necessitates the prolonged use of disposable surgical masks draws attention to the lack of research and literature on the need for infection control linked to surgical mask usage. Changing the policy from one-time usage to extended use has not been supported by evidence. Interestingly, there is a lack of high-quality research demonstrating the advantages of using surgical masks during procedures. There is no evidence that wearing a surgical mask reduces the risk of infection. According to a 2020 meta-analysis of 124 studies, the overall effect of not using face masks was associated with an SSIs risk ratio of 0.77.43,44 However, none of the individual studies exhibited statistically significant outcomes. The SSI rate was not different between masked and unmasked ancillary staff in many investigations. There are no data to support surgical mask usage stratified within each type of case (dirty, contaminated, clean-contaminated, and clean).
Because of the increased SSI risk associated with more advanced classes, most research, including a Cochrane Review (2016), focused primarily on clean patients. 45 Therefore, the generalizability of these investigations to cases that are not considered clean is low. Since the implications of these infections include substantial morbidity and possibly death, subspecialties more prone to place implants, such as cardiac surgery, ophthalmologic surgery, neurological surgery, and orthopedic surgery, are generally excluded from these studies. Using a single mask may not be worth the potential for serious complications or even death from SSIs in certain fields of medicine. Cataract surgery without mask use was associated with a 3.34-fold increased risk of infective endophthalmitis in one case-controlled study. 46 The surgeon's and the medical staff's protection during surgery is another factor to consider when choosing a surgical mask. It is clear that surgical masks protect users from large particles of debris and contaminants, but the absence of protection against micrometer-sized particles, such as bacteria and viruses, remains a real concern. A study of eight different surgical masks found that filter media varies widely in its capacity to prevent the passage of submicrometer contaminants, with results ranging from 20% to 100%. 47
Analysis of nine medical-grade surgical masks showed that none effectively blocked the passage of submicrometer particles into or out of the user's nose, mouth, or eyes. 48 Wearing a mask in the operating room can offer a false sense of security and lead to underreporting of exposures, mostly because it is considered that protection is provided against macroscopic contamination. Furthermore, whether prolonged mask-wearing increases the risk of infection at the surgical site is yet uncertain. Bacterial colonization on the interior of a surgical mask and the exterior surface was evaluated in a study of 40 total joint arthroplasty cases, in which surgeons were classified for operations lasting up to six hours at two-hour intervals. The authors found an increase in bacterial colony-forming units after each two-hour interval, however, they found no increased risk for SSI among all groups at any time interval. 49
Healthcare systems throughout the world are re-assessing their personal protective equipment (PPE) usage strategies because of the COVID-19 pandemic. Extrapolating the decreased need for PPE and operating room time for these instances yielded yearly savings of approximately $3.7 to $4.4 million. 50 These results suggest that the conservation of resources, specifically PPE, may be adopted with minimum impact on patient care and outcomes and may also provide a financial advantage.
Our findings showed that the application of lockdown during the COVID-19 pandemic was associated with an almost 50% reduction in the rate of SSIs. Regarding the impact of lockdown measures such as reduced human contact, increased hand-rubbing, and increased hygiene awareness on SSI, the evidence is sparse, and opinions are conflicting. Restrictions on hospital visitors, decontamination and isolation between patients, shorter hospital stays, fewer personnel on the site during surgery, and increased use of safety clothing and surgical masks all contributed to a decrease in the incidence of SSIs during the lockdown.51,52 According to several infection control teams, there was not enough time for additional preventative packages because of their focus on the COVID-19 pandemic.53,54
Limited or even contradictory evidence for suggested treatments to decrease SSI rates is a common barrier to quality improvement programs aimed at lowering SSI rates. 10 For instance, the relative merits of mechanical vs. oral antibiotic bowel preparation before colorectal surgeries are still up for debate, with contradicting evidence on both sides.55,56 Even when performed according to published evidence, results from surgery are not always satisfying. Preoperative measures, including maintaining a normal body temperature, skin-hair removal, and prophylactic antibiotic use, were the focus of the 2010 Surgical Care Improvement Project, designed to reduce SSIs. 57 There is evidence that these processes are crucial, although a strong correlation between compliance and better results has not been shown.58,59
We acknowledge that our study has some limitations, including the small number of studies in the pooled analyses, the observed publication bias, the high heterogeneity in some comparisons, and the low quality of included studies, as most of them were retrospective studies. Overall, the main source of heterogeneity in the included studies could be attributed to the different evaluated populations, as some studies included the pediatric population, which has a relatively low rate of SSIs compared with adults. In addition, the different types of surgery, such as general, oncologic, neurologic, and emergent abdominal surgeries, were another source for this heterogeneity.
Regarding the heterogeneity in the deep SSIs comparison, we solved it by excluding the study of Chacón-Quesada et al. 18 This study showed a higher reduction in the deep SSIs rate compared to Unterfrauner et al. 27 and Pantvaidya et al. 26 This reduction was attributed to the different measures applied in these studies; Chacón-Quesada et al. 18 applied different measures, including contact reduction with medical and non-medical staff, visit restriction by non-medical/care-associated personnel, and continuous use of disposable surgical masks or filtering face piece (FFP)-2 masks by all staff and visitors. On the other hand, the other studies investigated only the role of lockdown in addition to the conventional methods applied in the surgical room on the rate of deep SSIs. During the literature search process, we excluded non-English articles, which could be regarded as another limitation.
In conclusion, the evidence suggests that the COVID-19 pandemic may have unexpected benefits, including improved infection control protocols, which resulted in reduced SSI rates, especially superficial ones. In contrast to extended mask use, the lockdown was associated with reduced rates of SSIs. Therefore, we recommend establishing a protocol for managing this critical point by implementing a number of measures, including contact reduction with medical and non-medical staff, visit restriction by non-medical/care-associated personnel, and continuous use of disposable surgical masks or FFP-2 masks by all staff and visitors.
Footnotes
Acknowledgments
We would like to thank Noha Farouk Tashkandi and her program Research Platform for their efforts in facilitating the process of this research.
Authors' Contributions
Conceptualization: Alaidaroos. Methodology designing: Almuhaydib, Alaidaroos, Alshammary. Searching databases: Aldossari, Alowid. Screening: Almuhaydib, Alhossan, Aldossari. Data extraction: Alhossan, Aldossari, Fallatta, Alotaibi. Quality assessment: Alotaibi, Alshammary. Data analysis: Salem, Fallatta, Almuhaydib. Writing–original draft: Almuhaydib, Alhossan, Aldossari, Fallatta, Alotaibi, Alowid. Writing–review and editing: Alaidaroos, Salem, Alsaygh, Alshammary. Supervision: Alaidaroos. Submission and follow-up: Alaidaroos.
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.